Emergence of Monkeypox — West and Central Africa, 1970–2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arboviral Infection Surveillance Protocol
April 2013 Arboviral Infection Surveillance Protocol Arboviruses endemic to the U.S. include Eastern equine encephalitis virus (EEE), La Crosse encephalitis virus (LAC), Saint Louis encephalitis virus (SLE), West Nile virus (WNV), Western equine encephalitis virus (WEE), and the tickborne Powassan encephalitis virus (POW). See other materials for information on non-endemic arboviruses (e.g., dengue fever and yellow fever) Provider Responsibilities 1. Report suspect and confirmed cases of arbovirus infection (including copies of lab results) to the local health department within one week of diagnosis. Supply requested clinical information to the local health department to assist with case ascertainment. 2. Assure appropriate testing is completed for patients with suspected arboviral infection. The preferred diagnostic test is testing of virus-specific IgM antibodies in serum or cerebrospinal fluid (CSF). In West Virginia, appropriate arbovirus testing should include EEE, LAC, SLE, and WNV. Testing for a complete arboviral panel is available free of charge through the West Virginia Office of Laboratory Services (OLS). Laboratory Responsibilities 1. Report positive laboratory results for arbovirus infection to the local health department within 1 week. 2. Submit positive arboviral samples to the Office of Laboratory Services within 1 week. 3. Appropriate testing for patients with suspected arboviral infection includes testing of virus-specific IgM antibodies in serum or CSF. In West Virginia, testing should routinely be conducted for WNV, EEE, SLE, and LAC. A complete arboviral panel is available free of charge through OLS. For more information go to: http://www.wvdhhr.org/labservices/labs/virology/arbovirus.cfm Local Health Responsibilities 1. Conduct an appropriate case investigation. -

Poxvirus and Rabies Branch (PRB) Fact Sheet
Poxvirus & Rabies Branch (PRB) The epidemiologists, laboratory scientists, and public health professionals in PRB are responsible for surveillance, control, and prevention of illness and death due to poxviruses and rabies. Our Work Laboratory Reference, Diagnostics, & Training PRB’s provides laboratory reference, diagnostic services, and trainings to state and local health departments, the Department of Defense (DOD), international organizations, and the Laboratory Response Network (over 150 labs across the U.S. prepared to respond to bioterrorism). PRB collaborates with the private sector to develop and evaluate novel diagnostic assays, therapeutics, and vaccines for rabies and pox-related viruses. The branch maintains high-containment laboratories (BSL3 &4) to safely conduct public health research. Research & Surveillance PRB conducts research studies on the microbiology, molecular biology, pathogenesis (disease process), ecology, and evolution of Our Pathogens poxviruses and rabies. The branch monitors the incidence rates of PRB’s Poxvirus Team provides subject matter these diseases in the U.S. and internationally. expertise on: Expert Consultation Orthopoxviruses, including PRB provides consultation regarding poxvirus and rabies- Smallpox associated diseases and their diagnoses, prevention, control, and Monkeypox treatments. Assistance is offered to healthcare providers, academic Cowpox institutions, state and local health departments, other government Vaccinia Virus agencies, and the general public. PRB collaborates with non- governmental organizations to develop risk communication Parapoxviruses, including tools for disease prevention. The branch provides training on Orf Virus simple surveillance techniques and trains healthcare workers on monkeypox in the Democratic Republic of the Congo (DRC). PRB Pseudocowpox collaborates with the national government of Haiti on a rabies surveillance and control program which includes health education, enhanced diagnostics, surveillance, and an extensive dog vaccination campaign. -

MDHHS BOL Mosquito-Borne and Tick-Borne Disease Testing
MDHHS BUREAU OF LABORATORIES MOSQUITO-BORNE AND TICK-BORNE DISEASE TESTING MOSQUITO-BORNE DISEASES The Michigan Department of Health and Human Services Bureau of Laboratories (MDHHS BOL) offers comprehensive testing on clinical specimens for the following viral mosquito-borne diseases (also known as arboviruses) of concern in Michigan: California Group encephalitis viruses including La Crosse encephalitis virus (LAC) and Jamestown Canyon virus (JCV), Eastern Equine encephalitis virus (EEE), St. Louis encephalitis virus (SLE), and West Nile virus (WNV). Testing is available free of charge through Michigan healthcare providers for their patients. Testing for mosquito-borne viruses should be considered in patients presenting with meningitis, encephalitis, or other acute neurologic illness in which an infectious etiology is suspected during the summer months in Michigan. Methodologies include: • IgM detection for five arboviruses (LAC, JCV, EEE, SLE, WNV) • Molecular detection (PCR) for WNV only • Plaque Reduction Neutralization Test (PRNT) is also available and may be performed on select samples when indicated The preferred sample for arbovirus serology at MDHHS BOL is cerebral spinal fluid (CSF), followed by paired serum samples (acute and convalescent). In cases where CSF volume may be small, it is recommended to also include an acute serum sample. Please see the following document for detailed instructions on specimen requirements, shipping and handling instructions: http://www.michigan.gov/documents/LSGArbovirus_IgM_Antibody_Panel_8347_7.doc Michigan residents may also be exposed to mosquito-borne viruses when traveling domestically or internationally. In recent years, the most common arboviruses impacting travelers include dengue, Zika and chikungunya virus. MDHHS has the capacity to perform PCR for dengue, chikungunya and Zika virus and IgM for dengue and Zika virus to confirm commercial laboratory arbovirus findings or for complicated medical investigations. -

What Is Veterinary Public Health? Zoonosis
Your Zoonosis Connection Veterinary Public Health Division Volume 4, Issue 1 March 2012 612 Canino Rd., Houston, Texas 77076 Phone: 281-999-3191 Fax: 281-847-1911 Harris County Rabies Update Inside this issue: Rabies continues to be a serious health threat to people and domestic What is Veterinary 2 animals. In the United States prior to 1960, the majority of all animal cases re- Public Health ported to the Centers for Disease Control and Prevention were seen in do- Rabies Submissions 3 mestic animals. Now more than 90% of the cases occur in wild animals. Since the 1950s, human rabies deaths have declined from more than a 100 annually Continuing Education 3 to a couple each year. This reduction in the number of human deaths associat- ed with rabies can be attributed to the implementation of rabies vaccination Zoonosis Trivia 4 laws, oral rabies vaccination programs, improved public health practices and the increased administration of post-exposure prophylaxis. Did you know? Veterinarians are In Harris County, rabies was last documented in a dog in 1979 and in a cat in uniquely qualified to 1986. However, rabies continues to be enzootic in our bat population. In address issues and 2011, 4.3% of bats submitted for testing were positive for rabies, which has de- concerns related to clined from 7.9% in 2010 (see table below). Last year, one horse and two the interactions of skunks tested positive for rabies in Harris County. The horse was infected people, animals, and with the South Central Skunk strain of rabies, which often spills over into oth- the environment. -

Dengue Fever in Senegal 6 - 7 Ongoing Events Ebola Virus Disease in the Democratic Republic of the Congo Humanitarian Crisis in Cameroon
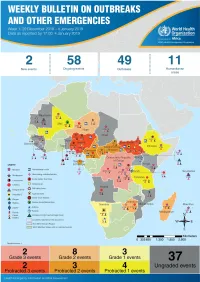
Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme is currently monitoring 58 events in the region. This week’s edition covers key new and ongoing events, including: 2 Overview Hepatitis E in Central African Republic 3 - 5 New events Monkeypox in Central African Republic Dengue fever in Senegal 6 - 7 Ongoing events Ebola virus disease in the Democratic Republic of the Congo Humanitarian crisis in Cameroon. 8 Summary of major issues challenges and For each of these events, a brief description, followed by public health proposed actions measures implemented and an interpretation of the situation is provided. 9 All events currently A table is provided at the end of the bulletin with information on all new and being monitored ongoing public health events currently being monitored in the region, as well as events that have recently been closed. Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo has reached a critical juncture, marked by a precarious security situation, persistence of pockets of community resistance/ mistrust and expanding geographical spread of the disease. During the reporting week, there was an incident involving a response team performing burial activity in Butembo. This came barely days following a widespread community strike (“ville morte”) in Beni and several towns, and an earlier armed attack in Beni. These incidents severely disrupted most outbreak control interventions. Meanwhile, EVD cases have been confirmed in new areas with worse insecurity and in close proximity to the border with Uganda. -

Imported Monkeypox, Singapore
DISPATCHES Imported Monkeypox, Singapore Sarah Ee Fang Yong, Oon Tek Ng, Zheng Jie Marc Ho, Tze Minn Mak, Kalisvar Marimuthu, Shawn Vasoo, Tsin Wen Yeo, Yi Kai Ng, Lin Cui, Zannatul Ferdous, Po Ying Chia, Bryan Jun Wei Aw, Charmaine Malenab Manauis, Constance Khia Ki Low, Guanhao Chan, Xinyi Peh, Poh Lian Lim, Li Ping Angela Chow, Monica Chan, Vernon Jian Ming Lee, Raymond Tzer Pin Lin, Mok Kwee Derrick Heng, Yee Sin Leo In May 2019, we investigated monkeypox in a traveler and public health management for this case, together from Nigeria to Singapore. The public health response with lessons learned and implications for control. included rapid identification of contacts, use of quaran- tine, and postexposure smallpox vaccination. No sec- The Case ondary cases were identified. Countries should develop On May 8, 2019, monkeypox was laboratory-con- surveillance systems to detect emerging infectious dis- firmed in a 38-year-old man from Nigeria who had eases globally. traveled to Singapore. The man resided in Delta State, Nigeria, but had attended a wedding in Ebonyi State onkeypox is a zoonosis endemic to West and during April 21–23, where he reported ingestion of MCentral Africa; human cases were first report- barbecued bushmeat that might have been contami- ed in 1970 (1). An outbreak ongoing in Nigeria since nated. He did not handle raw meat and had no expo- 2017 is the largest documented (2). Exported cases in sure to wild animals or their products. He held an ad- the United Kingdom and Israel were reported from ministrative job and reported no contact with rodents travelers infected in Nigeria in 2018 (3,4). -

Fragile Transmission Cycles of Tick-Borne Encephalitis Virus May Be Disrupted by Predicted Climate Change
doi 10.1098/rspb.2000.1204 Fragiletransmissionc yclesof tick-borne encephalitisvirusmaybedisruptedbypredicted climatechange Sarah E.Randolph * and David J.Rogers Department of Zoology,University of Oxford, SouthP arks Road, Oxford OX13PS, U K Repeatedpredictions that vector-bornedisease prevalencewill increase withglobal warming are usually basedon univariatemodels. T oaccommodatethe fullrange of constraints, the present-daydistribution of tick-borneencephalitis virus (TBEv) was matched statistically tocurrent climatic variables,to provide a multivariatedescription of present-day areas of disease risk.This was then appliedto outputs ofageneral circulationmodel that predicts howclimatic variablesmay change in the future, andfuture distributions ofTBEv were predicted forthem. Theexpected summer rise intemperature anddecrease inmoisture appearsto drive the distributionof TBEv into higher-latitude and higher-altitude regions progressively throughthe 2020s,2050s and 208 0s.The ¢ naltoe-hold in the 2080smay be con¢ ned to a small partof Scandinavia,including new foci in southern Finland. The reason for this apparentcontraction of the rangeof TBEv is that its transmission cycles dependon a particularpattern oftick seasonal dynamics, whichmay be disrupted byclimate change.The observed marked increase inincidence of tick-borne encephalitisin most parts ofEuropesince 1993may be dueto non-biological causes, such aspoliticaland sociologicalchanges. Keywords: ticks; tick-borneencephalitis; global warming ;climate matching;risk maps the winter withminimum temperatures below 712 8C. 1.INTRODUCTION Further south,in areas with medium tohigh tick densi- Tick-borneencephalitis (TBE) ,causedby two subtypes of ties, further increases intick abundance were related to a £avivirus(TBEv) transmitted bythe ticks Ixodes ricinus combinationof milder winters (fewer dayswith minimum and I.persulcatus ,is the most signi¢cant vector-borne temperatures below 7 7 8C)and extended spring and disease inEurope and Eurasia. -

To Ebola Reston
WHO/HSE/EPR/2009.2 WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 EPIDEMIC AND PANDEMIC ALERT AND RESPONSE WHO experts consultation on Ebola Reston pathogenicity in humans Geneva, Switzerland 1 April 2009 © World Health Organization 2009 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distin- guished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the policies of the World Health Organization. -
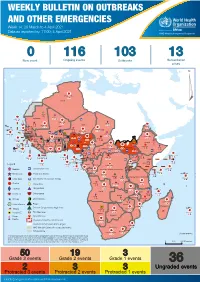
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 14: 29 March to 4 April 2021 Data as reported by: 17:00; 4 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 116 103 13 New event Ongoing events Outbreaks Humanitarian crises 117 622 3 105 Algeria ¤ 36 13 110 0 5 420 164 Mauritania 7 2 10 501 392 110 0 7 0 Niger 17 927 449 Mali 3 334 10 567 0 6 0 2 079 4 4 595 165 Eritrea Cape Verde 38 520 1 037 Chad Senegal 4 918 185 59 0 Gambia 27 0 3 0 17 125 159 9 761 45 Guinea-Bissau 796 17 7 0 Burkina Faso 225 46 215 189 2 963 0 162 593 2 048 Guinea 12 817 150 12 38 397 1 3 662 66 1 1 23 12 Benin 30 0 Nigeria 1 873 71 0 Ethiopia 420 14 481 5 6 188 15 Sierra Leone Togo 3 473 296 53 920 779 52 14 Ghana 5 245 72 Côte d'Ivoire 10 098 108 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 25 0 19 670 120 43 180 237 90 287 740 Cameroon 7 0 28 676 137 5 330 13 138 988 2 224 1 952 87 655 2 51 22 43 0 112 12 6 1 488 6 3 988 79 11 187 6 902 102 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 042 85 41 016 335 Kenya Legend 7 100 90 Gabon Congo 18 504 301 Rwanda Humanitarian crisis 2 212 34 22 482 311 Measles 18 777 111 Democratic Republic of the Congo 9 681 135 Burundi 2 964 6 Monkeypox Ebola virus disease Seychelles 27 930 739 1 525 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 189 0 4 084 20 509 21 Cholera Yellow fever 1 349 5 6 257 229 22 631 542 cVDPV2 Dengue fever 88 930 1 220 Comoros Angola Malawi COVID-19 Chikungunya 33 661 1 123 862 0 3 719 146 -

2018 DSHS Arbovirus Activity
Health and Human Texas Department of State Services Health Services Arbovirus Activity in Texas 2018 Surveillance Report August 2019 Texas Department of State Health Services Zoonosis Control Branch Overview Viruses transmitted by mosquitoes are referred to as arthropod-borne viruses or arboviruses. Arboviruses reported in Texas may include California (CAL) serogroup viruses, chikungunya virus (CHIKV), dengue virus (DENV), eastern equine encephalitis virus (EEEV), Saint Louis encephalitis virus (SLEV), western equine encephalitis virus (WEEV), West Nile virus (WNV), and Zika virus (ZIKV), many of which are endemic or enzootic in the state. In 2018, reported human arboviral disease cases were attributed to WNV (82%), DENV (11%), CHIKV (4%), ZIKV (2%), and CAL (1%) (Table 1). In addition, there were two cases reported as arbovirus disease cases which could not be diagnostically or epidemiologically differentiated between DENV and ZIKV. Animal infections or disease caused by WNV and SLEV were also reported during 2018. Local transmission of DENV, SLEV, and WNV was documented during 2018 (Figure 1). No reports of EEEV or WEEV were received during 2018. Table 1. Year-End Arbovirus Activity Summary, Texas, 2018 Positive Human* Arbovirus Mosquito Avian Equine TOTAL TOTAL Fever Neuroinvasive Severe Deaths PVD‡ Pools (Human) CAL 1 1 1 CHIK 7 7 7 DEN 20 20 20 SLE 2 0 2 WN 1,021 6 19 38 108 146 11 24 1,192 Zika** 4 4 TOTAL 1,023 6 19 65 109 0 178 11 24 1,226 CAL - California serogroup includes California encephalitis, Jamestown Canyon, Keystone, La Crosse, Snowshoe hare and Trivittatus viruses CHIK - Chikungunya DEN - Dengue SLE - Saint Louis encephalitis WN - West Nile ‡PVD - Presumptive viremic blood donors are people who had no symptoms at the time of donating blood through a blood collection agency, but whose blood tested positive when screened for the presence of West Nile virus or Zika virus. -

Ebola Virus Disease and Clinical Care Part I: History, Transmission, and Clinical Presentation
Ebola Virus Disease and Clinical Care Part I: History, Transmission, and Clinical Presentation This lecture is on Ebola virus disease (EVD) and clinical care. This is part one of a three-part lecture on this topic. Preparing Healthcare Workers to Work in Ebola Treatment Units (ETUs) in Africa This lecture will focus on EVD in the West African setting. Ebola Virus Disease and Clinical Care: The training and information you receive in this course will Part I: History, Transmission, and Clinical not cover the use of certain interventions such as intubation Presentation or dialysis which are not available in West African Ebola Treatment Units (ETUs). You will need supplemental training This presentation is current as of December 2014. This presentation contains materials from Centers for Disease Control and to care for patients appropriately in countries where advanced Prevention (CDC), Médecins Sans Frontières (MSF), and World Health Organization (WHO). care is available. U.S. Department of Health and Human Services U.S. Department of Health and Human Services Centers for Disease Control and Prevention Centers for Disease Control and Prevention version 12.03.2014 The learning objectives for this lecture are to: Learning Objectives ▶ Describe the routes of Ebola virus transmission Describe the routes of Ebola virus transmission Explain when and how patients are infectious ▶ Explain when and how patients are infectious Describe the clinical features of patients with Ebola ▶ Describe screening criteria for Ebola virus disease Describe the clinical features of patients with Ebola (EVD) used in West Africa Explain how to identify patients with suspected ▶ Describe screening criteria for EVD used in West Africa EVD who present to the ETU ▶ Explain how to identify patients with suspected EVD who present to the ETU This presentation contains materials from CDC, MSF, and WHO 2 A number of different viruses cause viral hemorrhagic fever. -
Health Emergency Information and Risk Assessment Health Emergency Information and Risk Assessment Overview
1 Health Emergency Information and Risk Assessment Health Emergency Information and Risk Assessment Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme (WHE) is currently monitoring 60 events in the region. This week’s edition covers key ongoing events, including: 2 Overview Ebola virus disease outbreak in the Democratic Republic of the Congo 3 - 6 Ongoing events Cholera in Burundi Cholera in Cameroon 7 Summary of major Yellow fever in Nigeria. issues challenges and proposed actions For each of these events, a brief description, followed by public health measures implemented and an interpretation of the situation is provided. 8 All events currently being monitored Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo (DRC) is in a critical phase as it enters its sixth month since the declaration of the outbreak. Despite the use of an effective vaccine, novel therapeutics as well as other EVD strategic interventions, the outbreak is persisting due to security challenges, pockets of community reluctance and inadequate infection prevention and control in some health facilities. Nevertheless, WHO and partners, under the government’s leadership, continue to respond to the EVD outbreak and remain committed to containing the outbreak. The Ministry of Health of Burundi has declared a new outbreak of cholera in the country. This outbreak, which is rapidly evolving, is particularly affecting people living in overcrowded areas, where sanitation conditions are precarious. Given that the risk factors for transmission of water-borne diseases are prevalent in the affected communities, there is a need to aggressively tackle this outbreak at its early stage using relevant sectors in order to avoid further spread.