Ebola Virus Disease Outbreak in North Kivu, DRC, 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Meas, Conservation and Conflict: a Case Study of Virunga National Park
© 2008 International Institute for Sustainable Development (IISD) Published by the International Institute for Sustainable Development MEAs, Conservation and Conflict The International Institute for Sustainable Development contributes to sustainable development by advancing policy recommendations on international trade and investment, economic policy, climate change, A case study of Virunga Nationalmeasurement Park, and DRCassessmen t, and natural resources management. Through the Internet, we report on international negotiations and share knowledge gained through collaborative projects with global partners, resulting in more rigorous research, capacity building in developing countries and better dialogue between North and South. IISD’s vision is better living for all— sustainably; its mission is to champion innovation, enabling societies to live sustainably. IISD is registered as a charitable Alec Crawford organization in Canada and has 501(c)(3) status in the United States. IISD receives core Johannah Bernstein operating support from the Government of Canada, provided through the Canadian International Development Agency (CIDA), the International Development Research Centre October 2008 (IDRC) and Environment Canada; and from the Province of Manitoba. The institute receives project funding from numerous governments inside and outside Canada, United Nations agencies, foundations and the priate sector. International Institute for Sustainable Development 161 Portage Avenue East, 6th Floor Winnipeg, Manitoba Canada R3B 0Y4 Tel: +1 (204) 958–7700 Fax: +1 (204) 958–7710 © 2008 International Institute for Sustainable Development (IISD) Published by the International Institute for MEAs, Conservation Sustainable Development and Conflict The International Institute for Sustainable Development contributes to sustainable A case study of Virunga development by advancing policy recommendations on international trade and investment, economic National Park, DRC policy, climate change, measurement and assessment, and natural resources management. -

Of the United Nations Mission in the DRC / MONUC – MONUSCO
Assessing the of the United Nations Mission in the DRC / MONUC – MONUSCO REPORT 3/2019 Publisher: Norwegian Institute of International Affairs Copyright: © Norwegian Institute of International Affairs 2019 ISBN: 978-82-7002-346-2 Any views expressed in this publication are those of the author. Tey should not be interpreted as reflecting the views of the Norwegian Institute of International Affairs. Te text may not be re-published in part or in full without the permission of NUPI and the authors. Visiting address: C.J. Hambros plass 2d Address: P.O. Box 8159 Dep. NO-0033 Oslo, Norway Internet: effectivepeaceops.net | www.nupi.no E-mail: [email protected] Fax: [+ 47] 22 99 40 50 Tel: [+ 47] 22 99 40 00 Assessing the Efectiveness of the UN Missions in the DRC (MONUC-MONUSCO) Lead Author Dr Alexandra Novosseloff, International Peace Institute (IPI), New York and Norwegian Institute of International Affairs (NUPI), Oslo Co-authors Dr Adriana Erthal Abdenur, Igarapé Institute, Rio de Janeiro, Brazil Prof. Tomas Mandrup, Stellenbosch University, South Africa, and Royal Danish Defence College, Copenhagen Aaron Pangburn, Social Science Research Council (SSRC), New York Data Contributors Ryan Rappa and Paul von Chamier, Center on International Cooperation (CIC), New York University, New York EPON Series Editor Dr Cedric de Coning, NUPI External Reference Group Dr Tatiana Carayannis, SSRC, New York Lisa Sharland, Australian Strategic Policy Institute, Canberra Dr Charles Hunt, Royal Melbourne Institute of Technology (RMIT) University, Australia Adam Day, Centre for Policy Research, UN University, New York Cover photo: UN Photo/Sylvain Liechti UN Photo/ Abel Kavanagh Contents Acknowledgements 5 Acronyms 7 Executive Summary 13 Te effectiveness of the UN Missions in the DRC across eight critical dimensions 14 Strategic and Operational Impact of the UN Missions in the DRC 18 Constraints and Challenges of the UN Missions in the DRC 18 Current Dilemmas 19 Introduction 21 Section 1. -

Download File
UNICEF DRC | COVID-19 Situation Report COVID-19 Situation Report #9 29 May-10 June 2020 /Desjardins COVID-19 overview Highlights (as of 10 June 2020) 25702 • 4.4 million children have access to distance learning UNI3 confirmed thanks to partnerships with 268 radio stations and 20 TV 4,480 cases channels © UNICEF/ UNICEF’s response deaths • More than 19 million people reached with key messages 96 on how to prevent COVID-19 people 565 recovered • 29,870 calls managed by the COVID-19 Hotline • 4,338 people (including 811 children) affected by COVID-19 cases under 388 investigation and 837 frontline workers provided with psychosocial support • More than 200,000 community masks distributed 2.3% Fatality Rate 392 new samples tested UNICEF’s COVID-19 Response Kinshasa recorded 88.8% (3,980) of all confirmed cases. Other affected provinces including # of cases are: # of people reached on COVID-19 through North Kivu (35) South Kivu (89) messaging on prevention and access to 48% Ituri (2) Kongo Central (221) Haut RCCE* services Katanga (38) Kwilu (2) Kwango (1) # of people reached with critical WASH Haut Lomami (1) Tshopo (1) supplies (including hygiene items) and services 78% IPC** Equateur (1) # of children who are victims of violence, including GBV, abuse, neglect or living outside 88% DRC COVID-19 Response PSS*** of a family setting that are identified and… Funding Status # of children and women receiving essential healthcare services in UNICEF supported 34% Health facilities Funds # of caregivers of children (0-23 months) available* DRC COVID-19 reached with messages on breadstfeeding in 15% 30% Funding the context of COVID-19 requirements* : Nutrition $ 58,036,209 # of children supported with distance/home- 29% based learning Funding Education Gap 70% 0% 20% 40% 60% 80% 100% *Funds available include 9 million USD * Risk Communication and Community Engagement UNICEF regular ressources allocated by ** Infection Prevention and Control the office for first response needs. -

UN Security Council, Children and Armed Conflict in the DRC, Report of the Secretary General, October
United Nations S/2020/1030 Security Council Distr.: General 19 October 2020 Original: English Children and armed conflict in the Democratic Republic of the Congo Report of the Secretary-General Summary The present report, submitted pursuant to Security Council resolution 1612 (2005) and subsequent resolutions, is the seventh report of the Secretary-General on children and armed conflict in the Democratic Republic of the Congo. It covers the period from 1 January 2018 to 31 March 2020 and the information provided focuses on the six grave violations committed against children, the perpetrators thereof and the context in which the violations took place. The report sets out the trends and patterns of grave violations against children by all parties to the conflict and provides details on progress made in addressing grave violations against children, including through action plan implementation. The report concludes with a series of recommendations to end and prevent grave violations against children in the Democratic Republic of the Congo and improve the protection of children. 20-13818 (E) 171120 *2013818* S/2020/1030 I. Introduction 1. The present report, submitted pursuant to Security Council resolution 1612 (2005) and subsequent resolutions, is the seventh report of the Secretary-General on children and armed conflict in the Democratic Republic of the Congo and covers the period from 1 January 2018 to 31 March 2020. It contains information on the trends and patterns of grave violations against children since the previous report (S/2018/502) and an outline of the progress and challenges since the adoption by the Working Group on Children and Armed Conflict of its conclusions on children and armed conflict in the Democratic Republic of the Congo, in July 2018 (S/AC.51/2018/2). -

Banyamulenge, Congolese Tutsis, Kinshasa
Response to Information Request COD103417.FE Immigration and Refugee Board of Canada www.irb-cisr.gc.ca Français Home Contact Us Help Search canada.gc.ca Home > Research > Responses to Information Requests RESPONSES TO INFORMATION REQUESTS (RIRs) New Search | About RIRs | Help The Board 31 March 2010 About the Board COD103417.FE Biographies Organization Chart Democratic Republic of the Congo: The treatment of the Banyamulenge, or Congolese Tutsis, living in Kinshasa and in the provinces of North Kivu and South Employment Kivu Legal and Policy Research Directorate, Immigration and Refugee Board of Canada, Ottawa References Publications Situation of the Banyamulenge in Kinshasa Tribunal Several sources consulted by the Research Directorate indicated that the Refugee Protection Banyamulenge, or Congolese Tutsis, do not have any particular problems in Division Kinshasa (Journalist 9 Mar. 2010; Le Phare 22 Feb. 2010; VSV 18 Feb. 2010). Immigration Division During a 18 February 2010 telephone interview with the Research Directorate, Immigration Appeal a representative of Voice of the Voiceless for the Defence of Human Rights (La Voix Division des sans voix pour les droits de l'homme, VSV), a human rights non-governmental Decisions organization (NGO) dedicated to defending human rights in the Democratic Republic of the Congo (DRC) (VSV n.d.), stated that his organization has never Forms been aware of [translation] “a case in which a person was mistreated by the Statistics authorities or the Kinshasa population in general” solely because that person was Research of Banyamulenge ethnic origin. Moreover, in correspondence sent to the Research Directorate on 22 February 2010, the manager of the Kinshasa newspaper Le Phare Research Program wrote the following: National Documentation [translation] Packages There are no problems where the Banyamulenge-or Tutsis-in Kinshasa are Issue Papers and concerned. -

Democratic Republic of the Congo – Ebola Outbreaks SEPTEMBER 30, 2020
Fact Sheet #10 Fiscal Year (FY) 2020 Democratic Republic of the Congo – Ebola Outbreaks SEPTEMBER 30, 2020 SITUATION AT A GLANCE 128 53 13 3,470 2,287 Total Confirmed and Total EVD-Related Total EVD-Affected Total Confirmed and Total EVD-Related Probable EVD Cases in Deaths in Équateur Health Zones in Probable EVD Cases in Deaths in Eastern DRC Équateur Équateur Eastern DRC at End of at End of Outbreak Outbreak MoH – September 30, 2020 MoH – September 30, 2020 MoH – September 30, 2020 MoH – June 25, 2020 MoH – June 25, 2020 Health actors remain concerned about surveillance gaps in northwestern DRC’s Équateur Province. In recent weeks, several contacts of EVD patients have travelled undetected to neighboring RoC and the DRC’s Mai- Ndombe Province, heightening the risk of regional EVD spread. Logistics coordination in Equateur has significantly improved in recent weeks, with response actors establishing a Logistics Cluster in September. The 90-day enhanced surveillance period in eastern DRC ended on September 25. TOTAL USAID HUMANITARIAN FUNDING USAID/BHA1,2 $152,614,242 For the DRC Ebola Outbreaks Response in FY 2020 USAID/GH in $2,500,000 Neighboring Countries3 For complete funding breakdown with partners, see funding chart on page 6 Total $155,114,2424 1USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 Total USAID/BHA funding includes non-food humanitarian assistance from the former Office of U.S. Foreign Disaster Assistance. 3 USAID’s Bureau for Global Health (USAID/GH) 4 Some of the USAID funding intended for Ebola virus disease (EVD)-related programs in eastern Democratic Republic of the Congo (DRC) is now supporting EVD response activities in Équateur. -
Understanding People's Resistance to Ebola Responses in The
FROM BIOLEGITIMACY TO ANTIHUMANITARIANISM | MAY 2021 Photo by: Ernest Katembo Ngetha. From Biolegitimacy to Antihumanitarianism: Understanding People’s Resistance to Ebola Responses in the Democratic Republic of the Congo Aymar Nyenyezi Bisoka, Koen Vlassenroot, and Lucien Ramazani 8 Congo Research Briefs | Issue 8 FROM BIOLEGITIMACY TO ANTIHUMANITARIANISM: UNDERSTANDING PEOPLE’S RESISTANCE TO EBOLA RESPONSES IN THE DEMOCRATIC REPUBLIC OF THE CONGO Aymar Nyenyezi Bisoka, Koen Vlassenroot, and Lucien Ramazani1 INTRODUCTION authorities and their ineffectiveness in providing security and creating The tenth outbreak of Ebola hemorrhagic fever in the Democratic lasting peace in areas hit by conflict. In such areas, people prioritize Republic of the Congo (DRC) officially started in August 2018 security above health provisions and feel abandoned by those they in the eastern province of North Kivu, leading the World Health expect to care about them. As one respondent told us, “we die more Organization (WHO), on July 17, 2019, to recognize it as a “public from war than from Ebola and no one cares about it.”4 The local health emergency of international concern.”2 At its formal conclusion population experienced the Ebola health crisis as an opportunity not on June 26, 2020, the pandemic had resulted in 3,470 reported to aim for better health care but to demand protection and peace. cases, including 2,287 deaths.3 Despite its devastating impact, local These observations tell us that, rather than accepting the health- populations seemed to be skeptical about the existence of the new care priorities of humanitarian interventions, people living in North pandemic. Consequently, the outbreak saw substantial and often Kivu saw the pandemic as a moment of struggle and resistance fierce local resistance to the medical response, including armed and mobilized to express their demands to a wide range of public attacks on Ebola treatment centers (ETCs) and violence toward authorities. -

Report on Violations of Human Rights and International Humanitarian Law by the Allied Democratic Forces Armed
UNITED NATIONS JOINT HUMAN RIGHTS OFFICE OHCHR-MONUSCO Report on violations of human rights and international humanitarian law by the Allied Democratic Forces armed group and by members of the defense and security forces in Beni territory, North Kivu province and Irumu and Mambasa territories, Ituri province, between 1 January 2019 and 31 January 2020 July 2020 Table of contents Summary ......................................................................................................................................................................... 4 I. Methodology and challenges encountered ............................................................................................ 7 II. Overview of the armed group Allied Democratic Forces (ADF) ................................................. 8 III. Context of the attacks in Beni territory ................................................................................................. 8 A. Evolution of the attacks from January 2015 to December 2018 .................................................. 8 B. Context of the attacks from 1 January 2019 and 31 January 2020 ............................................ 9 IV. Modus operandi............................................................................................................................................. 11 V. Human rights violations and abuses and violations of international humanitarian law . 11 A. By ADF combattants .................................................................................................................................. -
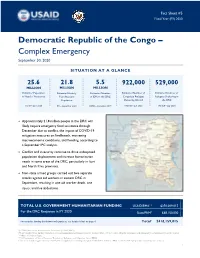
DRC Complex Emergency Fact Sheet #5 09.30.2020
Fact Sheet #5 Fiscal Year (FY) 2020 Democratic Republic of the Congo – Complex Emergency September 30, 2020 SITUATION AT A GLANCE 25.6 21.8 5.5 922,000 529,000 MILLION MILLION MILLION Estimated Population Estimated Acutely Estimated Number Estimated Number of Estimated Number of in Need of Assistance Congolese Refugees Refugees Sheltering in Food Insecure of IDPs in the DRC Population Sheltering Abroad the DRC OCHA – June 2020 UNHCR – July 2020 UNHCR – July 2020 IPC – September 2020 OCHA – December 2019 Approximately 21.8 million people in the DRC will likely require emergency food assistance through December due to conflict, the impact of COVID-19 mitigation measures on livelihoods, worsening macroeconomic conditions, and flooding, according to a September IPC analysis. Conflict and insecurity continue to drive widespread population displacement and increase humanitarian needs in some areas of the DRC, particularly in Ituri and North Kivu provinces. Non-state armed groups carried out two separate attacks against aid workers in eastern DRC in September, resulting in one aid worker death, one injury, and five abductions. TOTAL U.S. GOVERNMENT HUMANITARIAN FUNDING USAID/BHA1,2 $350,009,015 For the DRC Response in FY 2020 State/PRM3 $68,150,000 For complete funding breakdown with partners, see detailed chart on page 6 Total4 $418,159,015 1USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 Total USAID/BHA funding includes non-food humanitarian assistance from the former Office of U.S. Foreign Disaster Assistance and emergency food assistance from the former Office of Food for Peace. 3 U.S. Department of State’s Bureau of Population, Refugees, and Migration (State/PRM) 4 This total includes approximately $23,833,699 in supplemental funding through USAID/BHA and State/PRM for COVID-19 preparedness and response activities. -

Dengue Fever in Senegal 6 - 7 Ongoing Events Ebola Virus Disease in the Democratic Republic of the Congo Humanitarian Crisis in Cameroon
Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme is currently monitoring 58 events in the region. This week’s edition covers key new and ongoing events, including: 2 Overview Hepatitis E in Central African Republic 3 - 5 New events Monkeypox in Central African Republic Dengue fever in Senegal 6 - 7 Ongoing events Ebola virus disease in the Democratic Republic of the Congo Humanitarian crisis in Cameroon. 8 Summary of major issues challenges and For each of these events, a brief description, followed by public health proposed actions measures implemented and an interpretation of the situation is provided. 9 All events currently A table is provided at the end of the bulletin with information on all new and being monitored ongoing public health events currently being monitored in the region, as well as events that have recently been closed. Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo has reached a critical juncture, marked by a precarious security situation, persistence of pockets of community resistance/ mistrust and expanding geographical spread of the disease. During the reporting week, there was an incident involving a response team performing burial activity in Butembo. This came barely days following a widespread community strike (“ville morte”) in Beni and several towns, and an earlier armed attack in Beni. These incidents severely disrupted most outbreak control interventions. Meanwhile, EVD cases have been confirmed in new areas with worse insecurity and in close proximity to the border with Uganda. -

Fnl Operations and Additional Updates
Frederick National Laboratory Operations and Additional Updates Ethan Dmitrovsky, M.D. President, Leidos Biomedical Research and Laboratory Laboratory Director, Frederick National Laboratory for Cancer Research DEPARTMENT OF HEALTH AND HUMAN SERVICES • National Institutes of Health • National Cancer Institute Frederick National Laboratory is a Federally Funded Research and Development Center operated by Leidos Biomedical Research, Inc., for the National Cancer Institute Session Objectives • Review the Frederick National Laboratory rapid response to the pandemic. This is a case study for a Federally Funded Research and Development Center. • Show that this pivot did not prevent decisive quantitative or discovery science, translational research, and clinical trials. • Cite NCI and NIAID programs with major recent progress. • Answer your questions. Federally Funded Research and Development Center Operations Federally Funded Research and Development Center Contract Task Order Portfolio: • 5 Operational Task Orders - Benefits of services are recurring with annual funded appropriations. • NCI Task Order, 3 NIAID Task Orders, 1 Lease Task Order • 98 are Non-operational Task Orders • 38 are in Clinical Group • 47 are in Scientific Group • 13 are Facility or Infrastructure Refurbishments Task Orders • Extensive outreach to the broader research community is through subcontracting. Frederick National Laboratory Pivot with National Cancer Institute to Combat COVID-19 COVID-19 Publications ●Liu, G., et al. Cell Sys., In press, 2020. Pivot to ●Beigel, J.H. et al. New Engl. J. COVID-19 Med., 2020 ●Hicks, J., et al. medRxiv Response doi: https://doi.org/10.1101/2020.06 .22.20137695 Identifying genetic Testing and Clinical Trials to ●Klumpp-Thomas C., et al. determinants of validating Combat COVID-19 ► Identifying medRxivdoi: https://doi.org/10.110 SARS CoV 2 serologic assays Small molecule 1/2020.05.21.20109280. -

To Ebola Reston
WHO/HSE/EPR/2009.2 WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 EPIDEMIC AND PANDEMIC ALERT AND RESPONSE WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 © World Health Organization 2009 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distin- guished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the policies of the World Health Organization.