National and Subnational Experience with Estimating the Extent and Trend in Completeness of Registration of Deaths in Brazil1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gawc Link Classification FINAL.Xlsx
High Barcelona Beijing Sufficiency Abu Dhabi Singapore sufficiency Boston Sao Paulo Barcelona Moscow Istanbul Toronto Barcelona Tokyo Kuala Lumpur Los Angeles Beijing Taiyuan Lisbon Madrid Buenos Aires Taipei Melbourne Sao Paulo Cairo Paris Moscow San Francisco Calgary Hong Kong Nairobi New York Doha Sydney Santiago Tokyo Dublin Zurich Tokyo Vienna Frankfurt Lisbon Amsterdam Jakarta Guangzhou Milan Dallas Los Angeles Hanoi Singapore Denver New York Houston Moscow Dubai Prague Manila Moscow Hong Kong Vancouver Manila Mumbai Lisbon Milan Bangalore Tokyo Manila Tokyo Bangkok Istanbul Melbourne Mexico City Barcelona Buenos Aires Delhi Toronto Boston Mexico City Riyadh Tokyo Boston Munich Stockholm Tokyo Buenos Aires Lisbon Beijing Nanjing Frankfurt Guangzhou Beijing Santiago Kuala Lumpur Vienna Buenos Aires Toronto Lisbon Warsaw Dubai Houston London Port Louis Dubai Lisbon Madrid Prague Hong Kong Perth Manila Toronto Madrid Taipei Montreal Sao Paulo Montreal Tokyo Montreal Zurich Moscow Delhi New York Tunis Bangkok Frankfurt Rome Sao Paulo Bangkok Mumbai Santiago Zurich Barcelona Dubai Bangkok Delhi Beijing Qingdao Bangkok Warsaw Brussels Washington (DC) Cairo Sydney Dubai Guangzhou Chicago Prague Dubai Hamburg Dallas Dubai Dubai Montreal Frankfurt Rome Dublin Milan Istanbul Melbourne Johannesburg Mexico City Kuala Lumpur San Francisco Johannesburg Sao Paulo Luxembourg Madrid Karachi New York Mexico City Prague Kuwait City London Bangkok Guangzhou London Seattle Beijing Lima Luxembourg Shanghai Beijing Vancouver Madrid Melbourne Buenos Aires -
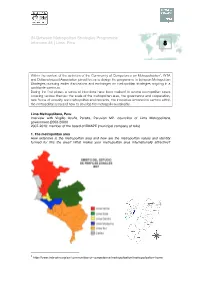
IN-Between Metropolitan Strategies Programme Interview #8 | Lima, Peru 8
IN-Between Metropolitan Strategies Programme Interview #8 | Lima, Peru 8 Within the context of the activities of the Community of Competence on Metropolisation1, INTA and Deltametropool Association joined forces to design the programme In-between Metropolitan Strategies pursuing earlier discussions and exchanges on metropolitan strategies ongoing in a worldwide spectrum. During the first phase, a series of interviews have been realised to several metropolitan cases covering various themes: the scale of the metropolitan area, the governance and cooperation, new forms of urbanity and metropolitan environments, the innovative economical sectors within the metropolitan area and how to develop the metropolis sustainably. Lima Metropolitana, Peru Interview with Virgilio Acuña Peralta, Peruvian MP, councillor of Lima Metropolitana government (2003-2006) 2007-2010: member of the board of EMAPE (municipal company of tolls) 1.! The metropolitan area How extensive is the metropolitan area and how are the metropolitan values and identity formed for this the area? What makes your metropolitan area internationally attractive? 1 http://www.inta-aivn.org/en/communities-of-competence/metropolisation/metropolisation-home In Between Metropolitan Strategies Programme – Interview 7 Lima Metropolitana counts 9 millions inhabitants (including the Province of Callao) and 42 districts. The administrative region of Lima Metropolitana (excluding Callao) has a total surface of 2800 km2. The metropolitan area has an extension of 150km North-South and 60Km on the West (sea coast) - East (toward the Andes) direction. The development of the city with urban sprawl goes south, towards the seaside resorts, outside of the administrative limits of Lima Metropolitana (Province of Cañete, City of Ica) and to the Northern beach areas. -

Spanish Impact on Peru (1520 - 1824)
Spanish Impact on Peru (1520 - 1824) San Francisco Cathedral (Lima) Michelle Selvans Setting the stage in Peru • Vast Incan empire • 1520 - 30: epidemics halved population (reduced population by 80% in 1500s) • Incan emperor and heir died of measles • 5-year civil war Setting the stage in Spain • Iberian peninsula recently united after 700 years of fighting • Moors and Jews expelled • Religious zeal a driving social force • Highly developed military infrastructure 1532 - 1548, Spanish takeover of Incan empire • Lima established • Civil war between ruling Spaniards • 500 positions of governance given to Spaniards, as encomiendas 1532 - 1548, Spanish takeover of Incan empire • Silver mining began, with forced labor • Taki Onqoy resistance (‘dancing sickness’) • Spaniards pushed linguistic unification (Quechua) 1550 - 1650, shift to extraction of mineral wealth • Silver and mercury mines • Reducciones used to force conversion to Christianity, control labor • Monetary economy, requiring labor from ‘free wage’ workers 1550 - 1650, shift to extraction of mineral wealth • Haciendas more common: Spanish and Creole owned land, worked by Andean people • Remnants of subsistence-based indigenous communities • Corregidores and curacas as go- betweens Patron saints established • Arequipa, 1600: Ubinas volcano erupted, therefor St. Gerano • Arequipa, 1687: earthquake, so St. Martha • Cusco, 1650: earthquake, crucifix survived, so El Senor de los Temblores • Lima, 1651: earthquake, crucifixion scene survived, so El Senor de los Milagros By 1700s, shift -

FGV Direito Rio in Rio De Janeiro, Brazil
FGV Direito Rio in Rio de Janeiro, Brazil FGV Direito Rio is one of the most well respected education institutions in one of the most exciting international cities in the world. There are more than 3,000 undergraduate students and almost 2,000 graduate and master’s students enrolled. During the 2019-20 academic year, no U of M Law students participated in the semester exchange. Summary of Course Offerings http://direitorio.fgv.br/graduacao/gradecurricular Semester Dates Fall semester: August through December 2020 Spring semester: February to July 2021 Language of instruction Portuguese; four to six courses are offered in English each semester Courses/Credits/Grades Up to 15 credits may be transferred per semester abroad Each class period is 100 minutes; each course has either 30 or 60 “course hours” Grading is from 0 (minimum) to 10 (maximum) with a passing grade being 7 2 ECTS Credits = 1 Minnesota Credit Registration Registration is done by the International Office prior to the student’s arrival. Participate in our Law School’s lottery for the term you will be away. Register for 12-15 credits. Before leaving for your semester abroad, contact the Law School registrar at [email protected] to convert your credits to Off-campus Legal Studies. Housing FGV Direito Rio does not have on-campus housing for international students. They will provide assistance once students arrive in locating and obtaining off-campus accommodations. Financial Aid and Tuition Payment Financial aid will remain in effect for the semester you are abroad. Please make arrangements to have the balance (after tuition is deducted) sent to you if disbursement occurs after you have departed the U.S. -

Buenos Aires to Lima By
FH {SR--27 The Bolivar Hotel Lima, Peru August 31, 1942 Dear hr. <oer s It is surprising how simple and relatively unexciting it seems to fly. Saturday, August 22, I climbed aboard a seven-ton, two-motored anagra plane and took off for the first time in my.life on the first lap of a 6,000 mile air journey--Buenos Aires to iiami. We were off and away without a bump. In a few minutes we were roaring high above the pampa. There is no reason to get poetic about a bird's eye view of the rGentine plains. For two and a half hours, at seven thousand feet, we moved over the flat gra. in belt. I amused myself by looking at the edge of the ing and watching one field after another come into view. That way one 5or the feeling of mo- tion.. any of the fields, I knew, were as large as five hundred or a thousand acres. One could count the chacras below. Every primitive bin or two meant a chacra. One could look right down upon th yel'low ,aize in thcorntrojes, uncovered and unpro- tected from the elements. Estancias were umistakable too, for stately groves of trees numbered them. Trees stood out best of all. In two hours flyin time the .green of the green fields bec-ame lighter, ore delicate, and I kno: that C6rdoba could not be very far away. Surely enoush, 6rdoba came into view, restin in a natural de- pression at the foot of the sierras and at the edge of the pampa. -

El Ermitaño and Pampa De Cueva As Case Studies for a Regional Urbanization Strategy
Article Place-Making through the Creation of Common Spaces in Lima’s Self-Built Settlements: El Ermitaño and Pampa de Cueva as Case Studies for a Regional Urbanization Strategy Samar Almaaroufi 1, Kathrin Golda-Pongratz 1,2,* , Franco Jauregui-Fung 1 , Sara Pereira 1, Natalia Pulido-Castro 1 and Jeffrey Kenworthy 1,3,* 1 Department of Architecture, Civil Engineering and Geomatics, Frankfurt University of Applied Sciences, 60318 Frankfurt, Germany; samarmaaroufi@gmail.com (S.A.); [email protected] (F.J.-F.); [email protected] (S.P.); [email protected] (N.P.-C.) 2 UIC School of Architecture, Universitat Internacional de Catalunya, 08017 Barcelona, Spain 3 Curtin University Sustainability Policy Institute, Curtin University, Bentley 6102, Australia * Correspondence: [email protected] (K.G.-P.); jeff[email protected] (J.K.) Received: 30 October 2019; Accepted: 2 December 2019; Published: 10 December 2019 Abstract: Lima has become the first Peruvian megacity with more than 10 million people, resulting from the migration waves from the countryside throughout the 20th century, which have also contributed to the diverse ethnic background of today’s city. The paper analyzes two neighborhoods located in the inter-district area of Northern Lima: Pampa de Cueva and El Ermitaño as paradigmatic cases of the city’s expansion through non-formal settlements during the 1960s. They represent a relevant case study because of their complex urbanization process, the presence of pre-Hispanic heritage, their location in vulnerable hillside areas in the fringe with a protected natural landscape, and their potential for sustainable local economic development. The article traces back the consolidation process of these self-built neighborhoods or barriadas within the context of Northern Lima as a new centrality for the metropolitan area. -

December 2017
Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Abidjan CR1 5 Abidjan DV1 9 Abidjan DV2 3 Abidjan DV3 2 Abidjan F11 1 Abidjan F12 1 Abidjan F21 1 Abidjan F22 2 Abidjan F23 1 Abidjan F41 1 Abidjan F42 1 Abidjan F43 2 Abidjan FX1 3 Abidjan FX2 1 Abidjan IR2 6 Abidjan IR5 5 Abu Dhabi CR1 6 Abu Dhabi CR2 3 Abu Dhabi DV1 12 Abu Dhabi DV2 4 Abu Dhabi DV3 5 Abu Dhabi E11 1 Abu Dhabi E14 1 Abu Dhabi E15 1 Abu Dhabi E21 3 Abu Dhabi E31 10 Abu Dhabi E34 7 Abu Dhabi E35 7 Abu Dhabi F11 1 Abu Dhabi F21 2 Abu Dhabi F24 1 Abu Dhabi F33 5 Abu Dhabi F41 6 Abu Dhabi F42 4 Abu Dhabi F43 5 Abu Dhabi FX1 3 Abu Dhabi I51 15 Abu Dhabi I52 13 Abu Dhabi I53 23 Abu Dhabi IR1 4 Abu Dhabi IR2 4 Abu Dhabi IR5 7 Page 1 of 57 Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Accra CR1 45 Accra CR2 1 Accra DV1 24 Accra DV2 9 Accra DV3 14 Accra E31 1 Accra E34 1 Accra F11 19 Accra F12 9 Accra F21 22 Accra F22 20 Accra F23 3 Accra F24 2 Accra F31 6 Accra F32 6 Accra F33 10 Accra F41 11 Accra F42 7 Accra F43 7 Accra FX1 10 Accra FX2 15 Accra FX3 9 Accra IB3 1 Accra IR1 76 Accra IR2 101 Accra IR3 4 Accra IR5 79 Addis Ababa CR1 52 Addis Ababa DV1 109 Addis Ababa DV2 23 Addis Ababa DV3 24 Addis Ababa E11 2 Addis Ababa E14 2 Addis Ababa E15 4 Addis Ababa F11 10 Addis Ababa F12 1 Addis Ababa F21 27 Addis Ababa F22 25 Addis Ababa F24 10 Addis Ababa F25 1 Addis Ababa F41 3 Addis Ababa F42 2 Page 2 of 57 Immigrant Visa Issuances By Post December 2017 (FY 2018) Post Visa Class Issuances Addis Ababa F43 5 Addis -

Global Rescue Will Evacuate You to Your Home Hospital of Choice
Mumbai. Qogir. Shanghai. Karachi. Istanbul. Delhi. São Paulo. Moscow. Medical Evacuation. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Ja- karta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Security Evacuation. Lima. Bogotá. Hong Kong. Bangkok . Makalu. Cairo. Dhaka. Ho Chi Minh City. Annapurna. Rio de Janeiro. Tianjin. Chongqing. Baghdad. Lhotse. Bangalore.Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou. Nanga Parbat. Saint Petersburg. Wuhan. Chennai. Medical Evacuation. Riyadh. Alexandria. Surat. Hyderabad. Shenyang. Ahmedabad. Ankara. Field Rescue. Cho Oyu. Johannesburg. Los Angeles. Kangchenjunga. Abidjan. Yokohama. Busan. Cape Town. Durban. Berlin. Pune. Pyongyang. Madrid. Kanpur. Jaipur. Field Rescue. Buenos Aires. Dhaulagiri. Nairobi. Jeddah. Mumbai. Qogir. Shanghai. Security Evacuation. Karachi. Istanbul. Delhi. São Paulo. Moscow. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Jakarta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Lima. Bogotá. Hong Kong. Bangkok Makalu. Cairo. Dhaka. Ho Chi Minh City. Annapurna. Rio de Janeiro. Tianjin. Chongqing. Baghdad. Lhotse. Bangalore. Field Rescue. Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou. Nanga Parbat. Security Evacuation. Saint Petersburg. Wuhan. Medical Evacuation. Chennai. Riyadh. Alexandria. Surat. Hyderabad. Shenyang. Ahmedabad. Ankara. Cho Oyu. Johannesburg. Los Angeles. Kangchenjunga. Abidjan. Yokohama. Busan. Cape Town. Durban. Berlin. Pune. Pyongyang. Madrid. Kanpur. Jaipur. Buenos Aires. Dhaulagiri. Nairobi.Global Jeddah. Mumbai. Qogir. Shanghai. Rescue Karachi. Istanbul. Delhi. São Paulo. Moscow. Medical Evacuation. Seoul. Beijing. Mount Everest. Mexico City. Tokyo. Jakarta. New York City. Lagos. Kinshasa. Nepal. Tehran. London. Manaslu. Security Evacuation. Lima. Bogotá. Hong CriticalKong. Bangkok . ServicesMakalu. Cairo. Dhaka.Provided Ho Chi Minh to City. Stratfor Annapurna. Rio deEnterprises, Janeiro. Tianjin. Chongqing. LLC Baghdad. Lhotse. Bangalore.Kolkata. Yangon. Santiago. Pakistan. Singapore. Guangzhou. -

The Lima-‐Paris Ac on Agenda (LPAA)
The Lima-Paris Acon Agenda (LPAA) Octubre 2015 LPAA – Background • UN Secretary-General’s Climate Summit (New York, September 2014) • Decision 1/CP.20 ‘Lima Call for Climate Acon’: “The Conference of Pares […] encourages the Execuve Secretary and the President of the Conference of the Pares to convene an annual high level event on enhancing implementaon of climate acon”. • Workstream 2 discussions and TEM’s process. LPAA – Raonale • Multude of actors are already engaged in climate acon, in different contexts and at different scales. • They need support for recognion, scaling up and to assess their acRon and related impacts. Ø Lima-Paris Acon Agenda (LPAA) LPAA – Objecves • Constute a broad plaZorm of selected mul sectoral cooperave iniaves, with the view to: - Showcasing progress made under the most promising iniaves and supporng their extension and replicaon - Encouraging new substanal commitments from new iniaves and actors, in all sectors - Promong cross-sectoral mul-stakeholder collaboraon - Highlighng linkages with SDGs - Building polical momentum ad bringing ‘the real world’ in climate negoaons (CoP21 decision?) - Ensuring the connuity and strenghtening of the Acon Agenda beyond Paris (SDGs implementaon etc.) Criteria for inclusion in the LPAA (1/2) • Ambious: short and long term quanfiable targets – transformave acons guided by a 2°C goal pathway. • Science based: Address a concrete impact of climate change. Transformave acons should apply new technologies, knowledge, communicaon strategy and/ or financial schemes that move a large group, industry, city or country towards a low carbon and more resilient future. • For cooperave internaonal iniaves: Mul-stakeholder approach – Inclusiveness – Balance regional representaon. Criteria for inclusion in the LPAA (2/2) • Capacity to deliver. -

International Civil Aviation Organization SAM/IG/23-IP/14
International Civil Aviation Organization SAM/IG/23-IP/14 South American Regional Office – Regional Project RLA/03/901 12/05/2019 Twenty Third Workshop/Meeting of the SAM Implementation Group (SAM/IG/23) – Regional Project RLA/06/901 (Lima, Peru, 20 to 24 May 2019) Agenda Item 5: Operational implementation of new ATM automated systems and integration of the existing systems a) Follow-up to AIDC performance and operation in the SAM Region STATUS OF AIDC IN COLOMBIA (Presented by Colombia) SUMMARY This information paper presents an operational concept to report on the status of implementation of AIDC in Colombia References: PANS/ATM (Doc 4444) Manual on AIDC implementation ASIA/PAC ICD 1. Background 1.1 In 1971, in order to decongest coordination speech channels, the NAT Region created what at that time was called OLDI (On Line Data Interchange), a concept still used by several ICAO Regions. 1.2 In 1994, the ASIA/PAC Regions saw the need to make OLDI more versatile and thus promoted the creation of another means of coordination, which they called AIDC. 1.3 The GREPECAS 15 meeting held in Brazil in 2008 formulated conclusion GREPECAS15/36: MEASURES TO REDUCE OPERATIONAL ERRORS IN THE ATC COORDINATION LOOP BETWEEN ADJACENT ACCs The DECLARATION OF BOGOTA, signed in December 2013, DECLARES its commitment to attain the following regional goals by 2016: 14. Interconnection of automated systems (ATS interfacility data communication - AIDC)) 100% of automated system interconnections. 2. Background 2.1 The SAM/IG14 meeting reviewed a plan of activities for the implementation of the AIDC interconnection in the SAM Region, starting with some of the States along the Pacific coast (Chile, Colombia, Ecuador and Peru), and considered that it should be submitted to the approval of the Eighth coordination meeting of Project RLA/06/901 (RCC/8). -

Lima Financial Services Cluster
MICROECONOMICS OF COMPETITIVENESS FINANCIAL SERVICES CLUSTER IN LIMA FINAL REPORT Mauricio Concha Zegarra Thomas Leonard Renato Sabato Felipe Santos Jade Smith Professor: Laura Alfaro Friday, May 6th, 2016 Harvard Business School 1 Note: Our team includes a Peruvian national who was helpful in accessing information and members who have some prior exposure to the microfinance sector through class or work. Thus, some of our information is not directly cited as it comes from previous and common knowledge, not a direct source. Country Analysis Since gaining independence from the Spanish Empire in 1824, Peru has had a long history of dictatorships and military coups. Only in the 1980s did the country achieve a peacefully elected democracy. Since that time, in spite of pressure from fringe, armed political groups like the “Shining Path”, the country has managed thirty-six years (and counting) of stable democracy. The country today exists as a constitutional republic with a unicameral legislature, and there are roughly eight active political parties at the national stage1 (parties coalesce and diverge as coalitions form and break apart from vote to vote).2 Like many South American countries, Peru’s population is predominantly of native or mestizo heritage (at 45% and 37% of the population, respectively), but the remaining 18% is Caucasian (15%), African, or East Asian (3%). In the last ten years, the country has seen net emigration of about two million people, mostly to the US, Spain, and Argentina.3 Peru’s population diversity and connections to other continents complement the country’s geographic strengths. Situated on the Pacific coast of South America, centered on the north-south axis of the continent, Peru offers over 1,900 miles of ocean coastline and acts as a central hub for air travel to, from, and around the continent. -

Public Health in Lima, Peru, 1535
THE NATURE OF COLONIAL BODIES: PUBLIC HEALTH IN LIMA, PERU, 1535- 1635 A Dissertation Submitted to the Graduate School of the University of Notre Dame in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy by Kathleen M. Kole de Peralta Karen Graubart, Director Graduate Program in History Notre Dame, Indiana July 2015 © Copyright 2015 Kathleen M. Kole de Peralta THE NATURE OF COLONIAL BODIES: PUBLIC HEALTH IN LIMA, PERU, 1535- 1640 Abstract by Kathleen M. Kole de Peralta In 1535, Francisco Pizarro founded Lima, Peru in the middle of a coastal dessert. Its residents transformed the landscape to build a colonial capital and in the process, the landscape shaped local understandings of race, gender, social status and power. Lima’s urban environment created a public health discourse that focused on the relationship between the natural world and human welfare. These discussions emerged in response to the rapid rate of Lima’s growth and the challenges it faced, including deforestation, food supply challenges, and the concentration of waste, disease, and illness. I argue that Lima’s cabildo [municipal government], comprised of just a fraction of the population, seized on these adversities to empower themselves over the majority of the population, promote their interests, and negotiate interactions between humans and their environs. Using the discourse of colonial bodies, health, and the natural world, town councilmen endeavored to control a racially and socially diverse population that surpassed 25,000 people by 1614. For my family ii CONTENTS Figures……………………………………………………………………... iv Tables………………………………………………………………………. v Acknowledgments………………………………………………………….. vii Chapter 1: What Nature Does to the Body………………………………… 1 1.1.