Introduction to Ebola Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Factor That Should Raise Awareness in the Practice of Pediatric Medicine: West Nile Virus
Case Report / Olgu Sunumu DOI: 10.5578/ced.201813 • J Pediatr Inf 2018; 12(2): e70-e72 A Factor That Should Raise Awareness in the Practice of Pediatric Medicine: West Nile Virus Çocuk Hekimliği Pratiğinde Farkındalığın Artması Gereken Bir Etken; Batı Nil Virüsü Duygu Uç1, Tamer Çelik1, Derya Gönen1, Asena Sucu1, Can Celiloğlu1, Orkun Tolunay1, Ümit Çelik1 1 Clinics of Pediatrics, Adana City Training and Research Hospital, Adana, Turkey Abstract Özet West Nile virus is an RNA virus found in Flaviviridae family and its vector Batı Nil virüsü Flaviviridae ailesinde yer alan bir RNA virüsü olup, vektörü is of Culex-type mosquitoes and the population of these flies soar dra- Culex türü sivrisineklerdir. Culex türü sineklerin popülasyonu Ağustos matically in August. Most of the infected people who have mild viremia ayında pik yapmaktadır. Ilımlı viremiye sahip enfekte bireylerin çoğu experience this disease asymptomatically or encounter situations simi- hastalığı asemptomatik geçirmekte ya da diğer viral enfeksiyonlara ben- lar to other viral infections. Patients suffer from fatigue, fever, and head- zeyen tablolarla karşımıza gelmektedir. Hastalarda sıklıkla halsizlik, ateş, ache, pain in the eyes, myalgia, diarrhea, vomiting, arthralgia, rash and baş ağrısı, gözlerde ağrı, miyalji, ishal, kusma, artralji, döküntü ve lenfa- lymphadenopathy. Similar to many diseases transmitted through mos- denopati görülebilmektedir. Sivrisinekler aracılığı ile bulaşan birçok has- quitoes, the West Nile virus should also be considered as a problem of talık -

Signature Redacted Signature of Author
Developing VHH-based tools to study Ebolavirus Infection By Jason V. M. H. Nguyen B.S., Biochemistry and Molecular Biology University of California, Santa Cruz, 2012 Submitted to the Microbiology Graduate Program in partial fulfillment of the requirements for the degree of Doctor of Philosophy At the Massachusetts Institute of Technology June 2019 2019 Massachusetts Institute of Technology. All rights reserved. Signature redacted Signature of Author...... .................................................................... V Y' Jason V. M. H. Nguyen Microbiology Graduate Program May 13, 2019 Signature redacted Certified by.............. ................................................................... Hidde L. Ploegh Senior Investigator Boston Children's Hospital It Signature redacted Accepted by....... ......................................................................... Jacquin C. Niles Associate Professor of Biological Engineering Chair of Microbiology Program MASSACHUSETTS INSTITUTE OF TECHNOLOGY JUN 2 12019 1 LIBRARIES ARCHIVES 2 Developing VHH-based tools to study Ebolavirus Infection By Jason V. M. H. Nguyen Submitted to the Microbiology Graduate Program on May 13th, 2019 in partial fulfillment of the requirements for the degree of Doctor of Philosophy ABSTRACT Variable domains of camelid-derived heavy chain-only antibodies, or VHHs, have emerged as a unique antigen binding moiety that holds promise in its versatility and utilization as a tool to study biological questions. This thesis focuses on two aspects on developing tools to study infectious disease, specifically Ebolavirus entry. In Chapter 1, I provide an overview about antibodies and how antibodies have transformed the biomedical field and how single domain antibody fragments, or VHHs, have entered this arena. I will also touch upon how VHHs have been used in various fields and certain aspects that remain underexplored. Chapter 2 focuses on the utilization of VHHs to study Ebolavirus entry using VHHs that were isolated from alpacas. -
Aids for Management of Common Headache Disorders in Primary Care
J Headache Pain (2007) 8:S1 DOI 10.1007/s10194-007-0366-y Lifting The Burden: The Global Campaign to Reduce the Burden of Headache Worldwide in collaboration with European Headache Federation Aids for management of common headache disorders in primary care This is a "Springer Open Choice" article. Unrestricted non-commercial use, distribution, and reproduction in any medium is permitted, provided the original author and source are credited. J Headache Pain (2007) 8:S2 PREFACE T.J. Steiner Aids for management of common headache P. Martelletti disorders in primary care T.J. Steiner Medical management of headache Whilst the focus of this publication Chairman: Global Campaign Committee disorders, for the vast majority of is Europe, these management aids Lifting The Burden people affected by them, can and have been developed to be useful should be carried out in primary cross-culturally and may suit a P. Martelletti care. It does not require specialist wider population. Editor-in-Chief Journal of Headache and Pain skills. Nonetheless, it is recognised The European principles of that non-specialists throughout management of common headache Europe may have received limited disorders in primary care are the training in the diagnosis and treat- essential core of these aids. These ment of headache. are set out in 12 sections, each one This special supplement of Journal more-or-less stand-alone. They are of Headache and Pain is the out- supplemented in Appendices 1 and put of a collaboration between the 2 by a measure of headache burden European Headache Federation (the HALT index), intended for (EHF) and Lifting The Burden: the pre-treatment assessment of illness Global Campaign to Reduce the severity, an outcome measure (the Burden of Headache Worldwide, a HART index), which is a guide to programme for the benefit of peo- follow-up and need for treatment- ple with headache conducted under review, and a series of patient the auspices of the World Health information leaflets developed to Organization. -

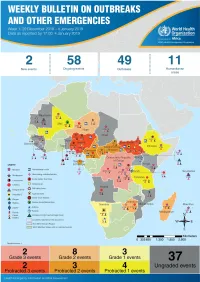
Dengue Fever in Senegal 6 - 7 Ongoing Events Ebola Virus Disease in the Democratic Republic of the Congo Humanitarian Crisis in Cameroon
Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme is currently monitoring 58 events in the region. This week’s edition covers key new and ongoing events, including: 2 Overview Hepatitis E in Central African Republic 3 - 5 New events Monkeypox in Central African Republic Dengue fever in Senegal 6 - 7 Ongoing events Ebola virus disease in the Democratic Republic of the Congo Humanitarian crisis in Cameroon. 8 Summary of major issues challenges and For each of these events, a brief description, followed by public health proposed actions measures implemented and an interpretation of the situation is provided. 9 All events currently A table is provided at the end of the bulletin with information on all new and being monitored ongoing public health events currently being monitored in the region, as well as events that have recently been closed. Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo has reached a critical juncture, marked by a precarious security situation, persistence of pockets of community resistance/ mistrust and expanding geographical spread of the disease. During the reporting week, there was an incident involving a response team performing burial activity in Butembo. This came barely days following a widespread community strike (“ville morte”) in Beni and several towns, and an earlier armed attack in Beni. These incidents severely disrupted most outbreak control interventions. Meanwhile, EVD cases have been confirmed in new areas with worse insecurity and in close proximity to the border with Uganda. -

National Guidelines for Clinical Management of Chikungunya 2016
CONTENTS Chapter Name of the Chapter Page No. 1 INTRODUCTION 1 2 Chikungunya: Status & disease burden 2-4 2.1 Transmission & trends 2 2.2 Global situation 2 2.3 Chikungunya in India (Past & present) 2-4 3 Laboratory diagnosis of Chikungunya f ever 5-7 3.1 Types of Laboratory tests available and specimens required: 5-6 3.2 Interpretation of results: 6 3.3 NVBDCP Laboratory Network: 6-7 3.4 Laboratory confirmation in case of Chikungunya outbreak 7 4 Case definition and differential diagnos is 8-9 4.1 Case definition 8 4.2 Differential diagnosis 8-9 5 Clinical manifestation of Chikungunya 10-16 5.1 Incubation period 10 5.2 Clinical Features: 10 5.3 Clinical Classification of severity of Chikungunya: 11 5.4 High Risk group: 11-12 5.5 Fever 12 5.6 Arthralgia 12 5.7 Back ache 12 5.8 Headache 13 5.9 Rash: 13 5.10 Stomatitis and oral ulcers : 13 5.11 Hyperpigmentation 13 5.12 Exfoliative dermatitis 13 5.13 Retrobulbar pain 13 5.14 Neurological manifestations 13 5.15 Occular manifestations 13 5.16 Chikungunya in Children 13-14 5.17 Impact of Chikungunya in Pregnancy & Neonates 14 5.17 Chikungunya in Elderly 14 5.18 Chikungunya Co infection with Dengue 14-15 5.19 Sequelae: 15 5.20 Mortality 15 5.21 Pathogenesis 16 6 Cl inical management of Chikungunya cases 17-20 6.1 Guiding principles of clinical management 17-18 6.2 Hospital based 18-19 6.3 Guiding principles for managing chronic pain 19 6.4 Summary 19-20 7 Public Health Measures 21-22 7.1 Minimizing transmissio n of infection: Annexure 1 Virus Genotype of Chikungunya virus 23-24 Vector Transmission Cycle References and Further study 25-26 Draft Chapter 1 INTRODUCTION Chikungunya fever is a viral disease transmitted to humans by the bite of infected Aedes aegypti mosquitoes. -

2019 Icar Program & Abstracts Book
Hosted by the International Society for Antiviral Research (ISAR) ND International Conference 32on Antiviral Research (ICAR) Baltimore MARYLAND PROGRAM and USA Hyatt Regency BALTIMORE ABSTRACTS May 12-15 2019 ND TABLE OF International Conference CONTENTS 32on Antiviral Research (ICAR) Daily Schedule . .3 Organization . 4 Contributors . 5 Keynotes & Networking . 6 Schedule at a Glance . 7 ISAR Awardees . 10 The 2019 Chu Family Foundation Scholarship Awardees . 15 Speaker Biographies . 17 Program Schedule . .25 Posters . 37 Abstracts . 53 Author Index . 130 PROGRAM and ABSTRACTS of the 32nd International Conference on Antiviral Research (ICAR) 2 ND DAILY International Conference SCHEDULE 32on Antiviral Research (ICAR) SUNDAY, MAY 12, 2019 › Women in Science Roundtable › Welcome and Keynote Lectures › Antonín Holý Memorial Award Lecture › Influenza Symposium › Opening Reception MONDAY, MAY 13, 2019 › Women in Science Award Lecture › Emerging Virus Symposium › Short Presentations 1 › Poster Session 1 › Retrovirus Symposium › ISAR Award of Excellence Presentation › PechaKucha Event with Introduction of First Time Attendees TUESDAY, MAY 14, 2019 › What’s New in Antiviral Research 1 › Short Presentations 2 & 3 › ISAR Award for Outstanding Contributions to the Society Presentation › Career Development Panel › William Prusoff Young Investigator Award Lecture › Medicinal Chemistry Symposium › Poster Session 2 › Networking Reception WEDNESDAY, MAY 15, 2019 › Gertrude Elion Memorial Award Lecture › What’s New in Antiviral Research 2 › Shotgun Oral -

To Ebola Reston
WHO/HSE/EPR/2009.2 WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 EPIDEMIC AND PANDEMIC ALERT AND RESPONSE WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 © World Health Organization 2009 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distin- guished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the policies of the World Health Organization. -

How Severe and Prevalent Are Ebola and Marburg Viruses?
Nyakarahuka et al. BMC Infectious Diseases (2016) 16:708 DOI 10.1186/s12879-016-2045-6 RESEARCHARTICLE Open Access How severe and prevalent are Ebola and Marburg viruses? A systematic review and meta-analysis of the case fatality rates and seroprevalence Luke Nyakarahuka1,2,5* , Clovice Kankya2, Randi Krontveit3, Benjamin Mayer4, Frank N. Mwiine2, Julius Lutwama5 and Eystein Skjerve1 Abstract Background: Ebola and Marburg virus diseases are said to occur at a low prevalence, but are very severe diseases with high lethalities. The fatality rates reported in different outbreaks ranged from 24–100%. In addition, sero-surveys conducted have shown different seropositivity for both Ebola and Marburg viruses. We aimed to use a meta-analysis approach to estimate the case fatality and seroprevalence rates of these filoviruses, providing vital information for epidemic response and preparedness in countries affected by these diseases. Methods: Published literature was retrieved through a search of databases. Articles were included if they reported number of deaths, cases, and seropositivity. We further cross-referenced with ministries of health, WHO and CDC databases. The effect size was proportion represented by case fatality rate (CFR) and seroprevalence. Analysis was done using the metaprop command in STATA. Results: The weighted average CFR of Ebola virus disease was estimated to be 65.0% [95% CI (54.0–76.0%), I2 = 97.98%] whereas that of Marburg virus disease was 53.8% (26.5–80.0%, I2 = 88.6%). The overall seroprevalence of Ebola virus was 8.0% (5.0%–11.0%, I2 = 98.7%), whereas that for Marburg virus was 1.2% (0.5–2.0%, I2 = 94.8%). -
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 14: 29 March to 4 April 2021 Data as reported by: 17:00; 4 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 116 103 13 New event Ongoing events Outbreaks Humanitarian crises 117 622 3 105 Algeria ¤ 36 13 110 0 5 420 164 Mauritania 7 2 10 501 392 110 0 7 0 Niger 17 927 449 Mali 3 334 10 567 0 6 0 2 079 4 4 595 165 Eritrea Cape Verde 38 520 1 037 Chad Senegal 4 918 185 59 0 Gambia 27 0 3 0 17 125 159 9 761 45 Guinea-Bissau 796 17 7 0 Burkina Faso 225 46 215 189 2 963 0 162 593 2 048 Guinea 12 817 150 12 38 397 1 3 662 66 1 1 23 12 Benin 30 0 Nigeria 1 873 71 0 Ethiopia 420 14 481 5 6 188 15 Sierra Leone Togo 3 473 296 53 920 779 52 14 Ghana 5 245 72 Côte d'Ivoire 10 098 108 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 25 0 19 670 120 43 180 237 90 287 740 Cameroon 7 0 28 676 137 5 330 13 138 988 2 224 1 952 87 655 2 51 22 43 0 112 12 6 1 488 6 3 988 79 11 187 6 902 102 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 042 85 41 016 335 Kenya Legend 7 100 90 Gabon Congo 18 504 301 Rwanda Humanitarian crisis 2 212 34 22 482 311 Measles 18 777 111 Democratic Republic of the Congo 9 681 135 Burundi 2 964 6 Monkeypox Ebola virus disease Seychelles 27 930 739 1 525 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 189 0 4 084 20 509 21 Cholera Yellow fever 1 349 5 6 257 229 22 631 542 cVDPV2 Dengue fever 88 930 1 220 Comoros Angola Malawi COVID-19 Chikungunya 33 661 1 123 862 0 3 719 146 -

Ebola Virus Disease and Clinical Care Part I: History, Transmission, and Clinical Presentation
Ebola Virus Disease and Clinical Care Part I: History, Transmission, and Clinical Presentation This lecture is on Ebola virus disease (EVD) and clinical care. This is part one of a three-part lecture on this topic. Preparing Healthcare Workers to Work in Ebola Treatment Units (ETUs) in Africa This lecture will focus on EVD in the West African setting. Ebola Virus Disease and Clinical Care: The training and information you receive in this course will Part I: History, Transmission, and Clinical not cover the use of certain interventions such as intubation Presentation or dialysis which are not available in West African Ebola Treatment Units (ETUs). You will need supplemental training This presentation is current as of December 2014. This presentation contains materials from Centers for Disease Control and to care for patients appropriately in countries where advanced Prevention (CDC), Médecins Sans Frontières (MSF), and World Health Organization (WHO). care is available. U.S. Department of Health and Human Services U.S. Department of Health and Human Services Centers for Disease Control and Prevention Centers for Disease Control and Prevention version 12.03.2014 The learning objectives for this lecture are to: Learning Objectives ▶ Describe the routes of Ebola virus transmission Describe the routes of Ebola virus transmission Explain when and how patients are infectious ▶ Explain when and how patients are infectious Describe the clinical features of patients with Ebola ▶ Describe screening criteria for Ebola virus disease Describe the clinical features of patients with Ebola (EVD) used in West Africa Explain how to identify patients with suspected ▶ Describe screening criteria for EVD used in West Africa EVD who present to the ETU ▶ Explain how to identify patients with suspected EVD who present to the ETU This presentation contains materials from CDC, MSF, and WHO 2 A number of different viruses cause viral hemorrhagic fever. -

Development of an Antibody Cocktail for Treatment of Sudan Virus Infection
Development of an antibody cocktail for treatment of Sudan virus infection Andrew S. Herberta,b, Jeffery W. Froudea,1, Ramon A. Ortiza, Ana I. Kuehnea, Danielle E. Doroskya, Russell R. Bakkena, Samantha E. Zaka,b, Nicole M. Josleyna,b, Konstantin Musiychukc, R. Mark Jonesc, Brian Greenc, Stephen J. Streatfieldc, Anna Z. Wecd,2, Natasha Bohorovae, Ognian Bohorove, Do H. Kime, Michael H. Paulye, Jesus Velascoe, Kevin J. Whaleye, Spencer W. Stoniera,b,3, Zachary A. Bornholdte, Kartik Chandrand, Larry Zeitline, Darryl Sampeyf, Vidadi Yusibovc,4, and John M. Dyea,5 aVirology Division, United States Army Medical Research Institute of Infectious Diseases, Fort Detrick, MD 21702; bThe Geneva Foundation, Tacoma, WA 98402; cFraunhofer USA Center for Molecular Biotechnology, Newark, DE 19711; dDepartment of Microbiology and Immunology, Albert Einstein College of Medicine, Bronx, NY 10461; eMapp Biopharmaceutical, Inc., San Diego, CA 92121; and fBioFactura, Inc., Frederick, MD 21701 Edited by Y. Kawaoka, University of Wisconsin–Madison/University of Tokyo, Madison, WI, and approved December 30, 2019 (received for review August 28, 2019) Antibody-based therapies are a promising treatment option for antibody-based immunotherapies. Subsequently, several indepen- managing ebolavirus infections. Several Ebola virus (EBOV)-specific dent groups reported the postexposure efficacy of monoclonal and, more recently, pan-ebolavirus antibody cocktails have been antibody (mAb)-based immunotherapies against EVD in ma- described. Here, we report the development and assessment of a caques when administered as mixtures of two or more mAbs (14–17). Sudan virus (SUDV)-specific antibody cocktail. We produced a panel These landmark studies demonstrated that combination mAb- of SUDV glycoprotein (GP)-specific human chimeric monoclonal based immunotherapies are a viable treatment option for EVD antibodies (mAbs) using both plant and mammalian expression and spurred therapeutic antibody development for filoviruses. -
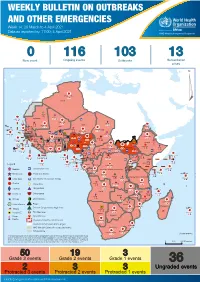
Health Emergency Information and Risk Assessment Health Emergency Information and Risk Assessment Overview
1 Health Emergency Information and Risk Assessment Health Emergency Information and Risk Assessment Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme (WHE) is currently monitoring 60 events in the region. This week’s edition covers key ongoing events, including: 2 Overview Ebola virus disease outbreak in the Democratic Republic of the Congo 3 - 6 Ongoing events Cholera in Burundi Cholera in Cameroon 7 Summary of major Yellow fever in Nigeria. issues challenges and proposed actions For each of these events, a brief description, followed by public health measures implemented and an interpretation of the situation is provided. 8 All events currently being monitored Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo (DRC) is in a critical phase as it enters its sixth month since the declaration of the outbreak. Despite the use of an effective vaccine, novel therapeutics as well as other EVD strategic interventions, the outbreak is persisting due to security challenges, pockets of community reluctance and inadequate infection prevention and control in some health facilities. Nevertheless, WHO and partners, under the government’s leadership, continue to respond to the EVD outbreak and remain committed to containing the outbreak. The Ministry of Health of Burundi has declared a new outbreak of cholera in the country. This outbreak, which is rapidly evolving, is particularly affecting people living in overcrowded areas, where sanitation conditions are precarious. Given that the risk factors for transmission of water-borne diseases are prevalent in the affected communities, there is a need to aggressively tackle this outbreak at its early stage using relevant sectors in order to avoid further spread.