'Acute Leukemia in Congenital Methehemoglobinemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Section 8: Hematology CHAPTER 47: ANEMIA
Section 8: Hematology CHAPTER 47: ANEMIA Q.1. A 56-year-old man presents with symptoms of severe dyspnea on exertion and fatigue. His laboratory values are as follows: Hemoglobin 6.0 g/dL (normal: 12–15 g/dL) Hematocrit 18% (normal: 36%–46%) RBC count 2 million/L (normal: 4–5.2 million/L) Reticulocyte count 3% (normal: 0.5%–1.5%) Which of the following caused this man’s anemia? A. Decreased red cell production B. Increased red cell destruction C. Acute blood loss (hemorrhage) D. There is insufficient information to make a determination Answer: A. This man presents with anemia and an elevated reticulocyte count which seems to suggest a hemolytic process. His reticulocyte count, however, has not been corrected for the degree of anemia he displays. This can be done by calculating his corrected reticulocyte count ([3% × (18%/45%)] = 1.2%), which is less than 2 and thus suggestive of a hypoproliferative process (decreased red cell production). Q.2. A 25-year-old man with pancytopenia undergoes bone marrow aspiration and biopsy, which reveals profound hypocellularity and virtual absence of hematopoietic cells. Cytogenetic analysis of the bone marrow does not reveal any abnormalities. Despite red blood cell and platelet transfusions, his pancytopenia worsens. Histocompatibility testing of his only sister fails to reveal a match. What would be the most appropriate course of therapy? A. Antithymocyte globulin, cyclosporine, and prednisone B. Prednisone alone C. Supportive therapy with chronic blood and platelet transfusions only D. Methotrexate and prednisone E. Bone marrow transplant Answer: A. Although supportive care with transfusions is necessary for treating this patient with aplastic anemia, most cases are not self-limited. -

A Case of Hemolysis and Methemoglobinemia Following Amyl Nitrite Use in an Individual with G6PD Deficiency
Available online at www.sciencedirect.com Journal of Acute Medicine 3 (2013) 23e25 www.e-jacme.com Case Report A case of hemolysis and methemoglobinemia following amyl nitrite use in an individual with G6PD deficiency Anselm Wong*, Zeff Koutsogiannis, Shaun Greene, Shona McIntyre Victorian Poisons Information Centre, Austin Hospital, Heidelberg 3084, Victoria, Australia Received 28 August 2012; accepted 26 December 2012 Available online 5 March 2013 Abstract A 34-year-old man presented feeling generally unwell with dark urine 3 days after inhaling amyl nitrite. His initial heart rate was 118/min, blood pressure 130/85 mmHg, O2 saturation 85% on 15 L/min oxygen, and Glasgow coma score 15. He was pale, with clear chest sounds on auscultation. His hemoglobin was 60 g/L, bilirubin 112 mM, and methemoglobin concentration 6.9% on an arterial blood gas. Amyl nitrite- induced hemolysis and methemoglobinemia were diagnosed. Methylene blue was not administered because of the relatively low methemo- globin concentration and the possibility of inducing further hemolysis. He was subsequently confirmed as having glucose-6-phosphate dehy- drogenase deficiency, which had originally been diagnosed in childhood. Amyl nitrite toxicity may include concurrent methemoglobinemia and hemolysis. Administration of methylene blue for clinically significant methemoglobinemia can induce further hemolysis. Copyright Ó 2013, Taiwan Society of Emergency Medicine. Published by Elsevier Taiwan LLC. All rights reserved. Keywords: Amyl nitrite; Glucose-6-phosphate dehydrogenase deficiency; Hematology; Toxicology 1. Introduction dark urine for 3 days following his return from Vanuatu 4 weeks earlier. He had drunk 100 half-coconut shells of kava Amyl nitrite is one of a number of alkyl nitrites otherwise while there. -

Approach to Anemia
APPROACH TO ANEMIA Mahsa Mohebtash, MD Medstar Union Memorial Hospital Definition of Anemia • Reduced red blood mass • RBC measurements: RBC mass, Hgb, Hct or RBC count • Hgb, Hct and RBC count typically decrease in parallel except in severe microcytosis (like thalassemia) Normal Range of Hgb/Hct • NL range: many different values: • 2 SD below mean: < Hgb13.5 or Hct 41 in men and Hgb 12 or Hct of 36 in women • WHO: Hgb: <13 in men, <12 in women • Revised WHO/NCI: Hgb <14 in men, <12 in women • Scrpps-Kaiser based on race and age: based on 5th percentiles of the population in question • African-Americans: Hgb 0.5-1 lower than Caucasians Approach to Anemia • Setting: • Acute vs chronic • Isolated vs combined with leukopenia/thrombocytopenia • Pathophysiologic approach • Morphologic approach Reticulocytes • Reticulocytes life span: 3 days in bone marrow and 1 day in peripheral blood • Mature RBC life span: 110-120 days • 1% of RBCs are removed from circulation each day • Reticulocyte production index (RPI): Reticulocytes (percent) x (HCT ÷ 45) x (1 ÷ RMT): • <2 low Pathophysiologic approach • Decreased RBC production • Reduced effective production of red cells: low retic production index • Destruction of red cell precursors in marrow (ineffective erythropoiesis) • Increased RBC destruction • Blood loss Reduced RBC precursors • Low retic production index • Lack of nutrients (B12, Fe) • Bone marrow disorder => reduced RBC precursors (aplastic anemia, pure RBC aplasia, marrow infiltration) • Bone marrow suppression (drugs, chemotherapy, radiation) -

Erythrocytes (Red Blood Cells, Rbcs)
Med Chem 535 ~ Diagnostic Medicinal Chemistry Hematology ~ Erythrocytes (Red Blood Cells, RBCs) I. Tests A. Red Blood Cell Count (RBC)* B. Hemoblobin (Hb or Hgb)* C. Hematocrit (Hct)* D. Wintrobe Indices (Indices) 1. Mean Corpuscular Volume (MCV) 2. Mean Corpuscular Hemoglobin (MCH) 3. Mean Corpuscular Hemoglobin Concentration (MCHC) E. Red Cell Distribution Width (RDW) F. Reticulocyte Count (Retics)* G. Erythrocyte Sedimentation Rate (ESR or Sed Rate) H. Serum Ferritin I. Transferrin and Serum Iron J. Haptoglobin K. Zinc Protoporphyrin Hemoglobin (ZPPH) II. RBC Disorders A. Polycythemia B. Anemias 1. Acute Blood Loss 2. Hemolytic Anemia 3. Anemia of Chronic Disease 4. Nutritional C. Hemoglobinopathies 1. Sickle Cell Anemia 2. Thalassemia 3. Methemoglobinemia/G6PD Deficiency III. Drug Induced Anemia A. Drug-Induced Oxidative Stress B. Cyanide Poisoning C. Immune Hemolytic Anemia HEMATOLOGY ~ ERYTHROCYTES HEMATOLOGY ~ the study of blood and its cellular elements: Erythrocytes (a.k.a., red blood cells), Leukocytes (a.k.a., white blood cells), and Platelets. The bone marrow typically produces ~ 2.5 x 109 RBCs, 1 x 109 granulocytes and 2.5 x 109 platelets per kg/day. CBC ~ Complete Blood Count is one of the most commonly ordered lab tests. It typically includes an erythrocyte count (RBC), leukocyte count (WBC), hemoglobin concentraton (Hgb), hematocrit (Hct), RBC indices, reticulocyte count, and platelet count. When a CBC with differential (Dif) is ordered, the WBC subtypes are quantified. Absolute Neutrophil Count (ANC) ~ neutrophil absolute number vs. relative percent Flow Cytometry Instruments can count 50,000 cells/sec When a particle passes through the detector it scatters light. Forward scattering is proportional to the size of the particle (cell): Particles between 2 fL and 20 fL are platelets; Particles > 36 fL are RBCs and WBCs; Analysis of samples with lysed RBCs affords WBCs. -

Anemia in Children JOSEPH J
Anemia in Children JOSEPH J. IRWIN, M.D., and JEFFREY T. KIRCHNER, D.O., Lancaster General Hospital, Lancaster, Pennsylvania Anemia in children is commonly encountered by the family physician. Multiple causes exist, but with a thorough history, a physical examination and limited laboratory evaluation a specific diagnosis can usually be established. The use of the mean corpuscular volume to classify the ane- mia as microcytic, normocytic or macrocytic is a standard diagnostic approach. The most common form of microcytic anemia is iron deficiency caused by reduced dietary intake. It is easily treat- able with supplemental iron and early intervention may prevent later loss of cognitive function. Less common causes of microcytosis are thalassemia and lead poisoning. Normocytic anemia has many causes, making the diagnosis more difficult. The reticulocyte count will help narrow the differential diagnosis; however, additional testing may be necessary to rule out hemolysis, hemoglobinopathies, membrane defects and enzymopathies. Macrocytic anemia may be caused by a deficiency of folic acid and/or vitamin B12, hypothyroidism and liver disease. This form of anemia is uncommon in children. (Am Fam Physician 2001;64:1379-86.) nemia is a frequent laboratory in developing humans: the embryonic, abnormality in children. As Gower-I, Gower-II, Portland, fetal hemoglo- many as 20 percent of children bin (HbF) and normal adult hemoglobin in the United States and 80 per- (HbA and HbA2). HbF is the primary hemo- cent of children in developing globin found in the fetus. It has a higher affin- Acountries will be anemic at some point by the ity for oxygen than adult hemoglobin, thus age of 18 years.1 increasing the efficiency of oxygen transfer to the fetus. -
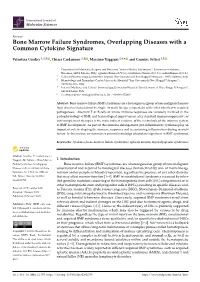
Bone Marrow Failure Syndromes, Overlapping Diseases with a Common Cytokine Signature
International Journal of Molecular Sciences Review Bone Marrow Failure Syndromes, Overlapping Diseases with a Common Cytokine Signature Valentina Giudice 1,2,3 , Chiara Cardamone 1,4 , Massimo Triggiani 1,4,* and Carmine Selleri 1,3 1 Department of Medicine, Surgery and Dentistry “Scuola Medica Salernitana”, University of Salerno, Baronissi, 84081 Salerno, Italy; [email protected] (V.G.); [email protected] (C.C.); [email protected] (C.S.) 2 Clinical Pharmacology, University Hospital “San Giovanni di Dio e Ruggi D’Aragona”, 84131 Salerno, Italy 3 Hematology and Transplant Center, University Hospital “San Giovanni di Dio e Ruggi D’Aragona”, 84131 Salerno, Italy 4 Internal Medicine and Clinical Immunology, University Hospital “San Giovanni di Dio e Ruggi D’Aragona”, 84131 Salerno, Italy * Correspondence: [email protected]; Tel.: +39-089-672810 Abstract: Bone marrow failure (BMF) syndromes are a heterogenous group of non-malignant hemato- logic diseases characterized by single- or multi-lineage cytopenia(s) with either inherited or acquired pathogenesis. Aberrant T or B cells or innate immune responses are variously involved in the pathophysiology of BMF, and hematological improvement after standard immunosuppressive or anti-complement therapies is the main indirect evidence of the central role of the immune system in BMF development. As part of this immune derangement, pro-inflammatory cytokines play an important role in shaping the immune responses and in sustaining inflammation during marrow failure. In this review, we summarize current knowledge of cytokine signatures in BMF syndromes. Keywords: cytokines; bone marrow failure syndromes; aplastic anemia; myelodysplastic syndromes Citation: Giudice, V.; Cardamone, C.; Triggiani, M.; Selleri, C. Bone Marrow 1. -
Anemia in the Insurance Applicant … What Do the Numbers Mean?
Anemia In the Insurance Applicant … What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation . Develop a consistent way to analyze Complete Blood Count (CBC) in an APS • How to use RBC (red blood cell) indices to determine type of anemia o Iron deficiency anemia o Anemia of chronic disease o Macrocytic anemia o Hemolytic anemia . Determine how the anemia is related to the entire medical history • Use the anemia rating table or go to another impairment where anemia may be a sign of disease severity 2 Blood Basics Whole blood is a mixture of plasma ~ 55% and blood cells ~ 45% 3 Blood Basics . Blood is a specialized body fluid – largest organ in the body! . Components of blood • Plasma is the unformed element of the blood – proteins circulate here • Red blood cells (erythrocytes) • White blood cells (leukocytes) • Platelets (thrombocytes) . Functions of the blood • Transport oxygen and nutrients to organs • Formation of blood clots to prevent blood loss • Carry cells and antibodies to areas of infection • Transport waste products from the liver and kidneys American Society of Hematology. Blood Basics/Homepage Accessed 5/18/16 4 Basic Hematology Components of the complete blood count (CBC) . WBC = White blood cells/infection-fighting cells . RBCs • Hemoglobin – major oxygen carrying molecule of the blood • Hematocrit – intact RBCs in volume of plasma o Expressed as a percentage of volume of blood . Platelets = involved with hemostasis (clotting) 5 Underwriting Anemia Building Blocks . Anemia is a pathologic state – it is never normal • Menstrual related blood loss exception . -

Difficult Cases of Paroxysmal Nocturnal Hemoglobinuria
Journal of Clinical Medicine Review Difficult Cases of Paroxysmal Nocturnal Hemoglobinuria: Diagnosis and Therapeutic Novelties Bruno Fattizzo 1,2,* , Fabio Serpenti 1, Juri Alessandro Giannotta 1 and Wilma Barcellini 1 1 Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, University of Milan, 20122 Milan, Italy; [email protected] (F.S.); [email protected] (J.A.G.); [email protected] (W.B.) 2 Department of Oncology and Oncohematology, University of Milan, 20122 Milan, Italy * Correspondence: [email protected]; Tel.: +39-025-5033-345 Abstract: Paroxysmal nocturnal hemoglobinuria (PNH) is an intriguing disease that can pose many difficulties to physicians, as well as to hematologists, who are unfamiliar with it. Research regarding its pathophysiologic, diagnostic, and therapeutic aspects is still ongoing. In the last ten years, new flow cytometry techniques with high sensitivity enabled us to detect PNH clones as small as <1% of a patient’s hematopoiesis, resulting in increasing incidence but more difficult data interpretation. Particularly, the clinical significance of small PNH clones in patients with bone marrow failures, including aplastic anemia and myelodysplastic syndromes, as well as in uncommon associations, such as myeloproliferative disorders, is still largely unknown. Besides current treatment with the anti-C5 eculizumab, which reduced PNH-related morbidity and mortality, new complement inhibitors will likely fulfill unmet clinical needs in terms of patients’ quality of life and better response rates (i.e., responses in subjects with C5 polymorphisms; reduction of extravascular hemolysis and breakthrough hemolysis episodes). Still, unanswered questions remain for these agents regarding their use in mono- or combination therapy, when to treat, and which drug is the best for which Citation: Fattizzo, B.; Serpenti, F.; patient. -

Hematology Ii
U.S. ARMY MEDICAL DEPARTMENT CENTER AND SCHOOL FORT SAM HOUSTON, TEXAS 78234-6100 HEMATOLOGY II SUBCOURSE MD0857 EDITION 200 DEVELOPMENT This subcourse is approved for resident and correspondence course instruction. It reflects the current thought of the Academy of Health Sciences and conforms to printed Department of the Army doctrine as closely as currently possible. Development and progress render such doctrine continuously subject to change. ADMINISTRATION For comments or questions regarding enrollment, student records, or shipments, contact the Nonresident Instruction Section at DSN 471-5877, commercial (210) 221- 5877, toll-free 1-800-344-2380; fax: 210-221-4012 or DSN 471-4012, e-mail [email protected], or write to: COMMANDER AMEDDC&S ATTN MCCS HSN 2105 11TH STREET SUITE 4192 FORT SAM HOUSTON TX 78234-5064 Approved students whose enrollments remain in good standing may apply to the Nonresident Instruction Section for subsequent courses by telephone, letter, or e-mail. Be sure your social security number is on all correspondence sent to the Academy of Health Sciences. CLARIFICATION OF TRAINING LITERATURE TERMINOLOGY When used in this publication, words such as "he," "him," "his," and "men" are intended to include both the masculine and feminine genders, unless specifically stated otherwise or when obvious in context. USE OF PROPRIETARY NAMES The initial letters of the names of some products are capitalized in this subcourse. Such names are proprietary names, that is, brand names or trademarks. Proprietary names have been used in this subcourse only to make it a more effective learning aid. The use of any name, proprietary or otherwise, should not be interpreted as an endorsement, deprecation, or criticism of a product; nor should such use be considered to interpret the validity of proprietary rights in a name, whether it is registered or not. -

The Chemistry of Hematology
The Chemistry of Hematology Gary L. Horowitz, MD Beth Israel Deaconess Medical Center Boston, MA Objectives • Explain how methylmalonic acid and homocysteine are related to B12 and folate deficiencies • List the common laboratory findings in iron deficiency anemia • Describe the chemical and molecular approaches to screening for Hereditary Hemochromatosis Topics to be Covered • Oxygen Concentration – Hemoglobin Species • D-Dimer – Separate talk later in course • Anemia – Hemolysis – Macrocytic Anemia – Microcytic Anemia Analytes • Hemoglobins • Vitamin B12 (cobalamin) – Oxyhemoglobin • Folic Acid – Reduced (Deoxy) • Homocysteine Hemoglobin • Methylmalonic Acid – Methemoglobin – Carboxyhemoglobin • D-Dimer • Iron • Transferrin/TIBC • LD (LD isoenzymes) • Ferritin • Haptoglobin Topics to be Covered • Oxygen Concentration – Hemoglobin Species • D-Dimer – Separate talk later in course • Anemia – Hemolysis – Macrocytic Anemia – Microcytic Anemia O2 Concentration in Blood • not simply PaO2 • not simply Hct (or, more precisely, Hgb) • not simply O2 saturation • rather, a combination of all 3, “O2 content” mm Hg g/dL = 0.003 * PO2 + 1.4 * [Hgb] * [%O2sat] = 0.0225 * PO2 + 1.4 * [Hgb] * [%O2sat] kPa g/dL Different Scenarios Illustrating Oxygen Content Concepts Hgb- Dissolved O2 comments PaO2 %O2Sat Hgb Hct Bound Oxygen Content O2 Normal 100 100 14 42 0.3 19.6 19.9 Low Hct 100 100 7 21 0.3 9.8 10.1 Low PaO2 25 50 14 42 0.1 9.8 9.9 (lung disease) 50% 100 50 14 42 0.3 9.8 10.1 Methemoglobin Very Low Hct 100 100 2 6 0.3 2.8 3.1 No Transfusion Hyperbaric -

Cdc 12413 DS1.Pdf
CHAPTER 1 PRINCIPLES OF DIAGNOSIS INTRODUCTION Anemia exists when a person’s level of circulating hemoglobin is lower than that in healthy persons of the same sex and age group in the same environment (Table 1). The most common kinds of anemia are due to nutritional deficiencies of iron, folic acid, and, less commonly, vitamin B12 and protein. Other common causes of anemia are congenital defects of hemoglobin production, namely, sickle cell anemia and other hemoglobinopathies, including thalassemia. Protozoal infections and infes tations, particularly malaria and hookworm, are also important direct causes of anemia, and bacterial infections may aggravate an existing anemia and prevent optimal response to hematinics. Because anemia has multiple etiologies, it presents two problems to laboratory personnel: 1. Ascertaining the presence of anemia. 2. Defining the underlying cause of the anemia. The laboratory tests that have been developed for the specialized investi gation of anemia during the past two decades can identify many types of Table 1 - Normal lower limits for hemoglobin and PCV* level Hemoglobin (g/L) PCV Infants (full term) 136 .44 Children, 3 months 95 .32 Children, 1 year 110 .36 Children, 10-12 years 120 .38 Women, nonpregnant 120 .38 Women, pregnant 130 .40 Men 130 .40 * Packed Cell Volume These are values at sea level. The hemoglobin (Hb) of most persons increases with altitude; for example, levels for men increase by about 10 g/1 at 2000 m (6500 ft) and by about 20 g/1 at 3000 m (10,000 ft). 2 Anemia anemia; however, most of these types do not represent major public health problems in developing countries, and the extensive laboratory facilities needed to identify them are often not available even in central laboratories in many developing countries. -

What Is Sickle Cell Disease?
Blood • Blood has red cells(erythrocyctes) Anemia 101 • White cells (leukocytes) • Platelets (thrombocytes) Allan Platt PA-C, MMSc Emory University PA Program Atlanta GA [email protected] www.EmoryPA.org Blood Components White Blood Cells • Fight infections • Are increased in infections Plasma 54% • Move inside and outside of blood vessels • Are made in the bone marrow White cells and platelets 1% Red Cells 45% White Blood Cells Platelets WBC - White Blood Cells 4.5 - 11.0 K/uL Low = Leukopenia High = Leukocytosis • Plug holes in the body to stop bleeding WBC Differential • Can help cause blood to clot • Neutrophils - Segs 54 -62% Made in the bone marrow Neutrophils - Bands 3 -5 % Lymphocytes - Lymphs 25 - 33% Monocytes - Monos 3 - 7% Eosinophils - Eos 1 - 3% Fibrin Basophils - Basos 0 - 0.75% Atypical Lymphs 0 1 Red Blood Cells Red Blood Cells • Carry oxygen from the lungs • Carry carbon dioxide back to the lungs • Also carry CO and NO • Normally live 120 days • Contains the protein hemoglobin • Made from iron, folic acid, vitamin B12 • Made in the bone marrow Microscope View Red Blood Cells - Shape Red cells travel through very narrow blood vessels Incidence of Sickle Cell Disease and Thalassemia World wide http://www.who.int/genomics/public/geneticdiseases/en/index2.html#SCA Red Blood Cells • Red Cell Flow Blood Vessel 2 Red Blood Cells - Hemoglobin Globin Synthesis in utero Oxygen Normal Hemoglobin A has 2 alpha and 2 beta globin chains with 4 iron binding sites Hemoglobin FA – Biochemistry – Normal Newborn Hemoglobin A – Biochemistry