Asymmetry of Authority Or Information Underlying Insufficient Communication Associated with a Risk of Crashes Or Incidents in Pa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

West Japan Railway Group Integrated Report 2019 —Report on Our Value for Society—
Continuity Progress Making Our Vision into Reality West Japan Railway Group Integrated Report 2019 —Report on Our Value for Society— West Japan Railway Company Contents 2 On the publication of “JR-West Group Integrated Report 2019” 3 Values held by the JR-West Group Our Starting Point 5 The derailment accident on the Fukuchiyama Line 11 Recovering from heavy rain damage through cooperation and think-and-act initiatives 13 Business activities of JR-West Group 15 The president’s message 17 The value we seek to provide through the non-railway business —Messages from group company Presidents Strategy of 21 Steps toward our vision 21 JR-West Group Medium-Term Management Plan 2022: approach & overview Value Creation 23 Toward long-term sustainable growth for Our Vision 25 Progress on Groupwide strategies—example initiatives 27 Promoting our technology vision 29 Special Three-Way Discussion The challenge of evolving in the railway/transportation field in an era of innovation 33 Fiscal 2019 performance in priority CSR fields and fiscal 2020 plans for priority initiatives 37 Safety 47 Customer satisfaction 51 Coexistence with communities A Foundation 55 Human resources/motivation Supporting 59 Human rights Value Creation 61 Global environment 67 Risk management 71 Corporate governance 73 Special Three-Way Discussion The role of the Board of Directors in achieving sustainable growth and enhancing corporate value 77 Initiatives in each business 81 Consolidated 10-year financial summary Data 83 Financial statements 87 Recognizing and responding to risks and opportunities 88 Data related to human resources and motivation (non-consolidated) Corporate profile (as of March 31, 2019) Scope As a rule, JR-West Group (including some Company name West Japan Railway Company initiatives at the non-consolidated level). -

Inori No Mori the Site of the Accident on the Fukuchiyama Line and The
Inori no Mori, The Site of the Accident Information on the Fukuchiyama Line and the Memorial ■ Inori no Mori is open every day from 8:00 am to 8:00 pm. Please note that it way be temporarily closed, such as under heavy weather condition. On April 25, 2005, we at the West Japan Railway Company caused the Accident on the Fukuchiyama Line, ■ You are requested to write your name in the visitors' book when you come to Inori no Mori. an extremely serious accident which claimed 106 lives and left more than 500 injured. We continue to honor the ■ Tables to place flowers in memory of the victims are memory of those whose lives were lost, and we offer our located in front of the cenotaph and by the northeast sincerest and most heartfelt apologies and condolences corner of the apartment building. to the bereaved families, all those who were injured and ■ Please show respect for its purpose and observe the following their families. rules and etiquette. Inori no Mori We would also like to offer our sincere apologies to those The Site of the Accident on the living in the vicinity of the accident and anyone else Fukuchiyama Line and the Memorial whom we affected in any way through our hand in this No cameras No smoking No food or drinks No sports/playing No pets tragic event. Furthermore, we extend our deepest gratitude to the police, firefighters, Japan Self-Defense ● Eating, drinking or smoking is only permitted in the Forces, medical personnel and institutions, nearby rest area located inside the building. -
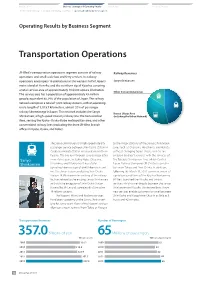
Operating Results by Business Segment — —
Introduction Business Strategy and Operating Results ESG Section Financial Section The President’s Message Medium-Term Management Plan Operating Results by Business Segment — — Operating Results by Business Segment Transportation Operations JR-West’s transportation operations segment consists of railway Railway Revenues operations and small-scale bus and ferry services. Its railway operations encompass 18 prefectures in the western half of Japan’s Sanyo Shinkansen main island of Honshu and the northern tip of Kyushu, covering a total service area of approximately 104,000 square kilometers. Other Conventional Lines The service area has a population of approximately 43 million people, equivalent to 34% of the population of Japan. The railway network comprises a total of 1,222 railway stations, with an operating route length of 5,015.7 kilometers, almost 20% of passenger railway kilometerage in Japan. This network includes the Sanyo Kansai Urban Area Shinkansen, a high-speed intercity railway line; the Kansai Urban (including the Urban Network) Area, serving the Kyoto–Osaka–Kobe metropolitan area; and other conventional railway lines (excluding the three JR-West branch offices in Kyoto, Osaka, and Kobe). The Sanyo Shinkansen is a high-speed intercity to the major stations of the Sanyo Shinkansen passenger service between Shin-Osaka Station in Line, such as Okayama, Hiroshima, and Hakata, Osaka and Hakata Station in Fukuoka in northern without changing trains. These services are Kyushu. The line runs through several major cities enabled by direct services with the services of Sanyo in western Japan, including Kobe, Okayama, the Tokaido Shinkansen Line, which Central Shinkansen Hiroshima, and Kitakyushu. -

Recent Trends in Japanese Transportation Masahiro Sugiyama
Recent Trends in Japanese Transportation Masahiro Sugiyama 1. Countermeasures for Natural Disasters 2004 was a year with an unusually high occurrence of natural disasters. There were 10 typhoons from June and the country was visited by heavy rains in the Niigata/Fukushima region and Fukui region in July. The disasters led to more than 230 dead or missing and almost 170,000 homes immersed in water. In October, the Chuetsu Earthquake with an intensity of 7 rocked the country, resulting in 40 deaths and the evacuation of over 100,000 people. In December, furthermore, the Sumatra-Andaman Earthquake and ensuing tsunami, led to approximately 100,000 dead or missing in 10 countries around the Indian Ocean. Many Japanese were among the victims. Faced with such a serious situation, the annual White Paper on Land, Infrastructure and Transport in Japan 2005 published in fiscal 2004 mentions the disaster recovery countermeasures and rebuilding support offered by the national government and the Ministry of Land, Infrastructure and Transport under the title of "Aiming to Build a Country Resilient to Disasters." This attempt was made to actively respond to social needs, and discussion includes actions taken against heavy rains and typhoons, earthquakes and tsunamis. Chuetsu Earthquake It is essential to quickly restore damaged lifelines such as transportation in (Collapsed lane on Kan-etsu Expressway)� (Photograph: Japan Highway Public Corporation Hokuriku � affected areas as stated in the White Paper. Confirmation made through Branch) Traffic in Japan -

Notice of the 32Nd Ordinary General Meeting of Shareholders
(Translation) NOTICE OF THE 32ND ORDINARY GENERAL MEETING OF SHAREHOLDERS To Our Shareholders: We should like to extend our heartfelt gratitude for your continued understanding of business operations of West Japan Railway Group (the "Group"). The Group very seriously takes its responsibility for the train accident on the Fukuchiyama Line we caused on April 25, 2005 and the gravity of its consequences, and has continued to implement various measures in terms of both physical and intangible aspects to improve safety. In consideration of this, I, as well as all officers and employees of the Group, have determined to continue to faithfully perform our roles in our respective positions with a sense of responsibility to build a safer railway system. Last year, the Group launched a "JR-West Group Medium-Term Management Plan 2022" and its core component, a "JR-West Group Railway Safety Think-and-Act Plan 2022." Based on our resolve never to cause another accident like that on the Fukuchiyama Line, we will implement plans toward the realization of our corporate philosophy and management vision and contribute to the creation of "a safe and comfortable society filled with meetings among people and smiles" which is our vision. With regard to shareholder returns, we will pay stable dividends, aiming for a dividend payout ratio of approximately 35% in the fiscal year ending March 31, 2023. In addition, over the aggregate period up to March 31, 2023, the Company's yardstick will be a total return ratio of approximately 40%, and we will make flexible acquisitions of treasury stock. During the fiscal year under review, we acquired and cancelled 1,253,600 shares of common stock of the Company. -

Northern and Western Kinki Region Shuichi Takashima
Railwa Railway Operators Railway Operators in Japan 11 Northern and Western Kinki Region Shuichi Takashima Keihanshin economic zone based on a from cities in the south. As a result, the Region Overview contraction of the Chinese characters population density in these northern forming parts of each city name. areas is low, despite the proximity to This article discusses railway lines in parts However, to some extent, each city is still Keihanshin. Shiga Prefecture borders the of four prefectures in the Kinki region: an economic entity in its own right, eastern side of Kyoto Prefecture and has Shiga, Kyoto, Osaka and Hyogo. The making the region somewhat different long played a major role as a three largest cities in these four prefectures from the huge conurbation of transportation route to eastern Japan and are Kyoto, Osaka and Kobe. Osaka was Metropolitan Tokyo. the Hokuriku region. y Japan’s most important commercial centre Topography is the main reason for this until it was surpassed by Tokyo in the late difference. Metropolitan Tokyo spreads 19th century. Kyoto is the ancient capital across the wide Kanto Plain, while Kyoto, Outline of Rail Network (where the Emperors resided from the 8th Osaka and Kobe are separated by Operators to 19th centuries), and is rich in historical highlands that (coupled with the nearby The region’s topography has determined sites and relics. Kobe had long been a sea and rivers) have prevented Keihanshin the configuration of the rail network. In major domestic port and became the most from expanding to the same extent as the Metropolitan Tokyo, lines radiate like important international port serving Metropolitan Tokyo. -

Living in Okayama Access to Okayama University 岡山を知る、日本を知る。
Discover Okayama, Discover Nippon. Living in Okayama Access to Okayama University 岡山を知る、日本を知る。 Accommodation Japan SAPPORO Your room is a single room SEOUL equipped with a desk, a chair, a wardrobe, a bed (linens NOT included), a SHANGHAI bathroom with shower facilities (including a bathtub and a toilet), a OKAYAMA refrigerator, a kitchenette, TOKYO AIR LINE and an air-conditioner. OSAKA SHINKANSEN GUAM From Tokyo by airplane from Haneda Airport 1h20min TAIPEI by Nozomi Shinkansen 3h20min NAHA From Osaka by Nozomi Shinkansen 45min E XCHANGE P ROGRAM OKAYAMA the Chugoku region Okayama City JAPAN SEA N To Tsuyama Handayama Estimated monthly Living Expenses Tottori Tsuyama TOTTORI To Line Matsue Yonago Prefecture TSUSHIMA Okayama CAMPUS Airport Route 53 To Shin Osaka Rent (dormitory) 15,000 OKAYAMA Sanyo Shinkansen Prefecture To Himeji Tsuyama HYOGO Center for Niimi Prefecture Global Partnerships Sanyo Main Line Utility 8,000 Okayama & Education Airport Tsushima Himeji Aioi Kibi Line Korakuen Campus Garden HIROSHIMA To Hiroshima Okayama Food 25,000 Prefecture Station Okayama To Soja Enjoy Shikata Campus Shin-Kurashiki Kurashiki To Kurashiki N Okayama City Hall Transportation 0 the Fukuyama Syoudoshima bike life Takamatsu Seto Ohashi Sakaide Line SHIKATA Miscellaneous 10,000 SETO INLAND SEA CAMPUS KAGAWA Prefecture To Takamatsu Asahi River (yen) ≒ Total 58,000 (120yen 1$) 25min, by bus from Okayama Airport as of May 2015 Tsushima Campus 7min, by bus from Okayama Station Shikata Campus 5min, by bus from Okayama Station Scholarship Contact Student Exchange Program Section ¥ 30,000 ~ 80,000 per month Center for Global Partnerships & Education, Okayama University Email : [email protected] 2-1-1 Tsushima Naka, Kita-ku, Okayama 700-8530, Japan ※This amount is subject to change in accordance with the yearly the University budget Printed in Japan. -

Annual Report 2015 Year Ended March 31, 2015 Profile
Annual Report 2015 Year ended March 31, 2015 Profile JR-West at a Glance Transportation Operations Non-Transportation Operations Railway and Real Estate and Bus and Ferry Services Retail Business Transportation Operations Non-Transportation Operations Shinkansen Operating Revenues Retail Business by Business Segment (from Third Parties) (Consolidated) Kansai Urban Area Real Estate Business Other Conventional Lines Other Businesses Fiscal 2015 (Year Ended March 31, 2015) Total ¥1,350.3 billion Bus and Ferry Services West Japan at a Glance JR-West’s railway network covers 18 prefectures in the western half of the island of Honshu and the northern tip of the island of Kyushu, and comprises 20% of Japan’s land area. The area we serve is home to approximately 43.1 million people, about 34% of the country’s population, and has a nominal GDP of ¥159 trillion. It also sees visits by 897 million tourists annually. GDP Population Tourists ¥159 trillion 43.1million 897 million Yonago West Japan Area Hiroshima Okayama Hakata Our History Contents West Japan Railway Company (JR-West) is one of the six 2 Introduction Overview ....................................................................................... 2 passenger railway transport companies created in 1987, Financial Highlights ................................................................. 4 when Japanese National Railways was split up and privatized. Non-financial Highlights ....................................................... 6 In our railway operations, which are our core business 8 Business Strategy and Operating Results activity, our railway network extends over a total of 5,007.1km. The President’s Message ........................................................ 8 ...... 10 Making the most of the various forms of railway asset value Medium-Term Management Plan 2017 —Update— Operating Results by Business Segment ..................... -
Guide Book (PDF)
■竹内街道・横大路・大路「お楽しみガイド」 H1-H4 Access Map for Takenouchi Kaido / Yokooji Discover Japan’s oldest public road and enjoy its history, cuisine, experiences, and more… JR Takarazuka Line (Fukuchiyama Line) ➡ Fukuchiyama Demachiyanagi ➡ Hankyu Takarazuka Line Takarazuka Fukuchiyama Sanjo Hankyu Kyoto Line Kawaramachi Senri-Chuo Bampaku-kinen-koen Osaka Gion-shijo Itami JR Kyoto Line (Tokaido Line) Hankyu International Hotarugaike Ibaraki Imazu Line Airport (Itami Airport) Esaka Maibara ➡ ➡ Minami-ibaraki Shin-Kobe, Hakata JR San-yo Shinkansen JR Tokaido Shinkansen Shin-Osaka Kyoto JR Osaka Higashi Line Osaka Monorail Line Nagoya, Nishinomiya-kitaguchi Hankyu Kobe Line Tokyo ➡ ➡ Tofukuji Juso Kosoku-Kobe ➡ Kobe-sannomiya Kobe Amagasaki JR Kobe Line Tambabashi Guide to Attractions Sannomiya Osaka Kintetsu- (Umeda) Hanshin Main Line Keihan Line Tambabashi ➡ Kobe-Sannomiya Amagasaki Kosoku-Kobe Kadoma-shi JR Nara JR Tozai Line Kyobashi Line Nishinomiya Imazu Kintetsu Kyoto Line Hanaten Yodoyabashi JR Gakkentoshi Line Nishikujo Sakurajima Shigino Kizu Kamo ➡ Kobe Hommachi Osaka Metro Chuo Line Takaida Kintetsu Keihanna Line Airport Benten-cho Tanimachi 4-chome Morinomiya Takaida-Chuo Nagata Kintetsu- Hanshin Namba Line Osaka-Namba Osaka-Uehommachi Kintetsu Nara Line Yamato-Saidaiji Nara JR-Namba Namba Tsuruhashi Fuse Ikoma J Nara R O s Kintetsu a k Ikoma Line a Lo op Osaka Bay L Naniwa Daido ine Shin-Imamiya Kashiwara Oji Kintetsu Osaka Metro Tennoji JR Yamatoji Line Midosuji Line Kyuhoji Kashihara Line Osaka- JR Tengachaya Abenobashi Sakurai Kintetsu -

2011 Annual Report
GROUP STRATEGY REVIEW OF OPERATIONS AS A CORPORATE CITIZEN DOMESTIC AND INTERNATIONAL PERSPECTIVES FINANCIAL SECTION TION C For the year ended March 31, 2011 Annual Report 2011 ONSTRU C E R CREATIVE CREATIVE KEY FIGURES TO BETTER UNDERSTAND JR EAST *Figures are as of March 31, 2011 Consolidated operating revenues, ¥2,537.4 billion On a daily basis about 17 million passengers travel a network of 70 train lines stretching 7,512.6 operating kilometers 92 stations are used by more than 100,000 passengers a day Total safety-related investments in the 24 years since JR East’s founding, about ¥2.5 trillion Open inside cover Jr east’s serVICE AREA TOKYO The new Hayabusa Series E5 super express railcars on the Tohoku Shinkansen Line will ultimately operate at a maximal speed of 320km/h Retail stores and restaurants in the stations, about 2,500 The number of Suica prepaid, rechargeable IC cards issued, about 35 million About 140,000 Open inside cover stores accept Suica electronic money Annual Report 2011 001 East Japan Railway Company (JR East) is the largest passenger railway company in the world, serving about 17 million passengers daily. JR East operates a five-route Shinkansen network between Tokyo and major cities in eastern Honshu (Japan’s main island). JR East has the ability to leverage passenger traffic and railway assets to develop non-transportation businesses. JR East alone provides nearly half of the huge volume of railway transportation in the Tokyo metropolitan area. HISTORY OF JR EAST April 1987 July 1992 March 1997 The Fukushima–Yamagata segment of the Yamagata Hybrid Shinkansen Line opens and the Tsubasa super-express begins service, marking the first Shinkansen through service to a conventional line. -

The Derailment Accident on the Fukuchiyama Line (PDF, 357KB)
Our Starting Point Our Starting Point Strategy of Value Creation for Our Vision A Foundation Supporting Value Creation Data The derailment accident on the Fukuchiyama Line On April 25, 2005, we at the West Japan Railway Company caused the Accident on the Fukuchiyama Line, an extremely We will continue to make concerted efforts for all persons affected by the accident, while striving to further enhance safety serious accident resulting in 106 fatalities and more than 500 injured passengers. We pray for all the victims of the accident measures and reform our corporate culture. and would like to express our sincerest apologies to their bereaved families. We would also like to express our deepest This accident has left an indelible mark on our hearts and we will continue drawing upon all of our capabilities to be sympathies and sincerest apologies to the injured passengers and their families. fully conscious of our responsibility for protecting the truly precious lives of our customers, and incessantly acting on the For the immense anxiety that the accident caused, we offer the deepest apology possible to our customers and those in basis of safety first, while building a railway that assures our customers of its safety and reliability. the local community. To Takarazuka * Arrows on cars indicate Overview the front of each car. Taking to heart the lessons from the accident Car 7 Date/time Monday, April 25, 2005, approx. 9:18 AM Because JR-West had never predicted an accident of this great magnitude before, we did not have an ATS (Automatic Train Weather conditions: sunny Car 6 Stop) system with speed check functions installed on the curve where the derailment occurred and we did not sufficiently take into account human factors in our employee training and similar programs. -

West Japan Railway Company Accident Type : Level Crossing
Railway accident investigation report Railway operator : West Japan Railway Company Accident type : Level crossing accident Date and time : About 8:21, February 13, 2015 Location : Hachinin-yama level crossing, class one level crossing, located at around 166,410 m from the origin at Kobe station, between Nishiachi station and Shin-Kurashiki station, double track, San-yo Line, Kurashiki City, Okayama Prefecture SUMMARY On February 13, 2015, the outbound local Electric 1731M train, composed of 6 vehicles, started from Okayama station bound for Fukuyama station, San-yo Line of West Japan Railway Company, departed from Nishiach station on schedule, 08:19. The driver of the train cruising with the speed of about 95 km/h, noticed the stop signal of the obstruction warning signal at Hachinin-yama level crossing and, at the same time, noticed the truck stopped in the level crossing, so that he immediately took an emergency brake and blew the whistle, but it was too late, the train collided with the truck and stopped at about 210 m passed the level crossing. There were about 300 passengers, the train driver and the conductor onboard the train, among them, 44 passengers and the train driver were injured, including one seriously injured passenger. The driver of the truck was not injured because he evacuated out of the level crossing when the collision occurred. The train was not derailed but damaged in the front part of the first vehicle and in the right side of the first and the second vehicles. The truck was seriously damaged but fire was not ignited.