Color in Healthcare Environments - a Research Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

COLOR SPACE MODELS for VIDEO and CHROMA SUBSAMPLING
COLOR SPACE MODELS for VIDEO and CHROMA SUBSAMPLING Color space A color model is an abstract mathematical model describing the way colors can be represented as tuples of numbers, typically as three or four values or color components (e.g. RGB and CMYK are color models). However, a color model with no associated mapping function to an absolute color space is a more or less arbitrary color system with little connection to the requirements of any given application. Adding a certain mapping function between the color model and a certain reference color space results in a definite "footprint" within the reference color space. This "footprint" is known as a gamut, and, in combination with the color model, defines a new color space. For example, Adobe RGB and sRGB are two different absolute color spaces, both based on the RGB model. In the most generic sense of the definition above, color spaces can be defined without the use of a color model. These spaces, such as Pantone, are in effect a given set of names or numbers which are defined by the existence of a corresponding set of physical color swatches. This article focuses on the mathematical model concept. Understanding the concept Most people have heard that a wide range of colors can be created by the primary colors red, blue, and yellow, if working with paints. Those colors then define a color space. We can specify the amount of red color as the X axis, the amount of blue as the Y axis, and the amount of yellow as the Z axis, giving us a three-dimensional space, wherein every possible color has a unique position. -

Tabla De Conversión Pantone a NCS (Natural Color System)
Tabla de conversión Pantone a NCS (Natural Color System) PANTONE NCS (más parecido) PANTONE NCS (más parecido) Pantone Yellow C NCS 0580-Y Pantone 3985C NCS 3060-G80Y Pantone Yellow U NCS 0580-Y Pantone 3985U NCS 4040-G80Y Pantone Warm Red C NCS 0580-Y70R Pantone 3995C NCS 5040-G80Y Pantone Warm Red U NCS 0580-Y70R Pantone 3995U NCS 6020-G70Y Pantone Rubine Red C NCS 1575-R10B Pantone 400C NCS 2005-Y50R Pantone Rubine Red U NCS 1070-R20B Pantone 400U NCS 2502-R Pantone Rhodamine Red C Pantone 401C NCS 2005-Y50R Pantone Rhodamine Red U NCS 1070-R20B Pantone 401U NCS 2502-R Pantone Purple C Pantone 402C NCS 4005-Y50R Pantone Purple U NCS 2060-R40B Pantone 402U NCS 3502-R Pantone Violet C Pantone 403C NCS 4055-Y50R Pantone Violet U NCS 3050-R60B Pantone 403U NCS 4502-R Pantone Reflex Blue C NCS 3560-R80B Pantone 404C NCS 6005-Y20R Pantone Reflex Blue U NCS 3060-R70B Pantone 404U NCS 5502-R Pantone Process Blue C NCS 2065-B Pantone 405C NCS 7005-Y20R Pantone Process Blue U NCS 1565-B Pantone 405U NCS 6502-R Pantone Green C NCS 2060-B90G Pantone 406C NCS 2005-Y50R Pantone Green U NCS 2060-B90G Pantone 406U NCS 2005-Y50R Pantone Black C NCS 8005-Y20R Pantone 407C NCS 3005-Y50R Pantone Black U NCS 7502-Y Pantone 407U NCS 3005-Y80R Pantone Yellow 012C NCS 0580-Y Pantone 408C NCS 3005-Y50R Pantone Yellow 012U NCS 0580-Y Pantone 408U NCS 4005-Y80R Pantone Orange 021C NCS 0585-Y60R Pantone 409C NCS 5005-Y50R Pantone Orange 021U NCS 0580-Y60R Pantone 409U NCS 5005-Y80R Pantone Red 032C NCS 0580-Y90R Pantone 410C NCS 5005-Y50R Pantone Red 032U NCS -
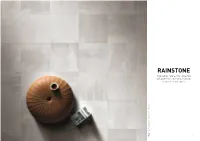
RAINSTONE Inspired by Nature, This Collection Will Give Fresh and Natural Design Elements to Any Space
RAINSTONE Inspired by nature, this collection will give fresh and natural design elements to any space. Rain Stone Dark Grey 60x60 cm | 24”x 24” Dark Grey Rain Stone 12 13 Floor Floor Floor Rain Stone_Natural 60x60 | 24”x24” 14 15 RAIN STONE NATURAL RAIN STONE BEIGE WHITE *CERST060002_NATURAL 60x120 - 24”x48” rect. CERST060006_NATURAL 60x60 - 24”x24” rect. *CERST060001_BEIGE WHITE 60x120 - 24”x48” rect. CERST060005_BEIGE WHITE 60x60 - 24”x24” rect. *CERST030014 _NATURAL 30x120 - 12”x48” rect. CERST030002_NATURAL 30x60 - 12”x24” rect. *CERST030013 _BEIGE WHITE 30x120 - 12”x48” rect. CERST030001_BEIGE WHITE 30x60 - 12”x24” rect. *CERST029002_NATURAL 29x29 - 12”x12” rect. CERST005002_NATURAL MOSAICO *CERST029001_BEIGE WHITE 29x29 - 12”x12” rect. CERST005001_BEIGE WHITE MOSAICO 5x5 - 2”x2” rect. 5x5 - 2”x2” rect. *CERST015002_NATURAL 15x60 - 6”x24” rect. *CERST010002_NATURAL 10x30 - 4”x12” rect. *CERST015001_BEIGE WHITE 15x60 - 6”x24” rect. *CERST010001_BEIGE WHITE 10x30 - 4”x12” rect. *CERST030006_NATURAL *CERST030010_NATURAL WALL *CERST030005_BEIGE WHITE *CERST030009_ BEIGE WHITE WALL 5x15 - 2”x6” rect. 30x60 - 12”x24” rect. 5x15 - 2”x6” rect. 30x60 - 12”x24” rect. 30x30 - 12”x12” su rete rect. 30x30 - 12”x12” su rete rect. *CERST031002 _ NATURAL CHEVRON *CERST028002 _ NATURAL FRINGE *CERST031001_ BEIGE WHITE CHEVRON *CERST028001_ BEIGE WHITE FRINGE 31,5x29,6 - 12,40”x11,65” rect. 28,8X28,8 - 11,34”x11,34” rect. 31,5x29,6 - 12,40”x11,65” rect. 28,8X28,8 - 11,34”x11,34” rect. 16 * Special order sizes 17 RAIN STONE LIGHT GREY RAIN STONE DARK GREY *CERST060003_LIGHT GREY 60x120 - 24”x48” rect. CERST060007_LIGHT GREY 60x60 - 24”x24” rect. *CERST060004_DARK GREY 60x120 - 24”x48” rect. CERST060008_DARK GREY 60x60 - 24”x24” rect. -

What's That Smell-Journal
Southern Journal of Philosophy (2009) VLVII: 321-348. What’s That Smell? Clare Batty University of Kentucky In philosophical discussions of the secondary qualities, color has taken center stage. Smells, tastes, sounds, and feels have been treated, by and large, as mere accessories to colors. We are, as it is said, visual creatures. This, at least, has been the working assumption in the philosophy of perception and in those metaphysical discussions about the nature of the secondary qualities. The result has been a scarcity of work on the “other” secondary qualities. In this paper, I take smells and place them front and center. I ask: What are smells? For many philosophers, the view that colors can be explained in purely physicalistic terms has seemed very appealing. In the case of smells, this kind of nonrelational view has seemed much less appealing. Philosophers have been drawn to versions of relationalism—the view that the nature of smells must be explained (at least in part) in terms of the effects they have on perceivers. In this paper, I consider a contemporary argument for this view. I argue that nonrelationalist views of smell have little to fear from this argument. It was the first time Grenouille had ever been in a perfumery, a place in which odors are not accessories but stand unabashedly at the center of interest…. He knew every single odor handled here and had often merged them in his innermost thoughts to create the most splendid perfumes. - Patrick Süskind, Perfume In philosophical discussions of the secondary qualities, color has taken center stage. -

Colour Vision, Philosophical Issues About
Encyclopedia of Cognitive Science 173 ENCYCLOPEDIA OF COGNITIVE SCIENCE 2000 ©Macmillan Reference Ltd Colour Vision, Philosophical Issues About Colour#Vision Byrne, Alex Alex Byrne MIT, Massachusetts, USA Hilbert, David R. David R. Hilbert University of Illinois at Chicago, Illinois, USA The primary issues concern whether objects have colours, and what sorts of properties the colours are. Some philosophers hold that nothing is coloured, others that colour are powers to affect perceivers, and others that colours are physical properties. 1. Introduction According to our everyday experience, many things are coloured. Roses are red and violets are blue. On the other hand, according to physical science, roses and violets are composed of colourless particles (or at any rate, if not particles, something equally colourless). These two pictures of the world do not seem to be obviously compatible, and indeed many have found them to be plainly incompatible. Galileo, for example, thought that physical science had shown that objects are not really coloured, but instead are "in the mind". Philosophical theories of colour since the scientific revolution have attempted either to reconcile the two pictures, or else to explain why one of them should be rejected. Until recently, philosophers drew most of their data about colour and colour perception from their own experience of colour. Although personal experience is a valuable source, in fact a good deal of information relevant to abstract philosophical questions about colour and the world as revealed by science is to be found in the work of colour scientists. Many contemporary philosophers take the physical, biological, Encyclopedia of Cognitive Science and behavioural sciences to place serious constraints on philosophical theories of colour. -

Color Primitivism
Springer http://www.jstor.org/stable/27667884 . Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Springer is collaborating with JSTOR to digitize, preserve and extend access to Erkenntnis (1975-). http://www.jstor.org This content downloaded on Mon, 18 Feb 2013 11:37:53 AM All use subject to JSTOR Terms and Conditions Erkenntnis (2007) 66:73-105 ? Springer 2007 DOI 10.1007/s 10670-006-9028-8 ALEX BYRNE and DAVID R. HILBERT COLOR PRIMITIVISM ABSTRACT. The typical kind of color realism is reductive: the color properties are identified with properties specified in other terms (as ways of altering light, for ? instance). If no reductive analysis is available if the colors are primitive sui generis - properties this is often taken to be a convincing argument for eliminativism. That is, realist primitivism is usually thought to be untenable. The realist preference for over reductive theories of color the last few decades is particularly striking in light of the generally anti-reductionist mood of recent philosophy of mind. The parallels case are between the mind-body problem and the of color substantial enough that the difference in trajectory is surprising. -

Cromie Is Designed Around the Natural Color System (NCS), a Color Notation System That Classifies Color According to the Way the Human Eye Perceives It
NCS SYSTEM Cromie is designed around the Natural Color System (NCS), a color notation system that classifies color according to the way the human eye perceives it. Unlike arbitrary numeric systems, NCS is capable of identifying and accurately notating any of the 10 million colors the eye can perceive. Relying on the six elementary colors (White, Black, Yellow, Red, Blue, Green), the NCS notation classifies a color in relation to each of the six elementary colors. NCS NOTATION Let’s take the NCS notation S 1050-Y90R as an example. The letter S before the complete notation indicates that the color is part of the NCS Second Edition. The number 1050 indicates the shade (i.e. the amount of blackness (S) and the chromaticity (C)). In this case, the blackness, or darkness (S), is 10% and the chromaticity (C) is 50%. Y90R indicates the similarity to the other two elementary colors, Y (yellow) and R (red). Y90R indicates yellow with 90% of red. Neutral gray tints have no shade (chromaticity equals 0) and are notated by the nuance followed by -N, as it is neutral color. 0300-N is white, followed by 0500-N, 1000-N, 1500 N, etc. up to 9000-N, which is black. NCS COLOR SPACE In this 3D model, all imaginable surface colours can be given a specific classification and an exact NCS notation. S 1050 - Y90 NCS COLOR CIRCLE The NCS color circle is a horizontal section that cuts the 3D model in two. In this circle, the four elementary colors are placed at the cardinal points and the space between two colors is divided into 10 parts. -
Color Appearance Models Second Edition
Color Appearance Models Second Edition Mark D. Fairchild Munsell Color Science Laboratory Rochester Institute of Technology, USA Color Appearance Models Wiley–IS&T Series in Imaging Science and Technology Series Editor: Michael A. Kriss Formerly of the Eastman Kodak Research Laboratories and the University of Rochester The Reproduction of Colour (6th Edition) R. W. G. Hunt Color Appearance Models (2nd Edition) Mark D. Fairchild Published in Association with the Society for Imaging Science and Technology Color Appearance Models Second Edition Mark D. Fairchild Munsell Color Science Laboratory Rochester Institute of Technology, USA Copyright © 2005 John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England Telephone (+44) 1243 779777 This book was previously publisher by Pearson Education, Inc Email (for orders and customer service enquiries): [email protected] Visit our Home Page on www.wileyeurope.com or www.wiley.com All Rights Reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning or otherwise, except under the terms of the Copyright, Designs and Patents Act 1988 or under the terms of a licence issued by the Copyright Licensing Agency Ltd, 90 Tottenham Court Road, London W1T 4LP, UK, without the permission in writing of the Publisher. Requests to the Publisher should be addressed to the Permissions Department, John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England, or emailed to [email protected], or faxed to (+44) 1243 770571. This publication is designed to offer Authors the opportunity to publish accurate and authoritative information in regard to the subject matter covered. -
What Color Is the Interdisciplinary?
ISSUES IN INTERDISCIPLINARY STUDIES Vol. 36(1), pp. 14-33 (2018) What Color Is the Interdisciplinary? by Brian McCormack Principal Lecturer, College of Integrative Sciences and Arts Arizona State University Abstract: Color has been considered as a special problem in several disciplines, notably art and music, but also philosophy and literature. Given that color is also a central feature of some scientific thought (think of Newton and the color spectrum, for example), the question “What color is the interdisciplinary?” seems to be a golden opportunity to investigate the interdisciplinarity of color. My question, which follows from Michael Taussig’s similar anthropological question, “What color is the sacred?” points to important issues about the nature of interdisciplinary thinking. Rather than merely posit an answer such as, for example, “interdisciplinarity is red,” we would do well to think through those issues. The question is novel not only because it invents the nominal adjectival form of “interdisciplinarity” as “the interdisciplinary” (as in “the sacred”), but also because it approaches interdisciplinarity with a hint of both reverence and irreverence. Giorgio Agamben’s take on “the sacred” and Walter Benjamin’s understanding of color figure into my response to the question. Agamben explains the importance of the “profanation” of the apparatuses of “the sacred.” And Benjamin’s ideas about the color of experience establish the basis of an answer to our question: the rainbow. Keywords: color, the sacred, the interdisciplinary, apparatus, profanation, Taussig, Agamben, Benjamin, the rainbow Introduction “What color is the interdisciplinary?” An odd question perhaps, but it enables two things to happen. First, the nominal form of the adjective “interdisciplinary,” normally understood to be “interdisciplinarity,” here becomes “the interdisciplinary” (a nominal adjective when used to describe a noun, and an adjectival noun when standing alone). -
Major Color Order Systems and Their Psychophysical Structure
Chapter 7 Major Color Order Systems and Their Psychophysical Structure In this chapter only the Munsell, OSA-UCS, and Swedish NCS systems will be discussed. The former two are the most important attempts to create psy- chologically uniform systems, the latter uses the presumed natural approach of Hering (see Chapter 2) to create a color order system, having a regular structure, but not one uniform in terms of size of perceived differences. There are several other newer color order systems extant, but they neither make claims for uniformity nor for regularity according to new, significant psycho- logical attributes. The issue of viewing conditions for these systems has been attended to in different ways.As discussed previously,the Munsell system is illustrated as if the chips at each value level would be viewed against an achromatic surround of the same value.Chips of two adjacent value levels are illustrated as if viewed against an achromatic surround of intermediate value. The actual atlas displays the chips on white paper (historically of various degrees of whiteness), thus result- ing in distortions of the value scale, particularly at lower values.The OSA-UCS system is defined for an achromatic surround of luminous reflectance Y = 30 (L = 0).The atlas samples are in transparent jackets.NCS,finally,has been estab- lished against an immediate achromatic surround of Y = 78 in a light booth painted with an achromatic gray of Y = 54.The atlas displays samples on white paper. Both latter systems only result in the intended color experiences when viewed against the appropriate surrounds. Munsell and NCS are defined for Color Space and Its Divisions: Color Order from Antiquity to the Present, by Rolf G. -

Tfl Basic Elements Standard
Transport for London Transport for London Basic elements standard Issue 3 MAYOR OF LONDON Transport for London Contents Foreword 1 Glossary 1.1 Colour glossary 1.2 Corporate typeface 2 Transport for London 2.1 Roundel usage 2.2 Roundel usage continued 2.3 Exclusion zones 2.4 Colours 3 Secondary identities For further information Foreword Contents A well designed, confident and consistent visual identity is highly effective in communicating the strengths of our organisation. It is essential that Transport for London (TfL) maintains a high standard for co-ordinated design in every aspect of our operations. This document gives guidance on the basic elements that make up the TfL visual identity. The information covers the corporate typeface, the visual identity and the corporate colours. For more guidance on TfL Corporate standards, please visit the TfL website: tfl.gov.uk/corporatedesign 1 Glossary Contents The main terms used in these guidelines are Symbol Logotype as follows: Other visual identifiers used by TfL. The text of TfL set in New Johnston Medium upper and lower case type. Logotypes are Mark used with roundels or symbols in a fixed A combination of a roundel or symbol relationship to form Marks, but can also be with a logotype in a fixed relationship as used in a looser relationship such as that used shown below. on stationery (see the Stationery standards). Exclusion zone The minimum area around marks, roundels or Transport for London symbols that must be kept free of other graphic elements. This is to ensure that they are reproduced clearly and legibly without Roundel interference from other visual devices. -
Form Without Matter Empedocles and Aristotle on Color Perception
Form without Matter Empedocles and Aristotle on Color Perception Mark Eli Kalderon 2 i Ineluctable modality of the visible: at least that if no more, thought through my eyes. Signatures of all things I am here to read, seaspawn and seawrack, the nearing tide, that rusty boot. Snotgreen, bluesilver, rust: coloured signs. Limits of the diaphane. But he adds: in bodies. Then he was aware of them bodies before of them coloured. How? By knocking his sconce against them, sure. Go easy. Bald he was and a millionaire, maestro di color che sanno. Limit of the diaphane in. Why in? Diaphane, adiaphane. If you can put your five fingers through it, it is a gate, if not a door. Shut your eyes and see. James Joyce, Ulysses “Quand nos yeux se touchent, fait-il jour ou fait-il nuit?” Jacques Derrida, Le toucher, Jean-Luc Nancy ii Contents 1 Empedocles 1 1.1 Dialectic .................................... 1 1.2 The Answer in the Style of Gorgias .................... 4 1.3 Empedocles’ Theory of Vision ....................... 7 1.4 Empedoclean Puzzlement .......................... 12 1.5 Definition ................................... 15 2 Perception at a Distance 17 2.1 The Sensible Qualities of Remote External Particulars ........ 19 2.1.1 External ................................ 20 2.1.2 Particular ............................... 26 2.1.3 Remote ................................ 30 2.2 Against the Empedoclean Principle .................... 31 2.3 The Generalized Form of Empedoclean Puzzlement .......... 39 3 Transparency 41 3.1 Motive and Method ............................. 41 3.2 Transparency in De Anima .......................... 42 3.3 Transparency in De Sensu ........................... 54 4 Color 65 4.1 Aristotle’s Explanatory Strategy .....................