Recommended Drug Dilution for Inpatient Leukemia, Lymphoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Application of a Characterized Pre-Clinical
THE APPLICATION OF A CHARACTERIZED PRE-CLINICAL GLIOBLASTOMA ONCOSPHERE MODEL TO IN VITRO AND IN VIVO THERAPEUTIC TESTING by Kelli M. Wilson A dissertation submitted to Johns Hopkins University in conformity with the requirements for the degree of Doctor of Philosophy Baltimore, Maryland March, 2014 ABSTRACT Glioblastoma multiforme (GBM) is a lethal brain cancer with a median survival time (MST) of approximately 15 months following treatment. A serious challenge facing the development of new drugs for the treatment of GBM is that preclinical models fail to replicate the human GBM phenotype. Here we report the Johns Hopkins Oncosphere Panel (JHOP), a panel of GBM oncosphere cell lines. These cell lines were validated by their ability to form tumors intracranially with histological features of human GBM and GBM variant tumors. We then completed whole exome sequencing on JHOP and found that they contain genetic alterations in GBM driver genes such as PTEN, TP53 and CDKN2A. Two JHOP cell lines were utilized in a high throughput drug screen of 466 compounds that were selected to represent late stage clinical development and a wide range of mechanisms. Drugs that were inhibitory in both cell lines were EGFR inhibitors, NF-kB inhibitors and apoptosis activators. We also examined drugs that were inhibitory in a single cell line. Effective drugs in the PTEN null and NF1 wild type cell line showed a limited number of drug targets with EGFR inhibitors being the largest group of cytotoxic compounds. However, in the PTEN mutant, NF1 null cell line, VEGFR/PDGFR inhibitors and dual PIK3/mTOR inhibitors were the most common effective compounds. -

The New Therapeutic Strategies in Pediatric T-Cell Acute Lymphoblastic Leukemia
International Journal of Molecular Sciences Review The New Therapeutic Strategies in Pediatric T-Cell Acute Lymphoblastic Leukemia Marta Weronika Lato 1 , Anna Przysucha 1, Sylwia Grosman 1, Joanna Zawitkowska 2 and Monika Lejman 3,* 1 Student Scientific Society, Laboratory of Genetic Diagnostics, Medical University of Lublin, 20-093 Lublin, Poland; [email protected] (M.W.L.); [email protected] (A.P.); [email protected] (S.G.) 2 Department of Pediatric Hematology, Oncology and Transplantology, Medical University of Lublin, 20-093 Lublin, Poland; [email protected] 3 Laboratory of Genetic Diagnostics, Medical University of Lublin, 20-093 Lublin, Poland * Correspondence: [email protected] Abstract: Childhood acute lymphoblastic leukemia is a genetically heterogeneous cancer that ac- counts for 10–15% of T-cell acute lymphoblastic leukemia (T-ALL) cases. The T-ALL event-free survival rate (EFS) is 85%. The evaluation of structural and numerical chromosomal changes is important for a comprehensive biological characterization of T-ALL, but there are currently no ge- netic prognostic markers. Despite chemotherapy regimens, steroids, and allogeneic transplantation, relapse is the main problem in children with T-ALL. Due to the development of high-throughput molecular methods, the ability to define subgroups of T-ALL has significantly improved in the last few years. The profiling of the gene expression of T-ALL has led to the identification of T-ALL subgroups, and it is important in determining prognostic factors and choosing an appropriate treatment. Novel therapies targeting molecular aberrations offer promise in achieving better first remission with the Citation: Lato, M.W.; Przysucha, A.; hope of preventing relapse. -

LEUSTATIN (Cladribine) Injection Should Be Administered Under the Supervision of a Qualified Physician Experienced in the Use of Antineoplastic Therapy
LEUSTATIN (cladribine) Injection For Intravenous Infusion Only WARNING LEUSTATIN (cladribine) Injection should be administered under the supervision of a qualified physician experienced in the use of antineoplastic therapy. Suppression of bone marrow function should be anticipated. This is usually reversible and appears to be dose dependent. Serious neurological toxicity (including irreversible paraparesis and quadraparesis) has been reported in patients who received LEUSTATIN Injection by continuous infusion at high doses (4 to 9 times the recommended dose for Hairy Cell Leukemia). Neurologic toxicity appears to demonstrate a dose relationship; however, severe neurological toxicity has been reported rarely following treatment with standard cladribine dosing regimens. Acute nephrotoxicity has been observed with high doses of LEUSTATIN (4 to 9 times the recommended dose for Hairy Cell Leukemia), especially when given concomitantly with other nephrotoxic agents/therapies. DESCRIPTION LEUSTATIN (cladribine) Injection (also commonly known as 2-chloro-2΄-deoxy- β -D-adenosine) is a synthetic antineoplastic agent for continuous intravenous infusion. It is a clear, colorless, sterile, preservative-free, isotonic solution. LEUSTATIN Injection is available in single-use vials containing 10 mg (1 mg/mL) of cladribine, a chlorinated purine nucleoside analog. Each milliliter of LEUSTATIN Injection contains 1 mg of the active ingredient and 9 mg (0.15 mEq) of sodium chloride as an inactive ingredient. The solution has a pH range of 5.5 to 8.0. Phosphoric -

Nelarabine) Injection • Severe Neurologic Reactions Have Been Reported
HIGHLIGHTS OF PRESCRIBING INFORMATION --------------------- DOSAGE FORMS AND STRENGTHS -------------- These highlights do not include all the information needed to use 250 mg/50 mL (5 mg/mL) vial (3) ARRANON safely and effectively. See full prescribing information for -------------------------------CONTRAINDICATIONS------------------------ ARRANON. None. ----------------------- WARNINGS AND PRECAUTIONS ---------------- ARRANON (nelarabine) Injection • Severe neurologic reactions have been reported. Monitor for signs and Initial U.S. Approval: 2005 symptoms of neurologic toxicity. (5.1) WARNING: NEUROLOGIC ADVERSE REACTIONS • Hematologic Reactions: Complete blood counts including platelets should See full prescribing information for complete boxed warning. be monitored regularly. (5.2) Severe neurologic adverse reactions have been reported with the use of • Fetal harm can occur if administered to a pregnant woman. Women should ARRANON. These adverse reactions have included altered mental states be advised not to become pregnant when taking ARRANON. (5.3) including severe somnolence, central nervous system effects including ------------------------------ ADVERSE REACTIONS ----------------------- convulsions, and peripheral neuropathy ranging from numbness and The most common (≥ 20%) adverse reactions were: paresthesias to motor weakness and paralysis. There have also been • Adult: anemia, thrombocytopenia, neutropenia, nausea, diarrhea, reports of adverse reactions associated with demyelination, and ascending vomiting, constipation, fatigue, -

Synthesis of Ribavirin, Tecadenoson, and Cladribine by Enzymatic Transglycosylation
catalysts Article Synthesis of Ribavirin, Tecadenoson, and Cladribine by Enzymatic Transglycosylation 1, 2 2,3 2 Marco Rabuffetti y, Teodora Bavaro , Riccardo Semproli , Giulia Cattaneo , Michela Massone 1, Carlo F. Morelli 1 , Giovanna Speranza 1,* and Daniela Ubiali 2,* 1 Department of Chemistry, University of Milan, via Golgi 19, I-20133 Milano, Italy; marco.rabuff[email protected] (M.R.); [email protected] (M.M.); [email protected] (C.F.M.) 2 Department of Drug Sciences, University of Pavia, viale Taramelli 12, I-27100 Pavia, Italy; [email protected] (T.B.); [email protected] (R.S.); [email protected] (G.C.) 3 Consorzio Italbiotec, via Fantoli 15/16, c/o Polo Multimedica, I-20138 Milano, Italy * Correspondence: [email protected] (G.S.); [email protected] (D.U.); Tel.: +39-02-50314097 (G.S.); +39-0382-987889 (D.U.) Present address: Department of Food, Environmental and Nutritional Sciences, University of Milan, y via Mangiagalli 25, I-20133 Milano, Italy. Received: 7 March 2019; Accepted: 8 April 2019; Published: 12 April 2019 Abstract: Despite the impressive progress in nucleoside chemistry to date, the synthesis of nucleoside analogues is still a challenge. Chemoenzymatic synthesis has been proven to overcome most of the constraints of conventional nucleoside chemistry. A purine nucleoside phosphorylase from Aeromonas hydrophila (AhPNP) has been used herein to catalyze the synthesis of Ribavirin, Tecadenoson, and Cladribine, by a “one-pot, one-enzyme” transglycosylation, which is the transfer of the carbohydrate moiety from a nucleoside donor to a heterocyclic base. As the sugar donor, 7-methylguanosine iodide and its 20-deoxy counterpart were synthesized and incubated either with the “purine-like” base or the modified purine of the three selected APIs. -

COMPARISON of the WHO ATC CLASSIFICATION & Ephmra/Intellus Worldwide ANATOMICAL CLASSIFICATION
COMPARISON OF THE WHO ATC CLASSIFICATION & EphMRA/Intellus Worldwide ANATOMICAL CLASSIFICATION: VERSION June 2019 2 Comparison of the WHO ATC Classification and EphMRA / Intellus Worldwide Anatomical Classification The following booklet is designed to improve the understanding of the two classification systems. The development of the two systems had previously taken place separately. EphMRA and WHO are now working together to ensure that there is a convergence of the 2 systems rather than a divergence. In order to better understand the two classification systems, we should pay attention to the way in which substances/products are classified. WHO mainly classifies substances according to the therapeutic or pharmaceutical aspects and in one class only (particular formulations or strengths can be given separate codes, e.g. clonidine in C02A as antihypertensive agent, N02C as anti-migraine product and S01E as ophthalmic product). EphMRA classifies products, mainly according to their indications and use. Therefore, it is possible to find the same compound in several classes, depending on the product, e.g., NAPROXEN tablets can be classified in M1A (antirheumatic), N2B (analgesic) and G2C if indicated for gynaecological conditions only. The purposes of classification are also different: The main purpose of the WHO classification is for international drug utilisation research and for adverse drug reaction monitoring. This classification is recommended by the WHO for use in international drug utilisation research. The EphMRA/Intellus Worldwide classification has a primary objective to satisfy the marketing needs of the pharmaceutical companies. Therefore, a direct comparison is sometimes difficult due to the different nature and purpose of the two systems. -
ATC/DDD Classification
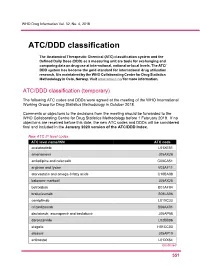
WHO Drug Information Vol. 32, No. 4, 2018 ATC/DDD classification The Anatomical Therapeutic Chemical (ATC) classification system and the Defined Daily Dose (DDD) as a measuring unit are tools for exchanging and comparing data on drug use at international, national or local levels. The ATC/ DDD system has become the gold standard for international drug utilization research. It is maintained by the WHO Collaborating Centre for Drug Statistics Methodology in Oslo, Norway. Visit www.whocc.no/ for more information. ATC/DDD classification (temporary) The following ATC codes and DDDs were agreed at the meeting of the WHO International Working Group for Drug Statistics Methodology in October 2018. Comments or objections to the decisions from the meeting should be forwarded to the WHO Collaborating Centre for Drug Statistics Methodology before 1 February 2019. If no objections are received before this date, the new ATC codes and DDDs will be considered final and included in the January 2020 version of the ATC/DDD Index. New ATC 5th level codes ATC level name/INN ATC code acalabrutinib L01XE51 amenamevir J05AX26 amlodipine and celecoxib C08CA51 arginine and lysine V03AF11 atorvastatin and omega-3 fatty acids C10BA08 baloxavir marboxil J05AX25 betrixaban B01AF04 brolucizumab S01LA06 cemiplimab L01XC33 crizanlizumab B06AX01 daclatasvir, asunaprevir and beclabuvir J05AP58 darolutamide L02BB06 elagolix H01CC03 elbasvir J05AP10 entinostat L01XX64 Continued 5 51 ATC/DDD classification WHO Drug Information Vol. 32, No. 4, 2018 New ATC 5th level codes (continued) -

ARRANON Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION -------------------------------------CONTRAINDICATIONS------------------------ These highlights do not include all the information needed to use None. (4) ARRANON safely and effectively. See full prescribing information for ARRANON. -------------------------WARNINGS AND PRECAUTIONS---------------------- Neurologic Adverse Reactions: Severe neurologic reactions have been ARRANON® (nelarabine) injection, for intravenous use reported. Monitor for signs and symptoms of neurologic toxicity. (5.1) Initial U.S. Approval: 2005 Hematologic Reactions: Complete blood counts including platelets should WARNING: NEUROLOGIC ADVERSE REACTIONS be monitored regularly. (5.2) See full prescribing information for complete boxed warning. Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective Severe neurologic adverse reactions have been reported with the use of contraception; and advise males to use condoms. (5.3, 8.1, 8.3) ARRANON. These adverse reactions have included altered mental states Effects on Ability to Drive and Use Machines: Somnolence may occur. including severe somnolence, central nervous system effects including Advise patients to refrain from these activities until somnolence has convulsions, and peripheral neuropathy ranging from numbness and resolved. (5.6) paresthesias to motor weakness and paralysis. There have also been reports of adverse reactions associated with demyelination, and ascending ------------------------------------ADVERSE REACTIONS------------------------- peripheral neuropathies similar in appearance to Guillain-Barré The most common (≥ 20%) adverse reactions were: syndrome. (5.1) Adult: anemia, thrombocytopenia, neutropenia, nausea, diarrhea, vomiting, constipation, fatigue, pyrexia, cough, and dyspnea. (6.1) Full recovery from these adverse reactions has not always occurred with Pediatric: anemia, neutropenia, thrombocytopenia, and leukopenia. (6.1) cessation of therapy with ARRANON. -

Chemotherapy: Drugs E-O Policy (Chemo Drug E-O)
chemo drug e-o 1 Chemotherapy: Drugs E-O Policy Page updated: September 2020 This section contains policy related to billing for injection services, listed in alphabetical order by generic drug name or drug type. For general billing policy information regarding injections services, refer to the Chemotherapy: An Overview section in this manual. Additional policy information for chemotherapy drug services can be found in the Chemotherapy: Drugs A-D Policy and Chemotherapy: Drugs P-Z Policy sections in this manual. Elotuzumab Elotuzumab is a humanized IgG1 monoclonal antibody that specifically targets the SLAMF7 (signaling lymphocytic activation molecule family member 7) protein. SLAMF7 is expressed on myeloma cells independent of cytogenetic abnormalities. SLAMF7 is also expressed on natural killer cells, plasma cells and at lower levels on specific immune cell subsets of differentiated cells within the hematopoietic lineage. Elotuzumab directly activates natural killer cells through both the SLAMF7 pathway and Fc receptors. Elotuzumab also targets SLAMF7 on myeloma cells and facilitates the interaction with natural killer cells to mediate the killing of myeloma cells through antibody-dependent cellular cytotoxicity (ADCC). Indications Elotuzumab is indicated in combination with lenalidomide and dexamethasone for the treatment of patients ages 18 years or older, with multiple myeloma who have received one to three prior therapies. Pre-medicate with dexamethasone, diphenhydramine, ranitidine and acetaminophen. Advise patients that lenalidomide has the potential to cause fetal harm. Authorization An approved Treatment Authorization Request (TAR) is required for reimbursement. The TAR must state that the treatment is for a patient with multiple myeloma who has received one to three prior therapies. -

Cladribine Injection
PRODUCT MONOGRAPH PrCLADRIBINE INJECTION Solution for Intravenous Injection 1 mg/mL USP Antineoplastic / Chemotherapeutic Agent Fresenius Kabi Canada Ltd. Date of Revision: 165 Galaxy Blvd, Suite 100 June 9, 2015 Toronto, ON M9W 0C8 Control No.: 181078 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION ......................................................... 3 SUMMARY PRODUCT INFORMATION ............................................................................... 3 INDICATIONS AND CLINICAL USE ..................................................................................... 3 CONTRAINDICATIONS .......................................................................................................... 3 WARNINGS AND PRECAUTIONS ......................................................................................... 4 ADVERSE REACTIONS ........................................................................................................... 7 DRUG INTERACTIONS ......................................................................................................... 10 DOSAGE AND ADMINISTRATION ..................................................................................... 11 OVERDOSAGE ....................................................................................................................... 13 ACTION AND CLINICAL PHARMACOLOGY ................................................................... 14 STORAGE AND STABILITY ................................................................................................ -

2015 Antiemesis.Pdf
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Antiemesis Version 2.2015 NCCN.org Continue Version 2.2015, 09/22/15 © National Comprehensive Cancer Network, Inc. 2015, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. Printed by Alexandre Ferreira on 10/25/2015 6:12:07 AM. For personal use only. Not approved for distribution. Copyright © 2015 National Comprehensive Cancer Network, Inc., All Rights Reserved. NCCN Guidelines Version 2.2015 Panel Members NCCN Guidelines Index Antiemesis Table of Contents Antiemesis Discussion David S. Ettinger, MD/Chair † Steve Kirkegaard, PharmD Σ Eric Roeland, MD The Sidney Kimmel Comprehensive Huntsman Cancer Institute UC San Diego Moores Cancer Cancer Center at Johns Hopkins at the University of Utah Center Michael J. Berger, PharmD/Vice Chair, BCOP Σ Dwight D. Kloth, PharmD, BCOP Σ Hope S. Rugo, MD † ‡ The Ohio State University Comprehensive Fox Chase Cancer Center UCSF Helen Diller Family Cancer Center - James Cancer Hospital Comprehensive Cancer Center and Solove Research Institute Ruth Lagman, MD £ Mayo Clinic Cancer Center Bridget Scullion, PharmD, BCOP Jonathan Aston, PharmD, BCOP, BCPS Σ Dana-Farber/Brigham and Women’s Vanderbilt-Ingram Cancer Center Dean Lim, MD † Cancer Center | Massachusetts City of Hope Comprehensive Cancer Center General Hospital Cancer Center Sally Barbour, PharmD, BCOP, CCP Σ Duke Cancer Institute Cynthia Ma, MD, PhD † John Timoney, PharmD, BCOP † Siteman Cancer Center at Barnes-Jewish Memorial Sloan Kettering Cancer Philip J. Bierman, MD † ‡ Hospital and Washington University School Center Fred & Pamela Buffet Cancer Center of Medicine Barbara Todaro, PharmD Σ Debra Brandt, DO Belinda Mandrell, PhD, RN † Roswell Park Cancer Institute Yale Cancer Center/Smilow Cancer Hospital St. -

Chemotherapy and Polyneuropathies Grisold W, Oberndorfer S Windebank AJ European Association of Neurooncology Magazine 2012; 2 (1) 25-36
Volume 2 (2012) // Issue 1 // e-ISSN 2224-3453 Neurology · Neurosurgery · Medical Oncology · Radiotherapy · Paediatric Neuro- oncology · Neuropathology · Neuroradiology · Neuroimaging · Nursing · Patient Issues Chemotherapy and Polyneuropathies Grisold W, Oberndorfer S Windebank AJ European Association of NeuroOncology Magazine 2012; 2 (1) 25-36 Homepage: www.kup.at/ journals/eano/index.html OnlineOnline DatabaseDatabase FeaturingFeaturing Author,Author, KeyKey WordWord andand Full-TextFull-Text SearchSearch THE EUROPEAN ASSOCIATION OF NEUROONCOLOGY Member of the Chemotherapy and Polyneuropathies Chemotherapy and Polyneuropathies Wolfgang Grisold1, Stefan Oberndorfer2, Anthony J Windebank3 Abstract: Peripheral neuropathies induced by taxanes) immediate effects can appear, caused to be caused by chemotherapy or other mecha- chemotherapy (CIPN) are an increasingly frequent by different mechanisms. The substances that nisms, whether treatment needs to be modified problem. Contrary to haematologic side effects, most frequently cause CIPN are vinca alkaloids, or stopped due to CIPN, and what symptomatic which can be treated with haematopoetic taxanes, platin derivates, bortezomib, and tha- treatment should be recommended. growth factors, neither prophylaxis nor specific lidomide. Little is known about synergistic neu- Possible new approaches for the management treatment is available, and only symptomatic rotoxicity caused by previously given chemo- of CIPN could be genetic susceptibility, as there treatment can be offered. therapies, or concomitant chemotherapies. The are some promising advances with vinca alka- CIPN are predominantly sensory, duration-of- role of pre-existent neuropathies on the develop- loids and taxanes. Eur Assoc Neurooncol Mag treatment-dependent neuropathies, which de- ment of a CIPN is generally assumed, but not 2012; 2 (1): 25–36. velop after a typical cumulative dose. Rarely mo- clear.