The Distribution of Sweat Glands Over the Human Body Has So Far Been In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wound Classification
Wound Classification Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State University Welcome! Thank you for joining this webinar about how to assess and measure a wound. 2 A Little About Myself… • Associate professor at Montana State University • Executive editor of the Journal of the World Council of Enterstomal Therapists (JWCET) and WCET International Ostomy Guidelines (2014) • Editorial board member of Ostomy Wound Management and Advances in Skin and Wound Care • Legal consultant • Former NPUAP board member 3 Today We Will Talk About • How to assess a wound • How to measure a wound Please make a note of your questions. Your Quality Improvement (QI) Specialists will follow up with you after this webinar to address them. 4 Assessing and Measuring Wounds • You completed a skin assessment and found a wound. • Now you need to determine what type of wound you found. • If it is a pressure ulcer, you need to determine the stage. 5 Assessing and Measuring Wounds This is important because— • Each type of wound has a different etiology. • Treatment may be very different. However— • Not all wounds are clear cut. • The cause may be multifactoral. 6 Types of Wounds • Vascular (arterial, venous, and mixed) • Neuropathic (diabetic) • Moisture-associated dermatitis • Skin tear • Pressure ulcer 7 Mixed Etiologies Many wounds have mixed etiologies. • There may be both venous and arterial insufficiency. • There may be diabetes and pressure characteristics. 8 Moisture-Associated Skin Damage • Also called perineal dermatitis, diaper rash, incontinence-associated dermatitis (often confused with pressure ulcers) • An inflammation of the skin in the perineal area, on and between the buttocks, into the skin folds, and down the inner thighs • Scaling of the skin with papule and vesicle formation: – These may open, with “weeping” of the skin, which exacerbates skin damage. -

Periodic Acid-Schiff Positive Material Accumulating Within the Lumen of Eccrine Sweat Glands*
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector PERIODIC ACID-SCHIFF POSITIVE MATERIAL ACCUMULATING WITHIN THE LUMEN OF ECCRINE SWEAT GLANDS* GEORGE W. HAMBRICK, JR., M.D. The purpose of this paper is to record findings with regard to diastase-resistant, periodic acid-Schiff positive material in the lumen of eccrine ducts and glands of two individuals. This material has two possible sources in the normal eccrine sweat gland, namely, the cuticle lining of the eccrine duct and the cells of the secretory tubule. Holyoke and Lobits (3) studying 35 normal skin biopsies re- B pp HI D FIG. 1. A. Vertical section through skin of the control area showing dilatation of an eccrine sweat duct with eosinophilic material in the lumen. H. and E., X178. B. Same find- ings as in A above from an area treated daily with 3 per cent hexachloronaphthalene in acetone for one week, Xl7S. C. Section through dermal parts of eccrine duct containing a cast. H. and E., X355. D. Section through dermal eccrine duct containing periodic acid- Schiff positive material in the lumen, X660. *Fromthe Department of Dermatology (Donald M. Pillsbury, M.D., Director), School of Medicine, University of Pennsylvania, Philadelphia 4, Pennsylvania. This study was supported by U. S. Army grant DA-49-007-MD-154. Received for publication March 29, 1957. 213 214 THF JOURNAL OF INVESTIGATIVE DERMATOLOGY ported the presence of material in the lumen of the eccrine duct and gland; they classified the material as amorphous, cast, cellular or bacterial. -

Sweat Gland Myoepithelial Cell Differentiation
Journal of Cell Science 112, 1925-1936 (1999) 1925 Printed in Great Britain © The Company of Biologists Limited 1999 JCS4638 Human sweat gland myoepithelial cells express a unique set of cytokeratins and reveal the potential for alternative epithelial and mesenchymal differentiation states in culture Margarete Schön1,*, Jennifer Benwood1, Therese O’Connell-Willstaedt2 and James G. Rheinwald1,2,‡ 1Division of Dermatology/Department of Medicine, Brigham and Women’s Hospital, and 2Division of Cell Growth and Regulation, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA 02115, USA *Present address: Department of Dermatology, Heinrich-Heine University, Moorenstrasse 5, 40225 Düsseldorf, Germany ‡Author for correspondence (e-mail: [email protected]) Accepted 9 April; published on WWW 26 May 1999 SUMMARY We have characterized precisely the cytokeratin expression myoepithelial cells, a constituent of secretory glands. pattern of sweat gland myoepithelial cells and have Immunostaining of skin sections revealed that only sweat identified conditions for propagating this cell type and gland myoepithelial cells expressed the same pattern of modulating its differentiation in culture. Rare, unstratified keratins and α-sma and lack of E-cadherin as the cell type epithelioid colonies were identified in cultures initiated we had cultured. Interestingly, our immunocytochemical from several specimens of full-thickness human skin. These analysis of ndk, a skin-derived cell line of uncertain cells divided rapidly in medium containing serum, identity, suggests that this line is of myoepithelial origin. epidermal growth factor (EGF), and hydrocortisone, and Earlier immunohistochemical studies by others had found maintained a closely packed, epithelioid morphology when myoepithelial cells to be K7-negative. -

Pressure Ulcer Staging Guide
Pressure Ulcer Staging Guide Pressure Ulcer Staging Guide STAGE I STAGE IV Intact skin with non-blanchable Full thickness tissue loss with exposed redness of a localized area usually Reddened area bone, tendon, or muscle. Slough or eschar may be present on some parts Epidermis over a bony prominence. Darkly Epidermis pigmented skin may not have of the wound bed. Often includes undermining and tunneling. The depth visible blanching; its color may Dermis of a stage IV pressure ulcer varies by Dermis differ from the surrounding area. anatomical location. The bridge of the This area may be painful, firm, soft, nose, ear, occiput, and malleolus do not warmer, or cooler as compared to have subcutaneous tissue and these adjacent tissue. Stage I may be Adipose tissue ulcers can be shallow. Stage IV ulcers Adipose tissue difficult to detect in individuals with can extend into muscle and/or Muscle dark skin tones. May indicate "at supporting structures (e.g., fascia, Muscle risk" persons (a heralding sign of Bone tendon, or joint capsule) making risk). osteomyelitis possible. Exposed bone/ Bone tendon is visible or directly palpable. STAGE II DEEP TISSUE INJURY Partial thickness loss of dermis Blister Purple or maroon localized area of Reddened area presenting as a shallow open ulcer discolored intact skin or blood-filled Epidermis with a red pink wound bed, without Epidermis blister due to damage of underlying soft slough. May also present as an tissue from pressure and/or shear. The intact or open/ruptured serum-filled Dermis area may be preceded by tissue that is Dermis blister. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

Sweat Glands • Oil Glands • Mammary Glands
Chapter 4 The Integumentary System Lecture Presentation by Steven Bassett Southeast Community College © 2015 Pearson Education, Inc. Introduction • The integumentary system is composed of: • Skin • Hair • Nails • Sweat glands • Oil glands • Mammary glands © 2015 Pearson Education, Inc. Introduction • The skin is the most visible organ of the body • Clinicians can tell a lot about the overall health of the body by examining the skin • Skin helps protect from the environment • Skin helps to regulate body temperature © 2015 Pearson Education, Inc. Integumentary Structure and Function • Cutaneous Membrane • Epidermis • Dermis • Accessory Structures • Hair follicles • Exocrine glands • Nails © 2015 Pearson Education, Inc. Figure 4.1 Functional Organization of the Integumentary System Integumentary System FUNCTIONS • Physical protection from • Synthesis and storage • Coordination of immune • Sensory information • Excretion environmental hazards of lipid reserves response to pathogens • Synthesis of vitamin D3 • Thermoregulation and cancers in skin Cutaneous Membrane Accessory Structures Epidermis Dermis Hair Follicles Exocrine Glands Nails • Protects dermis from Papillary Layer Reticular Layer • Produce hairs that • Assist in • Protect and trauma, chemicals protect skull thermoregulation support tips • Nourishes and • Restricts spread of • Controls skin permeability, • Produce hairs that • Excrete wastes of fingers and supports pathogens prevents water loss provide delicate • Lubricate toes epidermis penetrating epidermis • Prevents entry of -

There Are 25 Questions, Each Worth 3 Points and a Short Essay Worth 25 Points. DO YOUR OWN WORK !! Use Your Time Wisely 1. T
Mr. Holder Integumentary System – Unit 5 December 3, 2015 ARC TEST 1.0 DO NOT MARK OR WRITE ON THIS QUIZ !! There are 25 questions, each worth 3 points and a short essay worth 25 points. DO YOUR OWN WORK !! Use Your Time Wisely 1. The Integumentary System is divided into how many layers? a) 2 b) 3 c) 4 d) 6 2. What are the two major groups of membranes covering the human body? a) Epithelial & Mucus b) Cutaneous & Mucus c) Epithelial & Connective Tissue d) None of these 3. Which internal membrane provides protection for your joints? a) Serous b) Synovial c) Cutaneous d) Mucus 4. These membranes line internal cavities exposed to air & excrete a gooey substance. a) Serous b) Synovial c) Cutaneous d) Mucus 5. The Integumentary System protects the human body from … a) Friction b) Hot & Cold Temperature c) Bacteria d) All of These 6. Which stratum of the epidermis is full of keratin, cornified to prevent water loss? a) Basale b) Granulosum c) Corneum d) None of These 7. Which body system extends into the dermis to provide information to your brain? a) Cardiovascular b) Immune c) Integumentary d) Nervous 8. Subcutaneous tissue includes adipose tissue or fat. It is also known as the … a) Dermis b) Papillary Layer c) Hypodermis d) Reticular Layer 9. The dermis is divided into two layers. Which of these is the thickest? a) Papillary b) Reticular c) Basale d) Hypodermis 10. Which stratum of the epidermis is responsible for new cell production? a) Corneum b) Basale c) Granulosum d) Spinosum Page 1 Mr. -

The Anatomy of the Skin of the Chinese Tree Shrew Is Very Similar to That of Human Skin
ZOOLOGICAL RESEARCH The anatomy of the skin of the Chinese tree shrew is very similar to that of human skin DEAR EDITOR, murine model induced by imiquimod (Chuang et al., 2018) and inflammatory mouse model of Behçet's disease induced by The Chinese tree shrew (Tupaia belangeri chinensis) is a HSV-1 (Islam & Sohn, 2018), but the species disparity small mammal closely related to primates. It has a small body sometimes makes them difficult to extrapolate (van der Worp size, low maintenance cost, and a relatively short reproductive et al., 2010). Non-human primates (NHP), like rhesus cycle, all of which has made it the ideal model for the study of macaques, are genetically closer to humans and have a variety of human diseases. In this study, we compared the significant benefits in medical research (Buffalo et al., 2019; anatomy of the skin of the Chinese tree shrew with that of the Zhang et al., 2014). NHP has been used to explore responses rhesus macaque, mouse and human, with the intention of of Leishmania (Viannia) braziliensis cutaneous infection to N- providing the basic data required for the creation of skin methylglucamine antimoniate (Teva et al., 2005) and as disease models using this animal. Paraffin sections, SIVmac239-infected model for studying HIV infection (Zhang hematoxylin-eosin (H&E) staining, masson staining and et al., 2019), to name a few. The NHP model has been proved immunohistochemical techniques were used to examine the to be the best model for biomedical researches. However, dorsal skin structure of the Chinese tree shrew. The epidermis there are also some disadvantages of using NHP as the was shown to be composed of 1–2 layers of cells. -

Basic Biology of the Skin 3
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION CHAPTER Basic Biology of the Skin 3 The skin is often underestimated for its impor- Layers of the skin: tance in health and disease. As a consequence, it’s frequently understudied by chiropractic students 1. Epidermis—the outer most layer of the skin (and perhaps, under-taught by chiropractic that is divided into the following fi ve layers school faculty). It is not our intention to present a from top to bottom. These layers can be mi- comprehensive review of anatomy and physiol- croscopically identifi ed: ogy of the skin, but rather a review of the basic Stratum corneum—also known as the biology of the skin as a prerequisite to the study horny cell layer, consisting mainly of kera- of pathophysiology of skin disease and the study tinocytes (fl at squamous cells) containing of diagnosis and treatment of skin disorders and a protein known as keratin. The thick layer diseases. The following material is presented in prevents water loss and prevents the entry an easy-to-read point format, which, though brief of bacteria. The thickness can vary region- in content, is suffi cient to provide a refresher ally. For example, the stratum corneum of course to mid-level or upper-level chiropractic the hands and feet are thick as they are students and chiropractors. more prone to injury. This layer is continu- Please refer to Figure 3-1, a cross-sectional ously shed but is replaced by new cells from drawing of the skin. This represents a typical the stratum basale (basal cell layer). -

HYPERHIDROSIS 101: Understanding Excessive Sweat
HYPERHIDROSIS 101: Understanding Excessive Sweat Hyperhidrosis is a medical condition in which excessive sweating occurs beyond what is needed to maintain normal body temperature.1,2 Excessive sweating can occur in the hands, feet, underarms or face, and it often interferes with everyday activities.1 Understanding Sweat Sweat glands are small tubular structures in the skin that secrete sweat onto the skin via a duct.3 Eccrine sweat glands are distributed throughout almost the entire human body and they secrete directly onto the surface of the skin.3 Apocrine sweat glands are ten times larger than eccrine sweat glands.3 They are localized in the axilla (underarms) and perianal areas.3 Rather than directly opening onto the skin surface, these glands secrete sweat into the pilary canal of the hair follicle.3 What is Hyperhidrosis? We all sweat. It’s the body’s way of cooling itself and preventing 1 ourselves from overheating. People living with hyperhidrosis, What Causes Us to Sweat? however, sweat when the body doesn’t necessarily need cooling.1 Their sweat is excessive, often visible to others and usually occurs The main reason we sweat is to control without physical exertion or extreme heat. our body temperature.2 There are two different types of hyperhidrosis - primary (also known as focal Here’s how it works: Sensors in our skin can detect changes in temperature hyperhidrosis) and secondary hyperhidrosis.6 Primary hyperhidrosis often begins and relay signals to our brain when we in childhood or adolescence and affects localized areas of the body, including the exercise or when it is hot outside.4 In hands, feet, underarms or face.6 The condition may be inherited and many members turn, our brain signals the sweat glands 7 of the same family may suffer from hyperhidrosis. -

Kumka's Response to Stecco's Fascial Nomenclature Editorial
Journal of Bodywork & Movement Therapies (2014) 18, 591e598 Available online at www.sciencedirect.com ScienceDirect journal homepage: www.elsevier.com/jbmt FASCIA SCIENCE AND CLINICAL APPLICATIONS: RESPONSE Kumka’s response to Stecco’s fascial nomenclature editorial Myroslava Kumka, MD, PhD* Canadian Memorial Chiropractic College, Department of Anatomy, 6100 Leslie Street, Toronto, ON M2H 3J1, Canada Received 12 May 2014; received in revised form 13 May 2014; accepted 26 June 2014 Why are there so many discussions? response to the direction of various strains and stimuli. (De Zordo et al., 2009) Embedded with a range of mechanore- The clinical importance of fasciae (involvement in patho- ceptors and free nerve endings, it appears fascia has a role in logical conditions, manipulation, treatment) makes the proprioception, muscle tonicity, and pain generation. fascial system a subject of investigation using techniques (Schleip et al., 2005) Pathology and injury of fascia could ranging from direct imaging and dissections to in vitro potentially lead to modification of the entire efficiency of cellular modeling and mathematical algorithms (Chaudhry the locomotor system (van der Wal and Pubmed Exact, 2009). et al., 2008; Langevin et al., 2007). Despite being a topic of growing interest worldwide, This tissue is important for all manual therapists as a controversies still exist regarding the official definition, pain generator and potentially treatable entity through soft terminology, classification and clinical significance of fascia tissue and joint manipulative techniques. (Day et al., 2009) (Langevin et al., 2009; Mirkin, 2008). It is also reportedly treated with therapeutic modalities Lack of consistent terminology has a negative effect on such as therapeutic ultrasound, microcurrent, low level international communication within and outside many laser, acupuncture, and extracorporeal shockwave therapy. -
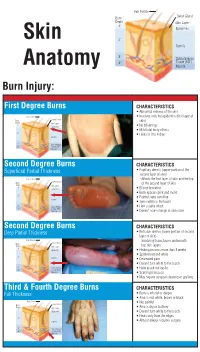
Identifying the Degree of a Burn Poster
Hair Folicle Sweat Gland Burn Depth Skin Layer 1° Epidermis Skin 2° Dermis 3° Subcutaneous 4° Tissue (FAT) Anatomy Muscle Burn Injury: First Degree Burns CHARACTERISTICS • Abnormal redness of the skin Hair Folicle • Involves only the epidermis (first layer of Sweat Gland Burn skin) Depth Skin Layer 1° Epidermis • No blistering • Mild total body effects 2° • Heals in 3 to 4 days Dermis 3° Subcutaneous 4° Tissue (FAT) Muscle Second Degree Burns CHARACTERISTICS Superficial Partial Thickness • Papillary dermis (upper portion of the second layer of skin) Hair Folicle – Affects the first layer of skin and the top Sweat Gland Burn of the second layer of skin Depth Skin Layer 1° Epidermis • Blister formation • Burn appears pink and moist 2° • Painful, very sensitive Dermis • Turns white to the touch 3° Subcutaneous • Hair usually intact 4° Tissue (FAT) Muscle • Doesn’t scar–change in skin color Second Degree Burns CHARACTERISTICS Deep Partial Thickness • Reticular dermis (lower portion of second layer of skin) Hair Folicle – Involving tissue layers underneath Sweat Gland Burn Depth Skin Layer top skin layers 1° Epidermis • Healing process more than 3 weeks • Spotted red and white 2° Dermis • Decreased pain • Doesn’t turn white to the touch 3° Subcutaneous • Hairs pluck out easily 4° Tissue (FAT) Muscle • Scarring increases • May require surgical cleaning or grafting Third & Fourth Degree Burns CHARACTERISTICS Full Thickness • Burn is into fat or deeper • Area is red, white, brown or black Hair Folicle • Not painful Sweat Gland Burn Depth Skin Layer • Area is dry or leathery 1° Epidermis • Doesn’t turn white to the touch • Heals only from the edges 2° Dermis • Almost always requires surgery 3° Subcutaneous 4° Tissue (FAT) Muscle.