Practice Preparatory Exam for Auriculotherapy Course
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sound and the Ear Chapter 2
© Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Chapter© Jones & Bartlett 2 Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION Sound and the Ear © Jones Karen &J. Kushla,Bartlett ScD, Learning, CCC-A, FAAA LLC © Jones & Bartlett Learning, LLC Lecturer NOT School FOR of SALE Communication OR DISTRIBUTION Disorders and Deafness NOT FOR SALE OR DISTRIBUTION Kean University © Jones & Bartlett Key Learning, Terms LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR Acceleration DISTRIBUTION Incus NOT FOR SALE OR Saccule DISTRIBUTION Acoustics Inertia Scala media Auditory labyrinth Inner hair cells Scala tympani Basilar membrane Linear scale Scala vestibuli Bel Logarithmic scale Semicircular canals Boyle’s law Malleus Sensorineural hearing loss Broca’s area © Jones & Bartlett Mass Learning, LLC Simple harmonic© Jones motion (SHM) & Bartlett Learning, LLC Brownian motion Membranous labyrinth Sound Cochlea NOT FOR SALE OR Mixed DISTRIBUTION hearing loss Stapedius muscleNOT FOR SALE OR DISTRIBUTION Compression Organ of Corti Stapes Condensation Osseous labyrinth Tectorial membrane Conductive hearing loss Ossicular chain Tensor tympani muscle Decibel (dB) Ossicles Tonotopic organization © Jones Decibel & hearing Bartlett level (dB Learning, HL) LLC Outer ear © Jones Transducer & Bartlett Learning, LLC Decibel sensation level (dB SL) Outer hair cells Traveling wave theory NOT Decibel FOR sound SALE pressure OR level DISTRIBUTION -

Specialized for Sound Detection A. Outer
EAR © 2019zillmusom I. Overview - specialized for sound detection A. Outer ear - funnel shaped structure of cartilage and skin that leads to Tympanic membrane; directs sound toward Tympanic membrane; helps detect source of sound. B. Middle ear - air filled chamber that contains bones (ossicles) that link Tympanic membrane to cochlea; also contains muscles that dampen sounds; middle ear is linked to Nasopharynx by auditory tube which allows for equilibration of air pressure on inner side of Tympanic membrane. C. Inner ear - fluid filled chamber in petrous part of temporal bone; inner ear contains Cochlea (hearing) and Vestibular apparatus for gravity detection (both innervated by CN VIII). Clinical Note: Functioning of inner ear can be tested independently by vibrations transmitted directly through bone (Weber test: tuning fork on calvarium is perceived as sound); CONDUCTIVE HEARING LOSS - damage to middle ear (tympanic membrane, auditory ossicles); SENSORINEURAL HEARING LOSS - damage to inner ear (cochlea, CN VIII). II. Outer Ear - composed of two parts: A. Auricle (pinna) - elastic cartilage covered with skin; functions to reflect sound waves. Parts: helix, antihelix, tragus and lobule. Decorative Note: Cartilage does not extend into Lobule; Lobule can be readily pierced to provide support for decorative metal objects. B. External auditory meatus - tube from auricle to the Tympanic membrane; posterior to Parotid gland and TMJ (Temporomandibular joint); located anterior to mastoid process. Outer third consists of elastic cartilage; contains hairs, sebaceous glands and ceruminous glands (produce cerumen = ear wax); serves to protect Tympanic membrane; Inner two thirds is composed of bone lined with skin. Clinical note: External auditory meatus is curved anteriorly in adults, is straight in children; in adults, auricle is pulled up and back to insert otoscope. -

ANATOMY of EAR Basic Ear Anatomy
ANATOMY OF EAR Basic Ear Anatomy • Expected outcomes • To understand the hearing mechanism • To be able to identify the structures of the ear Development of Ear 1. Pinna develops from 1st & 2nd Branchial arch (Hillocks of His). Starts at 6 Weeks & is complete by 20 weeks. 2. E.A.M. develops from dorsal end of 1st branchial arch starting at 6-8 weeks and is complete by 28 weeks. 3. Middle Ear development —Malleus & Incus develop between 6-8 weeks from 1st & 2nd branchial arch. Branchial arches & Development of Ear Dev. contd---- • T.M at 28 weeks from all 3 germinal layers . • Foot plate of stapes develops from otic capsule b/w 6- 8 weeks. • Inner ear develops from otic capsule starting at 5 weeks & is complete by 25 weeks. • Development of external/middle/inner ear is independent of each other. Development of ear External Ear • It consists of - Pinna and External auditory meatus. Pinna • It is made up of fibro elastic cartilage covered by skin and connected to the surrounding parts by ligaments and muscles. • Various landmarks on the pinna are helix, antihelix, lobule, tragus, concha, scaphoid fossa and triangular fossa • Pinna has two surfaces i.e. medial or cranial surface and a lateral surface . • Cymba concha lies between crus helix and crus antihelix. It is an important landmark for mastoid antrum. Anatomy of external ear • Landmarks of pinna Anatomy of external ear • Bat-Ear is the most common congenital anomaly of pinna in which antihelix has not developed and excessive conchal cartilage is present. • Corrections of Pinna defects are done at 6 years of age. -

KULAK ANATOMİSİ.Pdf
OMÜ SHMYO ANATOMİ KULAK ANATOMİSİ ÖĞR. GÖR. Dr. GÜRSEL AK GÜVEN DİLEK GÜN – 20460810 SELİN ÇETİNKAYA - 20460770 EDANUR ÇEPNİ - 20460780 RÜMEYSA İNAL -20460756 Auris Externa(Dış Kulak) Auris Media (Orta Kulak) Auris İnterna (İç Kulak) Auricula (Kulak Kepçesi) Cavitas Tympani (Timpan Labyrinthus Osseus (Kemik Boşluğu) Labirent) • Ligementa Auricularia • Auris Media’nın Duvarları • Vestibulum • Musculiauriculares • Canales Semicirculares • Auricula’nın Duyu Sinirleri Membrana Tympanica • Cochlea • Auricula’nın Arterleri (Kulak Zarı) • Arterleri Labyrinthus Membranaceus • Auricula’nın Venleri • Venleri (Zar Labirent) • Auricula’nın Lenfatikleri • Sinirleri • Ductus Semicirculares • Utriculus Meatus Acusticus Tuba Auditiva (Östaki • Sacculus Externus (Dış Kulak Yolu) Borusu) • Ductulus Cochlearis • Meatus Acusticus Externus Ossicula Auditus (Kulak • Organum Spirale (Corti Organı) Arterleri Kemikçikleri) • Membrana Tektoria • Meatus Acusticus Externus • Malleus • Incus • Stapes İç Kulak Sıvıları Venleri Musculi Ossiculorum Meatus Acusticus İnternus • Meatus Acusticus Externus Auditorium (Auris (İç Kulak Yolu) Duyu Sinirleri Media’nın Kasları) Auris İnterna’nın Damarları • Meatus Acusticus Externus Auris Media’nın Arterleri • Arterleri • Venleri Lenfatikleri Auris Media’nın Venleri Auris İnterna Sinirleri Auris Media’nın Sinirleri İşitme Siniri ve İşitme Yolları & İşitme Nedir ve Nasıl Gerçekleşir? Kulak Hastalıkları Buşon Hastalığı İşitme ve Sinir Sistemi • Afferent Sistem Timpanik Membran Perforasyonu Hastalığı • Efferent -

Effectiveness of Ear Molding in the Treatment of Congenital Auricular Deformity
CHINA CLINIcaL STUDIES IV ORIGINAL ARTICLE Effectiveness Of Ear Molding In the Treatment Of Congenital Auricular Deformity Corresponding authors: CHEN Peiwei 1 LI Jie 2 ZHAO Abstract Objective: To evaluate the short-term efficacy of ear molding in the treatment of congenital Shouqin 1 YANG Jingsong 1 DOU auricular deformity. Jingmin 1 WEI Chenyi 1 Methods: 24 infants (28 ears) were treated with ear molding device (EarWell Infant Ear Correction System). Doctors and parents were surveyed 1 month after treatment. Results: All cases were treated successfully without severe complications. 25 ears (89%) and 26 ears (92%) were rated as very satisfied or satisfied by doctors and parents, respectively. Conclusion: Ear molding is a noninvasive treatment, and effectively corrects congenital auricular deformity. Key words: Ear Disease; Deformity; Retrospective Study; Ear Molding. INFORMATION Exclusion Criteria Auricular deformities are classified into structural malformation and Age over 3 months; premature delivery; weight less than 2.5 kg; morphological malformation [1]. The former usually refers to the hypo- pathological jaundice, pneumonia and other systemic diseases. plasia of the auricle caused by the coloboma of skin and cartilage. The latter is the abnormal morphology of the well-developed auricle, which Overall 24 sick children (28 ears) were recruited for this treatment, could cause negative effects to the psychological development and so- including 14 males, 10 females, 16 right ears and 12 left ears. The age cial activities of children. Unlike structural malformations, such as mi- range for the recruited patients is 17-77 days, with a median age of 40.5 crotia, which must be corrected by auricle reconstruction, the auricle days. -

Congenital and Acquired Ear Deformities; Treatment Modalities
Congenital and acquired ear deformities; treatment modalities Marieke Petra van Wijk Author: M.P. van Wijk Cover: Ilse Modder, www.ilsemodder.nl Lay-out: Ilse Modder, www.ilsemodder.nl Print by: Gildeprint – Enschede, www.gildeprint.nl ISBN: 978-94-6323-565-5 © M.P. van Wijk, Utrecht, the Netherlands, 2019. All rights reserved. No part of this thesis may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording or any information storage or retrieval system, without prior permission of the author. Congenital and acquired ear deformities; treatment modalities Aangeboren en verworven oorschelpafwijkingen; behandelwijzen (met een samenvatting in het Nederlands) Proefschrift ter verkrijging van de graad van doctor aan de Universiteit Utrecht op gezag van de rector magnificus, prof.dr. H.R.B.M. Kummeling, ingevolge het besluit van het college voor promoties in het openbaar te verdedigen op dinsdag 23 april 2019 des middags te 2.30 uur door Marieke Petra van Wijk geboren op zaterdag 15 mei 1976 te Groningen promotor: Prof. dr. M. Kon copromotor: Dr. C. C. Breugem Paranimfen: Mw. Dr. E.M.L Corten Mw. Dr. A.L van Rijssen Leescommissie: Prof. Dr. J.J.M. van Delden Prof. Dr. R.L.A.W Bleys Prof. Dr. C.M.A.M. van der Horst Prof. Dr. R.J. Stokroos Prof. Dr. E.E.S. Nieuwenhuis TABLE OF CONTENTS Chapter 1. 11 Introduction and aim of the thesis Chapter 2. 29 Non-surgical correction of congenital deformities of the auricle: a systematic review of the literature. van Wijk MP, Breugem CC, Kon M. -

Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design
biomimetics Article Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design Pratap Sriram Sundar 1, Chandan Chowdhury 2 and Sagar Kamarthi 3,* 1 Indian School of Business, Mohali 160062, India; [email protected] 2 Indian School of Business, Gachibowli, Hyderabad 500111, India; [email protected] 3 Department of Mechanical and Industrial Engineering, Northeastern University, Boston, MA 02115, USA * Correspondence: [email protected]; Tel.: +1-617-373-3070 Abstract: The design of the human ear is one of nature’s engineering marvels. This paper examines the merit of ear design using axiomatic design principles. The ear is the organ of both hearing and balance. A sensitive ear can hear frequencies ranging from 20 Hz to 20,000 Hz. The vestibular apparatus of the inner ear is responsible for the static and dynamic equilibrium of the human body. The ear is divided into the outer ear, middle ear, and inner ear, which play their respective functional roles in transforming sound energy into nerve impulses interpreted in the brain. The human ear has many modules, such as the pinna, auditory canal, eardrum, ossicles, eustachian tube, cochlea, semicircular canals, cochlear nerve, and vestibular nerve. Each of these modules has several subparts. This paper tabulates and maps the functional requirements (FRs) of these modules onto design parameters (DPs) that nature has already chosen. The “independence axiom” of the axiomatic design methodology is applied to analyze couplings and to evaluate if human ear design is a good design (i.e., uncoupled design) or a bad design (i.e., coupled design). The analysis revealed that the human ear is a perfect design because it is an uncoupled structure. -

Tympanic Membrane (Membrana Tympanica, Myrinx)
Auditory and vestibular system Auris, is = Us, oton Auditory and vestibular system • external ear (auris externa) • middle ear (auris media) • internal ear (auris interna) = organum vestibulo- cochleare External ear (Auris externa) • auricle (auricula, pinna) – elastic cartilage • external acoustic meatus (meatus acusticus externus) • tympanic membrane (membrana tympanica, myrinx) • helix Auricle – crus, spina, cauda – (tuberculum auriculare Darwini, apex auriculae) • antihelix – crura, fossa triangularis • scapha • concha auriculae – cymba, cavitas • tragus • antitragus • incisura intertragica • lobulus auriculae posterior surface = negative image of the anterior one ligaments: lig. auriculare ant., sup., post. muscles – innervation: n. facialis • extrinsic muscles = facial muscles – mm. auriculares (ant., sup., post.) – m. temporoparietalis • intrinsic muscles: rudimentary – m. tragicus + antitragicus – m. helicis major+minor – m. obliquus + transversus auriculae, m. pyramidalis auriculae cartilage: cartilago auriculae - elastic skin: dorsally more loosen, ventrally firmly fixed to perichondrium - othematoma Auricle – supply • arteries: a. temporalis superficialis → rr. auriculares ant. a. carotis externa → a. auricularis post. • veins: v. jugularis ext. • lymph: nn.ll. parotidei, mastoidei • nerves: sensory – nn. auriculares ant. from n. auriculotemporalis (ventrocranial 2/3) – r. auricularis n. X. (concha) – n. occipitalis minor (dosrocranial) – n. auricularis magnus (cudal) motor: n. VII. External acoustic meatus (meatus acusticus -
Analysis in Otoplasty
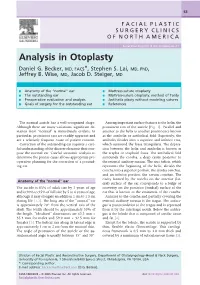
63 FACIAL PLASTIC SURGERY CLINICS OF NORTH AMERICA Facial Plast Surg Clin N Am 14 (2006) 63–71 Analysis in Otoplasty Daniel G. Becker, MD, FACS*, Stephen S. Lai, MD, PhD, Jeffrey B. Wise, MD, Jacob D. Steiger, MD & Anatomy of the “normal” ear & Mattress-suture otoplasty & The outstanding ear & Mattress-suture otoplasty: method of Tardy & Preoperative evaluation and analysis & Antihelix plasty without modeling sutures & Goals of surgery for the outstanding ear & References The normal auricle has a well-recognized shape. Among important surface features is the helix, the Although there are many variations, significant de- prominent rim of the auricle [Fig. 1]. Parallel and viation from ‘‘normal’’ is immediately evident. In anterior to the helix is another prominence known particular, prominent ears are readily apparent and as the antihelix or antihelical fold. Superiorly, the are a relatively frequent cause of patient concern. antihelix divides into a superior and inferior crus, Correction of the outstanding ear requires a care- which surround the fossa triangularis. The depres- ful understanding of the discrete elements that com- sion between the helix and antihelix is known as pose the normal ear. Careful anatomic analysis to the scapha or scaphoid fossa. The antihelical fold determine the precise cause allows appropriate pre- surrounds the concha, a deep cavity posterior to operative planning for the correction of a protrud- the external auditory meatus. The crus helicis, which ing ear. represents the beginning of the helix, divides the concha into a superior portion, the cymba conchae, and an inferior portion, the cavum conchae. The cavity formed by the concha on the anterior (lat- Anatomy of the “normal” ear eral) surface of the ear corresponds to a bulge or The auricle is 85% of adult size by 3 years of age convexity on the posterior (medial) surface of the and is 90% to 95% of full size by 5 to 6 years of age, ear that is known as the eminentia of the concha. -

Sundfeld-Reis Suture for the Correction of Auricular Axis and Ear
IDEAS AND INNOVATSundfeld-Reis IsutureONS for the correction of auricularVendraminFranco axis T FSandet al.et ear al. upper pole using otoplasty: preliminary note Sundfeld-Reis suture for the correction of auricular axis and ear upper pole using otoplasty: preliminary note Descrição do ponto de Sundfeld-Reis para correção do eixo auricular e polo superior da orelha em otoplastia: nota prévia DANIEL SUNDFELD SPIGA REAL1 ABSTRACT ROdrIGO PACHECO REIS2 Prominent ears are among the most frequent anomalies that affect the head and neck regions MÁRIO GUILHErmE CESCA and present with conchal disproportionality and/or the lack of an antihelix curvature. A ROCHA3 wide spectrum of techniques for the correction of these deformities has been published; the LYDIA MASAKO FErrEIRA4 most commonly cited are the techniques from Pitanguy, Converse, Stenvers, Stenstroem, Mustardé, Furnas, and Horlock. All of these techniques seek to restore facial harmony with proportional scaling of the pinna, a suitable cephaloauricular angle, and natural curvature of the antihelix. After reviewing the literature, the present study aims to describe a new technique for correcting the auricular axis and ear upper pole with a suture in the portion of the helical crus known as the Sundfeld-Reis technique. According to Adamson et al., this technique provides better positioning of the ear’s upper pole in relation to the tempo- ral pole without the need for suturing the triangular fossa region in the periosteum of the temporal bone. Therefore, using the Sundfeld-Reis technique, the pinna is placed parallel to the nasal dorsum, providing a natural result after otoplasty. The proposed technique is the latest possibility in the world of otoplasty that attains more natural results with fewer surgical interventions. -

Tutortube: Ear Anatomy and Physiology
TutorTube: Ear Anatomy and Physiology Fall 2020 Introduction Hello and welcome to TutorTube, where The Learning Center’s Lead Tutors help you understand challenging course concepts with easy to understand videos. My name is Grace Lead Tutor for Audiology and Speech-Language Pathology In today’s video, we will explore Ear Anatomy and Physiology. Let’s get started! Auditory Pathways The peripheral auditory pathway consists of the outer, middle and inner ear as well as the 8th cranial nerve. The 8th cranial nerve, called the vestibulocochlear nerve, is responsible for maintaining body balance and hearing. The central auditory pathway consists of the brainstem and brain. Sections You can see the three basic sections of the ear in figure 1. We have the outer ear that includes the pinna and the external auditory meatus. The middle ear that consists of the tympanic membrane, ossicles, and eustachian tube. The inner ear consists of cochlea, vestibule, and semicircular canals. Let’s look into these sections further. Figure 1 (“Anatomy of the Ear”) Contact Us – Sage Hall 170 – (940) 369-7006 [email protected] - @UNTLearningCenter 2 Outer Ear The pinna (AKA the auricle) is made up of cartilage, collects sound, and helps localize sound. We can see an example of the pinna in figure 2. Let’s go through and label parts of the pinna. Here we have the helix, scapha, antihelical fold, antihelix, antitragus, lobule, tragus, entrance to external auditory meatus, concha, and fossa. The external auditory meatus (or ear canal) connects the outer ear to the middle ear and funnels the sound to the eardrum. -
Plastic Surgery of the Ear
Volume 11 • Issue R3 PLASTIC SURGERY OF THE EAR Richard Y. Ha, MD Matthew J. Trovato, MD Reconstructive OUR EDUCATIONAL PARTNERS Selected Readings in Plastic Surgery appreciates the generous support provided by our educational partners. facial aesthetics OUR EDUCATIONAL PARTNERS www.SRPS.org Selected Readings in Plastic Surgery appreciates the generous support provided by our educational partners. Editor-in-Chief Jerey M. Kenkel, MD Editor Emeritus F. E. Barton, Jr, MD Contributing Editors R. S. Ambay, MD 30 Topics R. G. Anderson, MD S. J. Beran, MD Grafts and Flaps S. M. Bidic, MD Wound Healing, Scars, and Burns G. Broughton II, MD, PhD J. L. Burns, MD Skin Tumors: Basal Cell Carcinoma, Squamous Cell J. J. Cheng, MD Carcinoma, and Melanoma C. P. Clark III, MD Implantation and Local Anesthetics D. L. Gonyon, Jr, MD Head and Neck Tumors and Reconstruction A. A. Gosman, MD Microsurgery and Lower Extremity Reconstruction K. A. Gutowski, MD Nasal and Eyelid Reconstruction J. R. Grin, MD Lip, Cheek, and Scalp Reconstruction R. Y. Ha, MD Ear Reconstruction and Otoplasty F. Hackney, MD, DDS Facial Fractures L. H. Hollier, MD Blepharoplasty and Brow Lift R. E. Hoxworth, MD Rhinoplasty J. E. Janis, MD Rhytidectomy R. K. Khosla, MD Injectables J. E. Leedy, MD Lasers J. A. Lemmon, MD Facial Nerve Disorders A. H. Lipschitz, MD Cleft Lip and Palate and Velopharyngeal Insuciency R. A. Meade, MD Craniofacial I: Cephalometrics and Orthognathic Surgery D. L. Mount, MD Craniofacial II: Syndromes and Surgery J. C. O’Brien, MD Vascular Anomalies J. K. Potter, MD, DDS Breast Augmentation R.