Assessment and Evaluation of a Crosswalk Between the Functional Independence Measure
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Design of Senior Family Bathroom System Based on Demand Theory
E3S Web of Conferences 179, 02080 (2020) https://doi.org/10.1051/e3sconf/202017902080 EWRE 2020 Design of Senior Family Bathroom System Based on Demand Theory Rong Han1, Dandan Shao2*and YuXin Wang 3 1 College of Art, Jiangsu University, Zhenjiang City, Jiangsu Province,212000, China 2 College of Art, Jiangsu University, Zhenjiang City, Jiangsu Province,212000, China 3 College of Art, Jiangsu University, Zhenjiang City, Jiangsu Province,212000, China Abstract. Aiming at the characteristics of the elderly population, based on the demand theory, this paper proposes a design scheme of a suitable family bathroom system. Based on the theory of Maslow's demand theory, understand the real psychological status of the elderly through theoretical transformation, analyze the physical and psychological characteristics of the elderly, and simulate the specific behavior of the elderly in the bathroom space system through user interviews. In response to the elderly's needs for the space, facilities and supporting facilities of the bathroom system, a type of bathroom space was finally selected to carry out the design practice, which provided certain theoretical support and practical reference value for the subsequent research of bathroom products for the elderly. them focus on the general analysis of the product size and lack the corresponding in-depth exploration. At 1 Introduction present, there are many plagiarism products in the Since 2000, China has begun to enter an aging society. bathroom market and lack of innovative design. The Population aging is an inevitable trend in social design of home bathroom systems based on the theory of development and a hot topic in the world today (as needs is a targeted, humanized adjustment and change shown in Figure 1). -

Potty Training: NASA Tests New $23M Titanium Space Toilet 1 October 2020, by Marcia Dunn
Potty training: NASA tests new $23M titanium space toilet 1 October 2020, by Marcia Dunn the shakedown goes well, the toilet will be open for regular business. With SpaceX now launching astronauts to the space station and Boeing less than a year from sending up its first crew, more toilets are needed. The new one will be in its own stall alongside the old one on the U.S. side of the outpost. The old toilets cater more toward men. To better accommodate women, NASA tilted the seat on the new toilet and made it taller. The new shape should help astronauts position themselves better for No. 2, said Johnson Space Center's Melissa McKinley, the project manager. In this June 18, 2020 photo provided by NASA, astronaut Kate Rubins, center, and support personnel review the Universal Waste Management System, a low- gravity space toilet, in Houston. The new device is scheduled to be delivered to the International Space Station on Oct. 1, 2020. (Norah Moran/NASA via AP) NASA's first new space potty in decades—a $23 million titanium toilet better suited for women—is getting a not-so-dry run at the International Space Station before eventually flying to the moon. It's packed inside a cargo ship that should have blasted off late Thursday from Wallops Island, Virginia. But the launch was aborted with just two minutes remaining in the countdown. Northrop Northrup Grumman's Antares rocket is poised for launch at the NASA Wallops test flight facility Thursday, Oct. 1, Grumman said it would try again Friday night if 2020, in Wallops Island, Va. -
Beavers Space Badge What to Do Next…
Beavers Space Badge What to do next… There are still some things to do before you gain your space badge. These sheets should help you work out what you’ve done and what you still need to do. To gain your Beaver Space Badge you must do all these things: 1. Identify some of the things you can see in the night sky, for example stars, planets and the Moon. 2. Be able to name the eight planets in our solar system. 3. Identify at least one constellation you can see. 4. Find out about a current space mission 8 1 Activity 1 - Identify some of the things you Activity 2 - Identify the planets in our solar can see in the night sky system Cut out the names below and stick them on page 3 You will have: been introduced to the Moon in our planetarium. You should know that the Moon doesn’t make its own light, but Jupiter Neptune reflects the light of our Sun. This is why the Moon has phases. Mars What to do: Venus Saturn What can you see in the sky? What can you see during the daylight? What can you see at night? Uranus Mercury Earth What can you see in daylight and at night? Activity 4 - Find out about a space mission Draw a circle round the things you can see in the night sky. We live in an exciting time with a number of major space missions happening over the next few years. Here are just a few: Rosetta- Comet Chaser- The first probe to land on a comet. -
Grade 6 Science - Unit Lesson Guide
Anglophone School District - North Grade 6 Science - Unit Lesson Guide Space 1 Table of Contents Scientific Literacy!!!!!!!!!!3 Science Assessment Overview!!!!!!!!4 Focus and Context!!!!!!!!!!5 Unit Instructional Overview!!!!!!!!!6 Table - Space - Curriculum Outcomes!!!!!!!7 Strand 1 Space Exploration!!!!!!!! 8 Life of an Astronaut!!!!!!!!!!9 Examining Astronauts!!!!!!!!!10 Current Issues in Space!!!!!!!!!12 Strand 2 - Relative Position and Motion of the Earth, Moon, and Sun !! 13 Access Prior Knowledge !!!!!!!!!15 Cycle 1 - Movement of the Earth and Sun Activity!!!!!18 Cycle 2 - Day and Night Activity !!!!!!!!22 Cycle 3 - Seasons Activity and Discussion!!!!!!25 Day, Night, and Seasons - SPARK !!!!!!!30 Cycle 4 - Sun Shining on the Moon Activities (moon phases)!!!!33 Strand 3 - Strand - The Solar System!!!!!!! 41 Activity - Build a Model of the Solar System!!!!!!42 Activity - Studying Components of the Solar System!!!!!44 Strand 4 - Strand - Stars and Constellations!! ! ! ! ! 48 Activity - Understanding Constellations!!!!!!!49 Activity - Cultural Significance of Stars!!!!!!!50 2 The Aim of Science Education - Scientific Literacy The aim of science education in the Atlantic Provinces is to develop scientific literacy. Scientific Literacy is an evolving combination of the science-related attitudes, skills, and knowledge students need to develop inquiry, problem-solving, and decision-making abilities; to become lifelong learners; and to maintain a sense of wonder about the world around them. To develop scientific literacy, students require diverse learning experiences that provide opportunities to explore, analyze, evaluate, synthesize, appreciate, and understand the interrelationships among science, technology, society, and the environment. The Three Processes of Scientific Literacy An individual can be considered Scientifically Literate when he/she is familiar with, and able to engage in, three processes: Inquiry, problem solving, and decision making. -

A Syntactic Analysis of Spatial
A SYNTACTIC ANALYSIS OF SPATIAL CONFIGURATION TOWARDS THE UNDERSTANDING OF CONTINUITY AND CHANGE IN VERNACULAR LIVING SPACE: A CASE STUDY IN THE UPPER NORTHEAST OF THAILAND By NOPADON THUNGSAKUL A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY UNIVERSITY OF FLORIDA 2001 Copyright 2001 by Nopadon Thungsakul I dedicate this study to my family with love and gratitude and to my professors with profound respect. Completing this dissertation is truly beneficial to me, and I feel privileged to have been given this opportunity. ACKNOWLEDGMENTS I would like to express my appreciation and gratitude to a number of people who have been helpful in contributing to the completion of this dissertation. My chairperson, Wayne Drummond, Professor of Architecture, University of Nebraska-Lincoln, has generously shared his knowledge and experience in directing this research and provided valuable advice. My cochairperson, Dr. Diana H. Bitz, Associate, Professor of Architecture, and my committee members: Dr. H. Russell Bernard, Professor of Anthropology, Maelee T. Foster, Professor Emerita of Architecture, and Peter E. Prugh, Associate Professor of Architecture, inspired me in different ways. Their encouragement and support have made my school years a truly enjoyable experience. The opportunity to work with them and to benefit from their deep knowledge and varied viewpoints has been a valuable experience in my academic career. I am grateful to the Thai Government for generous financial support throughout the years of my graduate studies. Having the opportunity to study abroad has been a memorable learning experience and a wonderful period in my life. -
Surviving in Space
In This Guide What does the future hold for humans and space travel? Space is a one-of-a-kind exhibition that seeks to answer that question and more by exploring the challenges of living and working in space. Unlike traditional space exhibits that focus on the history of space travel, Space looks into current and future exploration. Take a journey to space through interactive exhibits, whole body experiences, and authentic artifacts that will engage you and your students with the unparalleled adventure of human space exploration. Your students will have the opportunity to: 1. Immerse themselves in the sights, sounds, and smells that astronauts experience while traveling and living in space; 2. Engage as problem solvers with some of the unique engineering challenges that must be solved to support living and working in space; TABLE OF CONTENTS 3. Experience what life is like in space through the voices of engineers, scientists and astronauts. In This Guide . 1 Space was produced in partnership with the International Space Exhibition Overview . 3 Station Office of NASA’s Johnson Space Center, the California Misconceptions About Space . 6 Science Center and the partner museums of the Science Museum Exhibit Collaborative. Connecting with the Classroom Pre-Visit . 11 Special thanks to Minnesota teachers who served as Guide advisors: Jill Jensen, Kim Atkins, Dee McLellan, Lynn Spears, Post-Visit . .16 Kate Watson, Brandi Hansmeyer. At the Museum Chaperone Guide . .22 Grades K–2 . .23 Grades 3–5 . .25 Grades 6–8 . .27 Grades 9–12 . 29 Resources for Teachers & Students . 31 Next Generation Science Standards . .33 Surviving in Space . -

Map & Guide Layout
Education Tips for your visit About Space Center Houston The Learning Space Start your visit by making sure you have timed tickets to see Discover the excitement and the shuttle in Independence Plaza and the NASA Tram Tour. wonders of space exploration More than 100,000 teachers and students from around the Timed tickets are available while at our center by going on our at Space Center Houston. world visit Space Center Houston annually to take part in website to spacecenter.org/nowait or visiting the timed ticket extraordinary learning opportunities. station near the Membership Desk. Owned by the 501(c)(3) nonprofit Manned Space Flight Education • Space Center University Next, go to Destiny Theater to see the signature film, Human Foundation, Space Center • Educator Resource Center Destiny, which explains many of the artifacts you will see. Houston is a space and science • School trips and overnight visits Exit the back of the theater to explore Starship Gallery, museum with an extensive • Virtual field trips through distance learning where you can see flown spacecraft and touch a lunar rock. science education program. • Day camps for children ages 4-14 • Camp-ins for Scouts Don’t forget to catch the three live shows and other films Space Center Houston is the • An annual educators conference on the present, past and future of human space exploration. Official Visitor Center of NASA Johnson Space Center and Visit the Information Desk or spacecenter.org/education Want to get even more out of your visit? Stop by the Informa- Houston’s first and only for more details. -

Editorial Comment
26. Carter L, Pruitt J, Brown CA, et al. Status of ISS water management odiferousIn-Flight Maintenance of a previously utilized Waste and recovery. Paper presented at: 46th International Conference of Collection System onboard orbiter Atlantis, during STS-46, by Environmental Systems. Vienna, Austria 2016. the first Swiss ESA astronaut, Claude Nicollier. There was also 27. Kayatin MJ, Pruitt JM, Nur M, Takada KC, Carter L. Upgrades to a space toilet scandal on ISS in 2007 when, after several failed 47th Inter- the International Space Station Water Recovery System. attempts of their own, NASA bought a Russian toilet for national Conference on Environmental Systems. Charleston, South $19 million to install in the US segment, but would not let Carolina 2017. 28. Feltman R. Why American astronauts drink Russian urine. Russian crew members use it. In 2018, that very toilet broke https://www.washingtonpost.com/news/speaking-of-science/wp/2015/ and US crew members had to borrow the Russian segment toi- 08/27/why-american-astronauts-drink-russian-urine/. Published let while asking RSS Energia for repair parts. 2015. Accessed. Although, the device worn in NASA’s Launch and Entry and 29. Duchesne SM, Tressler CH. Environmental Control and life Extravehicular Activity space suits-the Maximal Absorbency support integration strategy for 6-crew operations. 40th Interna- Garments, aka “space diapers” were made famous for a “discom- tional Conference on Environmental Systems. Barcelona, Spain moding” reason, this technology reduced the morbidity of many 2009. with earthbound incontinence; just as much of spaceflight tech- nology has improved the lives of terrestrial people worldwide. -

DOWNTOWN PUBLIC TOILET FACILITIES PROJECT TEAM RECOMMENDATIONS June 13, 2019
DOWNTOWN PUBLIC TOILET FACILITIES PROJECT TEAM RECOMMENDATIONS June 13, 2019 1. Project Background and Description Project Mission: Explore the issue of Downtown public toilet facilities in Chapel Hill. This document outlines beneficial bathroom locations, attributes and recommendations to be used by the Town, its partners and private property stakeholders as future development is considered in Downtown. Downtown Chapel Hill is an economic driver and public cultural center of Chapel Hill, a key visitor and family location of interest, and a heavily used corridor for the UNC community. To attract and retain a diverse set of visitors to the Downtown, it must include toilets available to all. Public toilets serve a community good and thus are a worthy investment of public and private funds. Among other avenues, this interest arose during the Spring 2018 Downtown Work Plan public input process after which a team was formed of community stakeholders to explore the issue, test possible solutions, and create a formal set of recommendations for the future. The Downtown Public Toilet Team (“Team”) focused on the vicinity of the Franklin and Columbia Street intersection due to this area being the highest foot traffic and the most significant amount of visitors and events. Team members met from late 2018 to early 2019 and include the following: Name Title Organization Aaron Executive Director, Off-Campus UNC Bachenheimer Student Life and Community Partnerships Chief Chris Blue Police Chief Town of Chapel Hill Tina Fuller Social Media Coordinator -

Developing Exploration Technologies on the ISS: Exploration Toilet Challenges October 17, 2019
National Aeronautics and Space Administration Developing Exploration Technologies on the ISS: Exploration Toilet Challenges October 17, 2019 James Broyan | AES Logistics Reduction Project Manager | Crew and Thermal Systems Division | JSC Introduction • The Waste Collector System (WCS) is unglamorous but essential • WCS defined as collection of urine, menstrual, and fecal waste • Unsuccessful WCS operation impacts crew performance • Crew cabin surfaces, clothing, crew and air become fouled resulting in unhygienic and noxious conditions • Ineffective processing/storage of waste impacts the vehicle • Precipitates/growth can foul urine vents or processing equipment • Fecal/urine gas generation (e.g. ammonia) can impact CO2 removal and trace contaminant control systems 2 Why WCS Hardware is Difficult? • Human to hardware interface is critical • Variability in crew body contours and crew positioning during use • Difficult to separate waste from body • Surface tension dominates • Water unavailable for waste transport from use area once separated • WCS development relative to vehicle development • Generally given inadequate consideration early in vehicle design • Vehicle mass and volume constraints compromise WCS functionality • Difficult to verify and validate hardware performance • Lack of adequate urine and fecal simulates and delivery systems • Ground tests inadequate and parabolic aircraft flights too short • Require multiple space flights to discover and resolve performance 3 Space Toilet Historical Experience • 6 US and 3 Russian toilets have flow but inclusive hygienic collection is still elusive (2007-01-3227) • Have worked well for some but not for all crew • Challenges for dual urination and defecation – more compatible for males • Escapes of urine and feces • Odor control of stored waste • Frequent component changeout 4 Space Toilets have continued to evolve Apollo 10 Lunar Lander transcript pilot Cernan: “Here’s another goddam turd. -

Designing Public Restrooms
This Online Learning Seminar is available through a professional courtesy provided by: Designing Public Restrooms Hadrian Inc. 7420 Clover Avenue Mentor, OH 44060 Tel:440-942-9118 Fax:440-942-9618 Toll-Free:1-800-536-1469 Email: [email protected] Web: www.hadrian-inc.com Getting Started Click on the start button to START begin this course START ©2007 Hadrian Inc. The material contained in this course was researched, assembled, and produced by Hadrian Inc. and remains their property. ‘LEED’ and related logo is a trademark of the U.S. Green Building Council and used by permission. Questions or concerns about the content of this course should be directed to the program instructor. powered by ©2007 Slide 1 of 63 • About the Instructor • About the Sponsor • Ask an Expert Designing Public Restrooms Presented By: Hadrian Manufacturing Inc. 965 Syscon Road Burlington, ON L7L 5S3 Description: Provides an overview of public washroom design including fixture counts, partition choices, accessibility and sustainable options. To ensure the accuracy of this program material, this course is valid only when listed on AEC Daily's Online Learning Center. Please click here to verify the status of this course. If the course is not displayed on the above page, it is no longer offered. The American Institute of Architects · Course No. AEC234 · This program qualifies for 1.0 HSW/LU hour. AEC Daily Corporation is a Registered Provider with The American Institute of Architects Continuing Education Systems (AIA/CES). Credit(s) earned on completion of this program will be reported to AIA/CES for AIA members. -
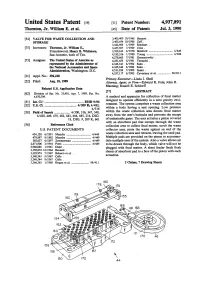
Valve for Waste Collection and Storage
United States Patent 1191 [113 Patent Number: 4,937,891 Thornton, Jr. William E. et al. [45] Date of Patent: Jul. 3.1990 VAL= FOR WASTE COLLECI'ION AND 3,405,409 10/1968 Bennett . STORAGE 3,405,454 10/1968 Zeff . 3,422,985 1/1969 Rinehart . Inventors: Thornton, Jr. William E., 3,457,567 7/1969 Criss . Friendswood; Henry B. Whitmore, 3,522,613 8/1970 Botsford ................................. 4/49 San Antonio, both of Tex. 4,185,336 1/1980 Young ..................................... 4/286 4,276,663 7/1981 Gensurowsky . Assignee: The United States of America as 4,281,655 8/1981 Terauchi . represented by the Administrator of 4,345,341 8/1982 Saito . the National Aeronautica and Space 4,345,342 8/1982 Saito . Administration, Washington, D.C. 4,531,939 7/1985 Izumi . 4,537.1 17 8/1985 Cavestany et al. .................. 98/39.1 Appl. NO.: 392,228 Primary Examiner-Linda J. Sholl Filed Aug. 10,1989 Attorney, Agent, or Firm-Edward K. Fein; John R. Manning; Russell E. Schlorff Related US. Application Data 1571 ABSTRACT Division of Ser. No. 35,401, Apr. 7, 1989, Pat. No. 4,870,709. A method and apparatus for collection of fecal matter designed to operate efticiently in a zero gravity envi- (3.5 E03D 9/04 Int. ................................................ ronment. The system comprises a waste collection area U.S. c1. ....................................... 4/209 R; 4/482; 4/316 within a body having a seat opening. Low pressure Field of Search ................... 4/300, 316, 347, 348, within the waste collection area directs fecal matter 4/420,449,479,482,483,484,485,216, DIG.