Minutes Board of Health HL29.1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Summary by Quartile.Xlsx
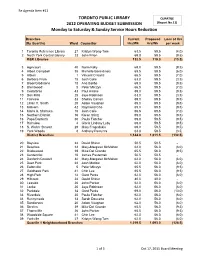
Re Agenda Item #11 TORONTO PUBLIC LIBRARY QUARTILE 2012 OPERATING BUDGET SUBMISSION (Report No.11) Monday to Saturday & Sunday Service Hours Reduction Branches Current Proposed Loss of Hrs (By Quartile) Ward Councillor Hrs/Wk Hrs/Wk per week 1 Toronto Reference Library 27 Kristyn Wong-Tam 63.5 59.5 (4.0) 2 North York Central Library 23 John Filion 69.0 59.5 (9.5) R&R Libraries 132.5 119.0 (13.5) 3 Agincourt 40 Norm Kelly 69.0 59.5 (9.5) 4 Albert Campbell 35 Michelle Berardinetti 65.5 59.5 (6.0) 5 Albion 1 Vincent Crisanti 66.5 59.5 (7.0) 6 Barbara Frum 15 Josh Colle 63.0 59.5 (3.5) 7 Bloor/Gladstone 18 Ana Bailão 69.0 59.5 (9.5) 8 Brentwood 5 Peter Milczyn 66.5 59.5 (7.0) 9 Cedarbrae 43 Paul Ainslie 69.0 59.5 (9.5) 10 Don Mills 25 Jaye Robinson 63.0 59.5 (3.5) 11 Fairview 33 Shelley Carroll 69.0 59.5 (9.5) 12 Lillian H. Smith 20 Adam Vaughan 69.0 59.5 (9.5) 13 Malvern 42 Raymond Cho 69.0 59.5 (9.5) 14 Maria A. Shchuka 15 Josh Colle 66.5 59.5 (7.0) 15 Northern District 16 Karen Stintz 69.0 59.5 (9.5) 16 Pape/Danforth 30 Paula Fletcher 69.0 59.5 (9.5) 17 Richview 4 Gloria Lindsay Luby 69.0 59.5 (9.5) 18 S. Walter Stewart 29 Mary Fragedakis 69.0 59.5 (9.5) 19 York Woods 8 AAnthonynthony Perruzza 63.0 59.5 ((3.5)3.5) District Branches 1,144.0 1,011.5 (132.5) 20 Bayview 24 David Shiner 50.5 50.5 - 21 Beaches 32 Mary-Margaret McMahon 62.0 56.0 (6.0) 22 Bridlewood 39 Mike Del Grande 65.5 56.0 (9.5) 23 Centennial 10 James Pasternak 50.5 50.5 - 24 Danforth/Coxwell 32 Mary-Margaret McMahon 62.0 56.0 (6.0) 25 Deer Park 22 Josh Matlow 62.0 56.0 (6.0) -
While Every Effort Is Made to Ensure the Accuracy of the Contents
While every effort is made to ensure the accuracy of the contents of this site, users should be aware that due to circumstances beyond our control, it may be necessary to change the text of documents posted here and therefore no responsibility will be accepted by the Toronto Transit Commission for discrepancies which may occur between documents contained on this site and the formal hardcopy versions presented to the Commission. If it is necessary to rely on the accuracy of Commission documents the Office of the General Secretary should be contacted at 393-3698 to obtain a certifed copy. ONLY HARDCOPY RECORDS CERTIFIED BY THE GENERAL SECRETARY WILL BE DEEMED TO BE OFFICIAL. Form Revised: February 2005 TORONTO TRANSIT COMMISSION REPORT NO. MEETING DATE: March 21, 2007 SUBJECT: Membership – TTC Committees RECOMMENDATION It is recommended that the Commission receive this report for information. DISCUSSION The attached provides a list of TTC Committees along with the membership for each Committee. - - - - - - - - - - - - March 2, 2007 1-16 Attachment TTC COMMITTEES TTC PROPERTY COMMITTEE Michael Thompson (Chair) Glenn De Baeremaeker Adam Giambrone Suzan Hall Peter Milczyn Anthony Perruzza TTC ADVERTISING REVIEW COMMITTEE Sandra Bussin Suzan Hall Anthony Perruzza Bill Saundercook (Committee Chair to be determined) TTC AUDIT COMMITTEE Bill Saundercook (Chair) Adam Giambrone Anthony Perruzza TTC BUDGET COMMITTEE Adam Giambrone Joe Mihevc Peter Milczyn Anthony Perruzza Bill Saundercook Michael Thompson (Committee Chair to be determined) TTC e-SYSTEM -

Agenda Item History - 2013.MM41.25
Agenda Item History - 2013.MM41.25 http://app.toronto.ca/tmmis/viewAgendaItemHistory.do?item=2013.MM... Item Tracking Status City Council adopted this item on November 13, 2013 with amendments. City Council consideration on November 13, 2013 MM41.25 ACTION Amended Ward:All Requesting Mayor Ford to respond to recent events - by Councillor Denzil Minnan-Wong, seconded by Councillor Peter Milczyn City Council Decision Caution: This is a preliminary decision. This decision should not be considered final until the meeting is complete and the City Clerk has confirmed the decisions for this meeting. City Council on November 13 and 14, 2013, adopted the following: 1. City Council request Mayor Rob Ford to apologize for misleading the City of Toronto as to the existence of a video in which he appears to be involved in the use of drugs. 2. City Council urge Mayor Rob Ford to co-operate fully with the Toronto Police in their investigation of these matters by meeting with them in order to respond to questions arising from their investigation. 3. City Council request Mayor Rob Ford to apologize for writing a letter of reference for Alexander "Sandro" Lisi, an alleged drug dealer, on City of Toronto Mayor letterhead. 4. City Council request Mayor Ford to answer to Members of Council on the aforementioned subjects directly and not through the media. 5. City Council urge Mayor Rob Ford to take a temporary leave of absence to address his personal issues, then return to lead the City in the capacity for which he was elected. 6. City Council request the Integrity Commissioner to report back to City Council on the concerns raised in Part 1 through 5 above in regard to the Councillors' Code of Conduct. -

Can Toronto Be Run Like a Business? Observations on the First Two Years of the Ford Mayoralty in Torontoi
Can Toronto be Run Like a Business? Observations on the First Two Years of the Ford Mayoralty in Torontoi. Richard Stren Cities Centre University of Toronto Prepared for Presentation at the CPSA Annual Conference, Edmonton, Alberta June, 2012 Draft Only. No Citations or References without Express Consent of the Author. Mayoral candidate Rob Ford’s speech at the National Ethnic Press and Media Council of Canada (August 9, 2010): I come from the private sector, where my father started a labeling company….I’m proud to say that with the help of my brothers we have expanded to three locations in New Jersey, Chicago and Rexdale, and we now employ approximately 300 people….What I have seen in the last ten years is very disturbing at City Hall. I’ve seen taxes go up and services go down… In the private sector, we deliver, it’s very simple. The first rule is, the customer is always right. The second rule is, repeat the first rule…In politics we should take the exact same attitude….The taxpayer is the boss of all the civil servants….I really take a business approach to politics…in that customer service is lacking at city hall. …Customer service is number one. Downloaded on May 10, 2012 at: http://www.youtube.com/watch?v=QOBotCHFRZE Video interview with Rob Ford on the day before the 2010 election: …[my brother and I have] run my father’s business that he started in 1962. We’ve expanded into Chicago and New Jersey. That’s the business approach I want to take to running the city. -

Blue Banner, Is Published Two Times Per Year
bbllue banner HAEL’S COLLEGE SC ST. MIC HOOL Volume 13 ~ Fall/Winter 2012 SPECIAL POLITICS ISSUE 16 Making Our Mark In Public Service 18 St. Mike’s and Party Politics 20 All Politics is Local lettersbb tol theu editore banner HAEL’S COLLEGE S ST. MIC CHOOL The St. Michael’s College School alumni magazine, Blue Banner, is published two times per year. It reflects the history, accomplishments and stories of graduates and its purpose is to promote collegiality, respect and Christian values under the direction of the Basilian Fathers. TABLE OF CONTENTS USEFUL WEBSITES PRESIDENT: Terence M. Sheridan ’89 Message from the President 4 St. Michael’s College School: www.stmichaelscollegeschool.com EDITOR: Gavin Davidson ’93 Message from the Alumni President 5 Blue Banner Online: www.mybluebanner.com CO-EDITOR: Michael De Pellegrin ’94 Letter from the Editor 6 Basilian Fathers: www.basilian.org CISAA (Varsity Athletic Schedule): www.cisaa.ca Tel: 416-653-3180 ext. 292 Fax: 416-653-8789 Letters to the Editor 7 Twitter: www.twitter.com/smcs1852 E-mail: [email protected] Alumni E-mail: [email protected] Open Letter to Alumni: Canada Publications Mail Agreement #40006997 One Mission, One Thousand Options 8 CONTACT DIRECTORY Welcoming the New Alumni Executive 9 CONTRIBUTING EDITORS Tel: 416-653-3180 ext. 292 Paul Forbes Retires After 36 Years and 29 Titles 10 Kimberley Bailey, Fr. Lawrence Hyginus ’00, Jillian Kaster, Pat Mancuso ’90, Richard McQuade, E-mail: [email protected] Rick Naranowicz ’73, Joe Younder ’56 A Major Renewal 12 Web: www.stmichaelscollegeschool.com • Admissions (ext. 195) Securing our Future by Giving Back 13 ALUMNI EXECUTIVE 2012-2015 • Advancement (ext. -

March 29, 2018 Mayor John Tory Office of the Mayor City Hall, 2Nd Floor 100 Queen St. W. Toronto, on M5H 2N2 Realizing Toronto Y
March 29, 2018 Mayor John Tory Office of the Mayor City Hall, 2nd Floor 100 Queen St. W. Toronto, ON M5H 2N2 Realizing Toronto’s Opportunity to Redevelop Downsview Your Worship, On behalf of the Ontario Society of Professional Engineers (OSPE), I am writing to request your support for the redevelopment of the Downsview lands: an incredible, multi-billion dollar opportunity for the city of Toronto to increase its supply of housing, attract investment and jobs and cement itself as a global centre for engineering innovation. As you are aware, Bombardier Aerospace announced their intention to relocate their operations at Downsview. For Toronto, this move presents a tremendous prospect for innovation and urban renewal that is unparalleled in modern history. Spanning an impressive 375-acres of prime development lands, Toronto’s opportunity at Downsview supersedes previous urban development success stories such as New York’s Hudson Yards and London’s Canary Wharf (24 and 97-acres respectively). Not only is its sheer size unprecedented—Downsview is also shovel-ready, presenting Toronto with a turn-key public project that complements existing infrastructure. Unlike most urban renewal projects around the globe, this development is able to monopolize on existing public infrastructure stock, thereby avoiding the time and resource costs typically associated with the construction of new service and transit linkages. The Downsview lands are situated at the epicentre of three world-class universities and benefits from exceptional connections to existing subway, rail, and highway transportation infrastructure. Developing Downsview can improve the flow and functionality of Toronto’s transit network. The development of the Downsview lands promises to improve ridership and the efficiency of the entire transit network by encouraging two-way passenger flows. -

Councillor Joe Mihevc Toronto City Hall St
Councillor Joe Mihevc Toronto City Hall St. Paul's West Ward 21 September 9th, 2015 Dear Colleagues, Re: Invitation to a public meeting informing Torontonians how they may assist Syrian refugees: I would like to invite you to join Councillor Joe Cressy (Ward 20, Trinity-Spadina), Debbie Douglas, Executive Director of OCASI (Ontario Council of Agencies Serving Immigrants), Ratna Omidvar, (Chair), Executive Director, Global Diversity Exchange, community agencies and me for a public meeting about the Syrian refugee crisis. The purpose of this meeting is to provide Torontonians with information and tangible action plans around how to assist people impacted by the ongoing refugee crisis. We have been hearing that, while several Canadians have already opened their homes, many more do not know how to get involved with the various initiatives currently taking place in Toronto or where to obtain the necessary information. The meeting will be held on: Date: Sunday, September 27th Time: 2:00pm – 4:00pm Venue: City Hall, Council Chambers and Members' Lounge, 100 Queen Street West We will hear from Ms. Douglas, Ms. Omidvar and yourself about how Torontonians can become more involved in supporting families and individuals through sponsorship and community support. There will also be an opportunity for your organization to have a display table along with relevant material. Kindly distribute this invitation to others who may be interested in participating as agencies or attending the meeting as potential refugee sponsors. If you would like to participate in this event or would like additional information about this meeting, please contact my office at 416.392.0208 or [email protected]. -

Item MM37.16
Agenda Item History - 2013.MM37.16 http://app.toronto.ca/tmmis/viewAgendaItemHistory.do?item=2013.MM... Item Tracking Status City Council adopted this item on July 16, 2013 without amendments. City Council consideration on July 16, 2013 MM37.16 ACTION Adopted Ward:All Protecting the Great Lakes from Invasive Species: Asian Carp - by Councillor Mike Layton, seconded by Councillor Paul Ainslie City Council Decision City Council on July 16, 17, 18 and 19, 2013, adopted the following: 1. City Council write a letter to the Federal and Provincial Ministers of the Environment strongly urging all parties to work in cooperation with the U.S. Army Corps of Engineers, to identify a preferred solution to the invasive carp issue and move forward to implement that solution with the greatest sense of urgency. Background Information (City Council) Member Motion MM37.16 (http://www.toronto.ca/legdocs/mmis/2013/mm/bgrd/backgroundfile-60220.pdf) Communications (City Council) (July 10, 2013) Letter from Dr. Terry Quinney, Provincial Manager, Fish and Wildlife Services, Ontario Federation of Anglers and Hunters (MM.Supp.MM37.16.1) (http://www.toronto.ca/legdocs/mmis/2013/mm/comm/communicationfile-39105.pdf) (July 12, 2013) Letter from Dr. Mark Gloutney, Director of Regional Operations - Eastern Region, Ducks Unlimited Canada (MM.Supp.MM37.16.2) (http://www.toronto.ca/legdocs/mmis/2013/mm/comm/communicationfile-39106.pdf) (July 12, 2013) E-mail from Terry Rees, Executive Director, Federation of Ontario Cottagers' Association (MM.Supp.MM37.16.3) (http://www.toronto.ca/legdocs/mmis/2013/mm/comm/communicationfile-39097.pdf) (July 16, 2013) Letter from Bob Kortright, Past President, Toronto Field Naturalists (MM.New.MM37.16.4) (http://www.toronto.ca/legdocs/mmis/2013/mm/comm/communicationfile-39184.pdf) Motions (City Council) Motion to Waive Referral (Carried) Speaker Nunziata advised Council that the provisions of Chapter 27, Council Procedures, require that Motion MM37.16 be referred to the Executive Committee. -

Speakers.Pdf
Presenters DAVE WALLACE [email protected] Dave Wallace became the Chief Information Officer (CIO) of the City of Toronto in May 2007. He is responsible for overseeing the City’s Information and Technology (I&T) services, working closely with the City’s divisions in support of their services to the public. He is also focusing on establishing a new organizational structure with an emphasis on strategies and business services functional responsibility. The result will be a new level of I&T services in the City that will transform the way I&T is delivered to meet both the City strategic and program specific needs now and into the future. Prior to joining the City, Dave was Vice-President of the National Public Sector Program at Chartwell Inc., where he provided advisory services, leadership and support to all three levels of government. He has completed many successful projects across the country in the areas of enterprise architecture, project portfolio management, applications development life cycle, IT service catalogue and business architecture. Dave has held many key roles in more than 20 years of service with the Ontario Government. He served for three years as the first Corporate Chief Technology Officer (CTO) within the OPS, reporting to the Office of the Corporate Chief Information Officer. In establishing the CTO’s Office, Dave created a flexible, agile team that provided strategic guidance to business areas on technology and information management trends, architecture methods, and standards. Dave was also Head Architect in the Office of the Corporate Chief Strategist, Manager of the Technology Architecture Management Office (Ministry of Transportation), and Senior Business Analyst (Ministry of Consumer and Commercial Relations). -

Funding Arts and Culture Top-10 Law Firms
TORONTO EDITION FRIDAY, DECEMBER 16, 2016 Vol. 20 • No. 49 2017 budget overview 19th annual Toronto rankings FUNDING ARTS TOP-10 AND CULTURE DEVELOPMENT By Leah Wong LAW FIRMS To meet its 2017 target of $25 per capita spending in arts and culture council will need to, not only waive its 2.6 per cent reduction target, but approve an increase of $2.2-million in the It was another busy year at the OMB for Toronto-based 2017 economic development and culture budget. appeals. With few developable sites left in the city’s growth Economic development and culture manager Michael areas, developers are pushing forward with more challenging Williams has requested a $61.717-million net operating proposals such as the intensifi cation of existing apartment budget for 2017, a 3.8 per cent increase over last year. neighbourhoods, the redevelopment of rental apartments with Th e division’s operating budget allocates funding to its implications for tenant relocation, and the redevelopment of four service centres—art services (60 per cent), museum and existing towers such as the Grand Hotel, to name just a few. heritage services (18 per cent), business services (14 per cent) While only a few years ago a 60-storey tower proposal and entertainment industries services (8 per cent). may have seemed stratospheric, the era of the supertall tower One of the division’s major initiatives for 2017 is the city’s has undeniably arrived. In last year’s Toronto law review, the Canada 150 celebrations. At the end of 2017 with the Canada 82- and 92-storey Mirvish + Gehry towers were the tallest 150 initiatives completed, $4.284-million in one-time funding buildings brought before the board. -
Minutes Licensing and Standards Committee LS11.1
1/31/12 2012-01-25 Minutes - Licensing and Standards Committee Minutes Licensing and Standards Committee Meeting No. 11 Contact Kelly McCarthy, Committee Administrator Meeting Date Wednesday, January 25, 2012 Phone 416-397-7796 Start Time 9:30 AM E-mail [email protected] Location Committee Room 1, City Hall Chair Councillor Cesar Palacio LS11.1 ACTION Referred Ward:All Clothing Drop Boxes Committee Decision The Licensing and Standards Committee referred this item to the Executive Director, Municipal Licensing and Standards, to report to the September 21, 2012 meeting of the Licensing and Standards Committee on the feasibility of a revised Clothing Drop Box by-law that either bans all drop boxes, or allows drop boxes and includes the following conditions: 1. Is comprehensive in that it licenses all clothing drop boxes within the City of Toronto with no exemptions. 2. Requires each box to display a sticker which is affixed to the box, must be renewed periodically and which clearly indicates that the box is licensed by the City of Toronto and meets the following conditions: a. Each box displays the municipal address of the property on which the box is located. b. Each box has the written permission of the owner of the property to be located on that property. c. A requirement that the box be emptied on a regular basis and be free of graffiti and otherwise maintained in an acceptable manner. d. That the operator shall maintain the property in the immediate vicinity of the box in a clean and tidy manner, free of litter and debris. -
2010 Clerk's Official Declaration of Election Results
Ulli S. Watkiss City Clerk City Clerk’s Office City Hall, 13th Floor, West Tel: 416-392-8011 100 Queen Street West Fax: 416-392-4900 Toronto, Ontario M5H 2N2 Email: [email protected] Web: www.toronto.ca DECLARATION OF RESULTS OF VOTING MONDAY, OCTOBER 25, 2010 Pursuant to the provisions of Section 55(4) of the Municipal Elections Act, 1996, as amended, I, Ulli S. Watkiss, City Clerk of the City of Toronto, declare to be elected the candidate having received the highest number of votes for the office for which voting has been held, as shown in bold on the pages attached. In addition, I make the following declaration of the number of votes for each candidate as shown on the subsequent pages. Dated at the City of Toronto Ulli S. Watkiss this 28th day of October, 2010 City Clerk MAYOR CANDIDATE NAME VOTES ELECTED Rob Ford 383501 X George Smitherman 289832 Joe Pantalone 95482 Rocco Rossi 5012 George Babula 3273 Rocco Achampong 2805 Abdullah-Baquie Ghazi 2761 Michael Alexander 2470 Vijay Sarma 2264 Sarah Thomson 1883 Jaime Castillo 1874 Dewitt Lee 1699 Douglas Campbell 1428 Kevin Clarke 1411 Joseph Pampena 1319 David Epstein 1202 Monowar Hossain 1194 Michael Flie 1190 Don Andrews 1032 Weizhen Tang 890 Daniel Walker 804 Keith Cole 801 Michael Brausewetter 796 Barry Goodhead 740 Tibor Steinberger 735 Charlene Cottle 733 Christopher Ball 696 James Di Fiore 655 Diane Devenyi 629 John Letonja 592 Himy Syed 582 Carmen Macklin 575 Howard Gomberg 477 David Vallance 444 Mark State 438 Phil Taylor 429 Colin Magee 401 Selwyn Firth 394 Ratan Wadhwa 290 Gerald Derome 251 10/28/2010 Page 1 of 14 COUNCILLOR WARD NO.