Goh -CONDUCTIVE HEARING LOSS FINAL Version.Pptx
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: a Clinical Study
Int Adv Otol 2014; 10(2): 102-6 • DOI: 10.5152/iao.2014.40 Original Article A Post-Tympanoplasty Evaluation of the Factors Affecting Development of Myringosclerosis in the Graft: A Clinical Study Can Özbay, Rıza Dündar, Erkan Kulduk, Kemal Fatih Soy, Mehmet Aslan, Hüseyin Katılmış Department of Otorhinolaryngology, Şifa University Faculty of Medicine, İzmir, Turkey (CÖ) Department of Otorhinolaryngology, Mardin State Hospital, Mardin, Turkey (RD, EK, KFS, MA) Department of Otorhinolaryngology, Katip Çelebi University Atatürk Training and Research Hospital, İzmir, Turkey (HK) OBJECTIVE: Myringosclerosis (MS) is a pathological condition characterized by hyaline degeneration and calcification of the collagenous structure of the fibrotic layer of the tympanic membrane, which may develop after trauma, infection, or inflammation as myringotomy, insertion of a ventila- tion tube, or myringoplasty. The aim of our study was to both reveal and evaluate the impact of the factors that might be effective on the post-tym- panoplasty development of myringosclerosis in the graft. MATERIALS and METHODS: In line with this objective, a total of 108 patients (44 males and 64 females) aged between 11 and 66 years (mean age, 29.5 years) who had undergone type 1 tympanoplasty (TP) with an intact canal wall technique and type 2 TP, followed up for an average of 38.8 months, were evaluated. In the presence of myringosclerosis, in consideration of the tympanic membrane (TM) quadrants involved, the influential factors were analyzed in our study, together with the development of myringosclerosis, including preoperative factors, such as the presence of myringosclerosis in the residual and also contralateral tympanic membrane, extent and location of the perforation, and perioperative factors, such as tympanosclerosis in the middle ear and mastoid cavity, cholesteatoma, granulation tissue, and type of the operation performed. -

The Incudomalleolar Articulation in Down Syndrome (Trisomy 21): a Temporal Bone Study
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2015 The incudomalleolar articulation in down syndrome (trisomy 21): a temporal bone study Fausch, Christian ; Röösli, Christof Abstract: HYPOTHESIS: One reason for conductive hearing loss (HL) in patients with Down syndrome (DS) is structural anomalies in the incudomalleolar joint (IMJ) that impair sound transmission. BACK- GROUND: The majority of hearing losses in patients with DS are conductive. One reason is the high incidence of inflammatory processes such as otitis media. However, in some patients, the middle earseems to be normal. The assumption of structural disorders causing a HL is supported by a previous study revealing structural abnormalities of the incudostapedial joint (ISJ) in these patients. METHODS: In a retrospective analysis, histologic sections of the IMJ of 16 patients with DS were compared with 24 age- and sex-matched subjects with normal middle ear ossicles. The length of 8 parameters of the IMJ were measured at 3 positions and compared between the 2 groups. RESULTS: Age (p = 0.318) and sex distri- bution (p = 1) for the DS group and the matched controls were comparable. The IMJs (p < 0.001) and the cartilage of patients with DS are significantly wider in most measurements compared with controls. However, the joint space is not significantly different in the 2 groups. CONCLUSION: Conductive HL might be caused by a significantly wider IMJ in patients with DS supporting the findings of aprevious study reporting similar findings for the ISJ. The etiology of these findings is unclear. -
Tympanic Membrane Perforations: the Safe Versus the Unsafe
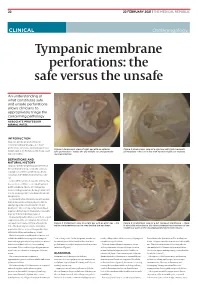
TMR_210222_22 2021-02-12T14:56:54+11:00 22 22 FEBRUARY 2021 | THE MEDICAL REPUBLIC CLINICAL Otolaryngology Tympanic membrane perforations: the safe versus the unsafe An understanding of what constitutes safe and unsafe perforations allows clinicians to appropriately triage the concerning pathology ASSOCIATE PROFESSOR NIRMAL PATEL INTRODUCTION Tympanic membrane perforations are seen frequently in general practice. Some perforations can be associated with significant Figure 1: Endoscopic view of right ear with an anterior Figure 2: Endoscopic view of a right ear with twin traumatic disease, such as cholesteatoma which may cause safe perforation – notice the dry middle ear and posterior perforations – the ear is dry with normal middle ear mucosa. major morbidity. myringosclerosis DEFINITIONS AND NATURAL HISTORY Tympanic membrane perforations are holes in the ear drum that most commonly occur as a consequence of either ear infections, chronic eustachian tube dysfunction or trauma to the ear. Acute middle ear infection (acute otitis media) is a common condition occurring at least once in 80% of children. Most acute otitis media resolves with spontaneous discharge of infected secretions through the eustachian tube into the nasopharynx. Occasionally when the infections are frequent, there is extensive scarring (tympanosclerosis and myringosclerosis) of the ear drum and middle ear . This scarring compromises blood supply to the healing ear drum and occasionally stops the hole from healing. (Figure 1) Traumatically induced holes occur from a rapid compression of the air column in the external ear canal, most commonly from a blow to the Figure 3: Endoscopic view of a right ear with an attic wax – the Figure 4: Endoscopic view of a left tympanic membrane – there white cholesteatoma can be seen behind the ear drum. -

Redalyc.Deviant Facial Nerve Course in the Middle Ear Cavity
Brazilian Journal of Otorhinolaryngology ISSN: 1808-8694 [email protected] Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico- Facial Brasil Cho, Jungkyu; Choi, Nayeon; Hwa Hong, Sung; Moon, Il Joon Deviant facial nerve course in the middle ear cavity Brazilian Journal of Otorhinolaryngology, vol. 81, núm. 6, 2015, pp. 681-683 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=392442695018 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Document downloaded from http://bjorl.elsevier.es day 25/11/2015. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. Braz J Otorhinolaryngol. 2015;81(6):681---683 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org CASE REPORT ଝ Deviant facial nerve course in the middle ear cavity Trajeto anômalo do nervo facial na cavidade da orelha média ∗ Jungkyu Cho, Nayeon Choi, Sung Hwa Hong, Il Joon Moon Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Received 27 December 2014; accepted 17 March 2015 Available online 7 September 2015 Introduction (Fig. 1A). Other physical exams showed no facial nerve palsy or auricular anomaly (Fig. 1B). Pure-tone average Anomalous facial nerve (FN) course can be found in a sig- (0.5, 1, 2, and 3 kHz) showed air-bone gap of 58 dB nificant number of cases with aural anomalies. -

ICD-9 Diseases of the Ear and Mastoid Process 380-389
DISEASES OF THE EAR AND MASTOID PROCESS (380-389) 380 Disorders of external ear 380.0 Perichondritis of pinna Perichondritis of auricle 380.00 Perichondritis of pinna, unspecified 380.01 Acute perichondritis of pinna 380.02 Chronic perichondritis of pinna 380.1 Infective otitis externa 380.10 Infective otitis externa, unspecified Otitis externa (acute): NOS circumscribed diffuse hemorrhagica infective NOS 380.11 Acute infection of pinna Excludes: furuncular otitis externa (680.0) 380.12 Acute swimmers' ear Beach ear Tank ear 380.13 Other acute infections of external ear Code first underlying disease, as: erysipelas (035) impetigo (684) seborrheic dermatitis (690.10-690.18) Excludes: herpes simplex (054.73) herpes zoster (053.71) 380.14 Malignant otitis externa 380.15 Chronic mycotic otitis externa Code first underlying disease, as: aspergillosis (117.3) otomycosis NOS (111.9) Excludes: candidal otitis externa (112.82) 380.16 Other chronic infective otitis externa Chronic infective otitis externa NOS 380.2 Other otitis externa 380.21 Cholesteatoma of external ear Keratosis obturans of external ear (canal) Excludes: cholesteatoma NOS (385.30-385.35) postmastoidectomy (383.32) 380.22 Other acute otitis externa Excerpted from “Dtab04.RTF” downloaded from website regarding ICD-9-CM 1 of 11 Acute otitis externa: actinic chemical contact eczematoid reactive 380.23 Other chronic otitis externa Chronic otitis externa NOS 380.3 Noninfectious disorders of pinna 380.30 Disorder of pinna, unspecified 380.31 Hematoma of auricle or pinna 380.32 Acquired -

Hearing Loss, Vertigo and Tinnitus
HEARING LOSS, VERTIGO AND TINNITUS Jonathan Lara, DO April 29, 2012 Hearing Loss Facts S Men are more likely to experience hearing loss than women. S Approximately 17 percent (36 million) of American adults report some degree of hearing loss. S About 2 to 3 out of every 1,000 children in the United States are born deaf or hard-of-hearing. S Nine out of every 10 children who are born deaf are born to parents who can hear. Hearing Loss Facts S The NIDCD estimates that approximately 15 percent (26 million) of Americans between the ages of 20 and 69 have high frequency hearing loss due to exposure to loud sounds or noise at work or in leisure activities. S Only 1 out of 5 people who could benefit from a hearing aid actually wears one. S Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old. Hearing Loss Facts S There is a strong relationship between age and reported hearing loss: 18 percent of American adults 45-64 years old, 30 percent of adults 65-74 years old, and 47 percent of adults 75 years old or older have a hearing impairment. S Roughly 25 million Americans have experienced tinnitus. S Approximately 4,000 new cases of sudden deafness occur each year in the United States. Hearing Loss Facts S Approximately 615,000 individuals have been diagnosed with Ménière's disease in the United States. Another 45,500 are newly diagnosed each year. S One out of every 100,000 individuals per year develops an acoustic neurinoma (vestibular schwannoma). -

Intratympanic Membrane Cholesteotoma: an Unusual Rare Case
Central Journal of Ear, Nose and Throat Disorders Bringing Excellence in Open Access Case Report *Corresponding author Mohamad Ali El Natout, Department of Otolaryngology Head & Neck Surgery, American University of Beirut Intratympanic Membrane Medical Center, P.O.Box: 11-0236, Riad El-Solh, Beirut 1107 2020, Beirut-Lebanon, USA, Tel: 96-133-449-66; Email: Cholesteotoma: An Unusual Submitted: 11 July 2016 Accepted: 23 July 2016 Rare Case Published: 01 August 2016 Copyright 1 2 1 Hayat Adib , Tamer El Natout , and Mohamad Ali El Natout * © 2016 El Natout et al. 1Department of Otolaryngology Head & Neck Surgery, American University of Beirut Medical Center, USA OPEN ACCESS 2Faculty of Medicine, American University of Beirut, USA Keywords • Intratympanic membrane Abstract • Cholesteatoma • Acquired Intraympanic membrane cholesteotoma without a preceding ear trauma or surgery is a rare entity. Only few cases have been documented in the literature. The exact etiology of this lesion is still unclear. We report an unusual case of an intratympaniccholesteatoma in an adult patient. He is a 45-year-old male who presented with ear fullness and hearing loss six months following an acute otitis media without otorrhea or a tympanic membrane perforation. Physical exam showed a central whitish area on the tympanic membrane. CT scan demonstrated thickening of the tympanic membrane. On the audiogram, he had a 20-dB air-bone gap; tympanogram showed a B-curve. We surgically explored his middle ear and encountered a central tympanic membrane 5X3 mm cholesteatoma with intact middle ear cavity. Accordingly we performed a tympanoplasty. The gold standard for diagnosis of tympanic membrane cholesteotoma is oto-microscopy. -

Doctoral Dissertation Template
UNIVERSITY OF OKLAHOMA GRADUATE COLLEGE MECHANICAL PROPERTIES OF HUMAN INCUDOSTAPEDIAL JOINT AND TYMPANIC MEMBRANE IN NORMAL AND BLAST-DAMAGED EARS A DISSERTATION SUBMITTED TO THE GRADUATE FACULTY in partial fulfillment of the requirements for the Degree of DOCTOR OF PHILOSOPHY By SHANGYUAN JIANG Norman, Oklahoma 2018 MECHANICAL PROPERTIES OF HUMAN INCUDOSTAPEDIAL JOINT AND TYMPANIC MEMBRANE IN NORMAL AND BLAST-DAMAGED EARS A DISSERTATION APPROVED FOR THE STEPHENSON SCHOOL OF BIOMEDICAL ENGINEERING BY ______________________________ Dr. Rong Z. Gan, Chair ______________________________ Dr. Vassilios I. Sikavitsas ______________________________ Dr. Matthias U. Nollert ______________________________ Dr. Edgar A. O’Rear ______________________________ Dr. Harold L. Stalford © Copyright by SHANGYUAN JIANG 2018 All Rights Reserved. I dedicate my dissertation work to my family. Acknowledgements I would like to express my sincere appreciation to my advisor, Dr. Rong Z. Gan for the enormous amount time, energy, resource, and patience she had devoted in my training process. I joined the Ph.D. program at the University of Oklahoma right after I got my bachelor degree and with great language difficulties. Dr. Gan has been teaching me how to think, read, learn and write as a researcher regardless of my weak background since the first day I arrived in the US. Her respect, enthusiasm, and persistence to work has deeply impressed me and changed my attitude towards my work and life. The past five years in the biomedical engineering laboratory is one of the most precious experiences in my life. I would like to express my appreciation to my committee members, Dr. Vassilios I. Sikavitsas, Dr. Matthias U. Nollert, Dr. Edgar A. -

Treatment of a Traumatic Incudomalleolar Joint Subluxation with Hydroxyapatite Bone Cement Dennis Bojrab II 1, Jennifer F Ha2,3,4,5*, David a Zopf 1
Annals of International Case Report Case Report Open Access | Research Treatment of A Traumatic Incudomalleolar Joint Subluxation with Hydroxyapatite Bone Cement Dennis Bojrab II 1, Jennifer F Ha2,3,4,5*, David A Zopf 1 1Department of Paediatrics Otolaryngology Head & Neck Surgery, University of Michigan Health System, C.S. Mott Children’s Hospital, 1540 East Hospital Drive, Ann Arbor, Michigan 48109, United States of America 2Department of Paediatrics Otolaryngology Head & Neck Surgery, Perth Children’s Hospital, Roberts Road, Nedlands 6009, Western Australia 3Murdoch ENT, Wexford Medical Centre, St John of God Hospital (Murdoch), Suite 17-18, Level 1, 3 Barry Marshall Parade, Murdoch 6150, West- ern Australia 4School of Surgery, University of Western Australia, Stirling Highway, Crawley 6009, Western Australia 5 St John of God Hospital (Murdoch), Wexford Medical Centre, Suite 17-18, Level 1, 3 Barry Marshall Parade, Murdoch 6150, Western Australia Abstract Trauma-related hearing loss can be conductive, sensorineural, or mixed in nature. Alteration of any of the conductive mechanisms can result in a conductive hearing loss. Depending on the location and type of ossicular injury there several reconstructive options have been described. Hydroxyapetite cement has been reported on several occasions for incudostapedial dislocation, however, rare- ly/never for incudomalleolar dislocation. Here we report a patient with traumatic Incudomalleolar Joint (IMJ) separation which was successfully repaired using bone cement. Case Description A 15-year-old male patient was referred to our Paediatric Otolaryngology department by his paediatrician with a lifelong history of left sided hearing loss. He was involved in two motor vehicle accidents when he was younger. -

Neurootological Evaluation of Tinnitus
International Tinnitus Journal 1, 93-97 (1995) Neurootological Evaluation of Tinnitus J. c. R. Seabra, M.D., H. Diamantino, M.D., J. Faria e Almeida, M.D. Ear, Nose and Throat Department, Vila Nova de Gaia, Portugal Abstract: We analyse the neurootological data of patients attended in the Ear, Nose and Throat (E.N.T.) department of the Centro Hospitalar de Vila Nova de Gaia for a tinnitus problem. We submitted these patients to our neurootological routine evaluation. This approach is justified in a tinnitus patient because the cochleovestibular system is a unit and acts as a whole. We characterise the population that came to us by sex and mean age. The profile of these patients is then analysed by our neurootological routine evaluation, which comprises the history taking and audiometric as well as equilibriometric investigations. The results of the audiovestibulometric examinations - pure tone audiometry, vocal audiometry, and Brain Evoked Response Audiometry (B.E.R.A.), Cranio-Corpo Graphy (C.C.G.), Electronystagmography (E.N.G.) - are discussed. We concluded that many tinnitus patients, even those who had no vestibular symptoms, showed some disturbances in the vestibular tests. This fact highlights the need for a complete cochleovestibular investigation in all patients complaining about tinnitus. INTRODUCTION middle ear disease, such as chronic otitis, tympanic perforations, or tympanosclerosis. innitus is a widespread symptom that mortifies We investigated 44 patients, 19 men and 25 women, with T patients and frustrates doctors. It may be the only a mean age of 48-years (standard deviation being 12). symptom complained by patients, but commonly The patients underwent our routine neurootological it is associated with neurosensory hearing loss and/or examination which comprises: vertigo. -

Differential Diagnosis and Treatment of Hearing Loss JON E
Differential Diagnosis and Treatment of Hearing Loss JON E. ISAACSON, M.D., and NEIL M. VORA, M.D., Milton S. Hershey Medical Center, Hershey, Pennsylvania Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be cat- egorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hear- ing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (Am Fam Physician 2003;68:1125-32. Copyright© 2003 American Academy of Family Physicians) ore than 28 million Amer- tive, the sound will be heard best in the icans have some degree of affected ear. If the loss is sensorineural, the hearing impairment. The sound will be heard best in the normal ear. differential diagnosis of The sound remains midline in patients with hearing loss can be sim- normal hearing. Mplified by considering the three major cate- The Rinne test compares air conduction gories of loss. Conductive hearing loss occurs with bone conduction. The tuning fork is when sound conduction is impeded through struck softly and placed on the mastoid bone the external ear, the middle ear, or both. Sen- (bone conduction). When the patient no sorineural hearing loss occurs when there is a longer can hear the sound, the tuning fork is problem within the cochlea or the neural placed adjacent to the ear canal (air conduc- pathway to the auditory cortex. -

Imaging of Temporal Bone Trauma
Imaging of Temporal Bone Trauma Tabassum A. Kennedy, MD*, Gregory D. Avey, MD, Lindell R. Gentry, MD KEYWORDS Temporal bone fracture Trauma Ossicular injury Hearing loss Facial nerve Cerebrospinal fluid leak Pneumolabyrinth Perilymphatic fistula KEY POINTS Multidetector temporal bone computed tomography examinations should be performed in patients with a clinical or radiographic suspicion of temporal bone fracture. Categorization of temporal bone fractures should include a descriptor for fracture direction, the presence or absence of labyrinthine involvement, and the segment of temporal bone involved. It is important to identify associated complications related to temporal bone trauma that will guide management. Complications include injury to the tympanic membrane, ossicular chain, vestibulo- cochlear apparatus, facial nerve, tegmen, carotid canal, and venous system. INTRODUCTION evaluation with a noncontrast CT examination of the head. Careful scrutiny of the temporal bone The temporal bone is at risk for injury in the setting on head CT is necessary to detect primary and of high-impact craniofacial trauma occurring in 3% secondary signs of temporal bone injury. External to 22% of patients with trauma with skull fractures 1–3 auditory canal opacification, otomastoid opacifi- (Table 1). Motor vehicle collisions, assaults, cation, air within the temporomandibular joint, and falls are the most common mechanisms of 4–6 ectopic intracranial air adjacent to the temporal injury. Most patients with temporal bone trauma bone, and pneumolabyrinth in the setting of sustain unilateral injury, occurring in 80% to 90% 5,7,8 trauma should raise the suspicion of an associated of cases. Multidetector computed tomography temporal bone fracture (Fig. 1). Patients with (CT) has revolutionized the ability to evaluate the temporal bone trauma often sustain concomitant intricate anatomy of the temporal bone, enabling intracranial injury, which often necessitates more clinicians to detect fractures and complications emergent management.