Emanuel Syndrome: a Rare Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Case Study of Distinctive Phenotypes Arising from Emanuel Syndrome in Two Karyotypically Identical Patients Mot Yee Yik1, Rabiatul Basria S.M.N
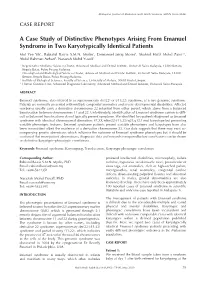
Malaysian Journal of Medicine and Health Sciences (eISSN 2636-9346) CASE REPORT A Case Study of Distinctive Phenotypes Arising From Emanuel Syndrome in Two Karyotypically Identical Patients Mot Yee Yik1, Rabiatul Basria S.M.N. Mydin2, Emmanuel Jairaj Moses1, Shahrul Hafiz Mohd Zaini2,3, Abdul Rahman Azhari4, Narazah Mohd Yusoff1 1 Regenerative Medicine Sciences Cluster, Advanced Medical and Dental Institute, Universiti Sains Malaysia, 13200 Bertam, Kepala Batas, Pulau Pinang Malaysia 2 Oncological and Radiological Sciences Cluster, Advanced Medical and Dental Institute, Universiti Sains Malaysia, 13200 Bertam, Kepala Batas, Pulau Pinang Malaysia, 3 Institute of Biological Sciences, Faculty of Science, University of Malaya, 50603 Kuala Lumpur. 4 Human Genetics Unit, Advanced Diagnostic Laboratory, Advanced Medical and Dental Institute, Universiti Sains Malaysia ABSTRACT Emanuel syndrome, also referred to as supernumerary der(22) or t(11;22) syndrome, is a rare genomic syndrome. Patients are normally presented with multiple congenital anomalies and severe developmental disabilities. Affected newborns usually carry a derivative chromosome 22 inherited from either parent, which stems from a balanced translocation between chromosomes 11 and 22. Unfortunately, identification of Emanuel syndrome carriers is diffi- cult as balanced translocations do not typically present symptoms. We identified two patients diagnosed as Emanuel syndrome with identical chromosomal aberration: 47,XX,+der(22)t(11;22)(q24;q12.1)mat karyotype but presenting variable phenotypic features. Emanuel syndrome patients present variable phenotypes and karyotypes have also been inconsistent albeit the existence of a derivative chromosome 22. Our data suggests that there may exist ac- companying genetic aberrations which influence the outcome of Emanuel syndrome phenotypes but it should be cautioned that more patient observations, diagnostic data and research is required before conclusions can be drawn on definitive karyotypic-phenotypic correlations. -

18 (2), 2015 77-82 a Case with Emanuel Syndrome
18 (2), 2015 l 77-82 DOI: 10.1515/bjmg-2015-0089 CASE REPORT A CASE WITH EMANUEL SYNDROME: EXTRA DERIVATIVE 22 CHROMOSOME INHERITED FROM THE MOTHER İkbal Atli E*, Gürkan H, Vatansever Ü, Ulusal S, Tozkir H *Corresponding Author: Emine İkbal Atli, Ph.D., Department of Medical Genetics, Faculty of Medicine, Trakya University, Campus Of Balkan, D100 Street, Edirne 22030, Turkey. Tel: +90-554-253-4030. Fax: +90- 284-223-4201. E-mail: [email protected] ABSTRACT INTRODUCTION Emanuel syndrome (ES) is a rare chromosomal Emanuel syndrome (ES) is an unbalanced disorder that is characterized by multiple congenital translocation syndrome, usually arising through a anomalies and developmental disabilities. Affected 3:1 meiosis I malsegregation during gametogenesis children are usually identified in the newborn period in a phenotypically balanced translocation normal as the offspring of balanced (11;22) translocation carrier. While the true mortality rate in Emanuel syn- carriers. Carriers of this balanced translocation usu- drome is unknown, long-term survival is possible [1]. ally have no clinical symptoms and are often identi- Emanuel syndrome is also referred to as derivative fied after the birth of offspring with an unbalanced 22 syndrome, derivative 11;22 syndrome, partial tri- form of the translocation, the supernumerary der(22) somy 11;22, or supernumerary der(22)t(11;22) syn- t(11;22) syndrome. We report a 3-year-old boy with drome [2]. In this partial duplication, 11(q23-qter) the t(11;22)(q23;q11) chromosome, transmitted in and 22(pter-q11) complex, congenital diaphragmatic an unbalanced fashion from his mother. -

Updates on Myopia
Updates on Myopia A Clinical Perspective Marcus Ang Tien Y. Wong Editors Updates on Myopia Marcus Ang • Tien Y. Wong Editors Updates on Myopia A Clinical Perspective Editors Marcus Ang Tien Y. Wong Singapore National Eye Center Singapore National Eye Center Duke-NUS Medical School Duke-NUS Medical School National University of Singapore National University of Singapore Singapore Singapore This book is an open access publication. ISBN 978-981-13-8490-5 ISBN 978-981-13-8491-2 (eBook) https://doi.org/10.1007/978-981-13-8491-2 © The Editor(s) (if applicable) and The Author(s) 2020, corrected publication 2020 Open Access This book is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made. The images or other third party material in this book are included in the book's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the book's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specifc statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. -
Research Institute Annual Report 2005
Research Annual Report 2005 The Joseph Stokes Jr. Research Institute of The Children’s Hospital of Philadelphia Embarking on a New Era ely to children is founded b xclusiv y Dr. F ted e ranc dica is W de . Le ital wi sp s, w ho it st h fir H ’s ew n so tio n na B ac he h T e an — d 5 5 R 8 .A 1 .F . P e n r o s e “... very large numbers of specialties moved towards the solution of each individual patient’s problem through highly diversified laboratory and clinical research.” - Joseph Stokes Jr., M.D., 1967 CONTENTS PURSUING RESEARCH PREEMINENCE 2 PROGRESS NOTES 30 SUPPORTING RESEARCH - STOKES CORE FACILITIES 40 INNOVATION FUELING PROGRESS 46 BUILDING THE INTELLECTUAL COMMUNITY 52 ADMINISTRATIVE ENHANCEMENTS 80 FINANCIAL/AWARD INFORMATION 84 WHO'S WHO AT STOKES 87 It is with great enthusiasm that we introduce the premier annual report for the Joseph Stokes Jr. Research Institute of The Children’s Hospital of Philadelphia. Stokes Institute has a rich and distinguished “bench to bedside” research history. The Institute serves as the home for more than 250 world-class investigators conducting innovative research in the laboratories and clinics across our campus. And, as you will see within the pages of this report, our investigators continue to advance the basic understanding of pediatric diseases and to develop new therapies that will benefit our patients and their families for generations to come. We’ve witnessed substantial growth in the Hospital’s research program over the last decade. -

Optical Genome Mapping As a Next-Generation
medRxiv preprint doi: https://doi.org/10.1101/2021.02.19.21251714; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Optical genome mapping as a next-generation cytogenomic tool for detection of structural and copy number variations for prenatal genomic analyses Nikhil Shri Sahajpal1#, Hayk Barseghyan2,3,4#, Ravindra Kolhe1, Alex Hastie4, Alka Chaubey1,4* 1Department of Pathology, Augusta University, Augusta, GA, USA 2Center for Genetic Medicine Research, Children’s National Hospital, Washington, DC, USA 3Genomics and Precision Medicine, School of Medicine and Health Sciences, George Washington University Washington, DC, USA 4Bionano Genomics Inc., San Diego, CA, USA # Equal contribution authors * Corresponding author: Alka Chaubey, PhD, FACMG Chief Medical Officer Bionano Genomics, Inc. 9540 Towne Centre Drive, Suite 100 San Diego, CA 92121 E: [email protected] C: (858) 337-2120 NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. medRxiv preprint doi: https://doi.org/10.1101/2021.02.19.21251714; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Abstract Global medical associations (ACOG, ISUOG, ACMG) recommend diagnostic prenatal testing for the detection and prevention of genetic disorders. -

2015-2020 Consolidated Plan for Washington County and the Cities of Beaverton and Hillsboro
Volume 2 2015-2020 Consolidated Plan for Washington County and the Cities of Beaverton and Hillsboro Cover photos of 2010-2015 CDBG and HOME projects: (Clockwise from the top left): City of North Plains Claxtar St. Waterline, Street and Sidewalk Improvements City of Hillsboro Walnut Park Improvements Northwest Housing Alternatives Alma Gardens Apartments, Hillsboro City of Hillsboro Dairy Creek Park Picnic Shelters and Accessibility Improvements WaCo LUT SW 173rd Sidewalk Improvements, Aloha City of Tualatin’s Juanita Pohl Center Centro Cultural de Washington County, Cornelius Bienestar, Inc.’s Juniper Gardens Apartments, Forest Grove Public Service activities funded by the City of Beaverton Home assisted by WaCo Office of Community Development’s Housing Rehabilitation Program Boys and Girls Aid Transitional Living Program, Beaverton Sequoia Mental Health Services Clinical Office Building (adjacent to Spruce Place Apartments) Copies of this document may be accessed online at: http://www.co.washington.or.us/CommunityDevelopment/Planning/2015-2020-consolidated-plan.cfm Approved by Washington County Board of Commissioners May 5, 2015 Minute Order #15-127 2015-2020 Consolidated Plan Volume 2 Washington County Consortium Washington County and The Cities of Beaverton and Hillsboro Oregon Prepared by Washington County Office of Community Development In collaboration with City of Beaverton Community Development Division and City of Hillsboro Planning Department Washington County 2015-2020 Consolidated Plan Volume 2 TABLE OF CONTENTS APPENDIX A: Supplementary Information for Introduction A.1 2010-2015 Consolidated Plan Objectives, Goals and Accomplishments ............................ 1 APPENDIX B: Supplementary Information for Chapter 2 Introductory Materials B.1 Citizen Participation Plan .................................................................................................... 3 B.2 Overview of the Con Plan Work Group ........................................................................... -

Case Report Chromosomal Abnormalities in Syndromic Orofacial Clefts: Report of Three Children
Hindawi Case Reports in Genetics Volume 2018, Article ID 1928918, 5 pages https://doi.org/10.1155/2018/1928918 Case Report Chromosomal Abnormalities in Syndromic Orofacial Clefts: Report of Three Children Rathika Damodara Shenoy ,1 Vijaya Shenoy,1 and Vikram Shetty2 1 DepartmentofPediatrics,K.S.HegdeMedicalAcademy,Nitte(DeemedtobeUniversity),Karnataka,India 2Nitte Meenakshi Institute of Craniofacial Surgery, Nitte (Deemed to be University), Karnataka, India Correspondence should be addressed to Rathika Damodara Shenoy; [email protected] Received 15 March 2018; Revised 1 August 2018; Accepted 27 August 2018; Published 9 September 2018 Academic Editor: Silvia Paracchini Copyright © 2018 Rathika Damodara Shenoy et al. Tis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Tis case series of three children reports clinical features and chromosomal abnormalities seen in a craniofacial clinic. All presented with orofacial clef, developmental or intellectual disability, and dysmorphism. Emanuel syndrome or supernumerary der (22)t(11; 22), the prototype of complex small supernumerary marker disorders, was seen in one child. Duplication 4q27q35.2 with concomitant deletion 21q22.2q22.3 and duplication 12p13.33p13.32 with concomitant deletion 18q22.3q23 seen in the remaining two children are not reported in literature. Maternal balanced translocation was established in both of these children. 1. Introduction 2. Methods Orofacial clef (OFC) is a common congenital anomaly with Genomic DNA was extracted from whole blood treated a prevalence of 1 in 600 live-births. It includes clef lip, clef with EDTA by standard protocol using protein precipitation lip with palate (CLP), and clef palate (CP). -

Next Generation Phenotyping in Emanuel and Pallister Killian
Received: 28 April 2017 Revised and accepted: 22 June 2017 DOI: 10.1111/cge.13087 SHORT REPORT Next generation phenotyping in Emanuel and Pallister-Killian syndrome using computer-aided facial dysmorphology analysis of 2D photos T. Liehr1 | N. Acquarola2 | K. Pyle1 | S. St-Pierre3 | M. Rinholm4 | O. Bar5 | K. Wilhelm1 | I. Schreyer1,6 1Jena University Hospital, Friedrich Schiller University, Institute of Human Genetics, Jena, High throughput approaches are continuously progressing and have become a major part of Germany clinical diagnostics. Still, the critical process of detailed phenotyping and gathering clinical infor- 2Pallister-Killian Syndrome Foundation of mation has not changed much in the last decades. Forms of next generation phenotyping Australia, Myaree, Australia (NGP) are needed to increase further the value of any kind of genetic approaches, including 3 Chromosome 22 Central, Timmins, Canada timely consideration of (molecular) cytogenetics during the diagnostic quest. As NGP we used 4 Chromosome 22 Central, Fuquay-Varina, in this study the facial dysmorphology novel analysis (FDNA) technology to automatically iden- North Carolina tify facial phenotypes associated with Emanuel (ES) and Pallister-Killian Syndrome (PKS) from 5FDNA Inc., Boston, Massachusetts 2D facial photos. The comparison between ES or PKS and normal individuals expressed a full 6Center for Ambulant Medicine, Human Genetics, Jena, Germany separation between the cohorts. Our results show that NPG is able to help in the clinic, and Correspondence could reduce the time patients spend in diagnostic odyssey. It also helps to differentiate ES or Dr Thomas Liehr, Institut für Humangenetik, PKS from each other and other patients with small supernumerary marker chromosomes, espe- Postfach, D-07740 Jena, Germany. -

The Genetics of Myopia 5 Milly S
The Genetics of Myopia 5 Milly S. Tedja, Annechien E. G. Haarman, Magda A. Meester-Smoor, Virginie J. M. Verhoeven, Caroline C. W. Klaver, and Stuart MacGregor Key Points • While the recent global rise of myopia prevalence is primarily attributable to environmental changes, within populations inherited factors play a large role in explaining why some individuals are affected by myopia while oth- ers are not. • Early efforts to identify the specific genes underlying the heritability of refractive error used linkage and candidate gene designs to identify up to 50 loci and genes, although most remain unconfirmed. M. S. Tedja · A. E. G. Haarman · M. A. Meester-Smoor Department of Ophthalmology, Erasmus Medical Center, Rotterdam, The Netherlands Department of Epidemiology, Erasmus Medical Center, Rotterdam, The Netherlands V. J. M. Verhoeven Department of Ophthalmology, Erasmus Medical Center, Rotterdam, The Netherlands Department of Epidemiology, Erasmus Medical Center, Rotterdam, The Netherlands Department of Clinical Genetics, Erasmus Medical Center, Rotterdam, The Netherlands C. C. W. Klaver Department of Ophthalmology, Erasmus Medical Center, Rotterdam, The Netherlands Department of Epidemiology, Erasmus Medical Center, Rotterdam, The Netherlands Department of Ophthalmology, Radboud University Medical Center, Nijmegen, The Netherlands S. MacGregor (*) Statistical Genetics, QIMR Berghofer Medical Research Institute, Brisbane, QLD, Australia e-mail: [email protected] © The Author(s) 2020 95 M. Ang, T. Y. Wong (eds.), Updates on Myopia, https://doi.org/10.1007/978-981-13-8491-2_5 96 M. S. Tedja et al. • As the sample size in genome-wide association studies (GWAS) has increased, the number of implicated loci has risen steadily, with 161 vari- ants reported in the latest meta-analysis. -

Artificial Intelligence (AI) in Rare Diseases
G C A T T A C G G C A T genes Review Artificial Intelligence (AI) in Rare Diseases: Is the Future Brighter? 1,2 1,2,3, 1,2,3, 1,2, Sandra Brasil , Carlota Pascoal y , Rita Francisco y, Vanessa dos Reis Ferreira *, Paula A. Videira 1,2,3 and Gonçalo Valadão 4,5,6 1 Portuguese Association for CDG, 2820-381 Lisboa, Portugal; [email protected] (S.B.); [email protected] (C.P.); [email protected] (R.F.); [email protected] (P.A.V.) 2 CDG & Allies—Professionals and Patient Associations International Network (CDG & Allies—PPAIN), Faculdade de Ciências e Tecnologia, Universidade NOVA de Lisboa, 2829-516 Lisboa, Portugal 3 UCIBIO, Departamento Ciências da Vida, Faculdade de Ciências e Tecnologia, Universidade NOVA de Lisboa, 2829-516 Lisboa, Portugal 4 Instituto de Telecomunicações, 1049-001 Lisboa, Portugal; [email protected] 5 Departamento de Ciências e Tecnologias, Autónoma Techlab–Universidade Autónoma de Lisboa, 1169-023 Lisboa, Portugal 6 Electronics, Telecommunications and Computers Engineering Department, Instituto Superior de Engenharia de Lisboa, 1959-007 Lisboa, Portugal * Correspondence: [email protected] Authors contributed equally. y Received: 30 September 2019; Accepted: 20 November 2019; Published: 27 November 2019 Abstract: The amount of data collected and managed in (bio)medicine is ever-increasing. Thus, there is a need to rapidly and efficiently collect, analyze, and characterize all this information. Artificial intelligence (AI), with an emphasis on deep learning, holds great promise in this area and is already being successfully applied to basic research, diagnosis, drug discovery, and clinical trials. -

Emanuel Syndrome Information
CHROMOSOME DISORDER OUTREACH EMANUEL SYNDROME INFORMATION Emanuel Syndrome All chromosomal syndromes are caused by deletions (duplications, trisomies) of one chromosome. The only exception is Emanuel syndrome (ES), caused by the cumulative action of partial trisomies for two chromosomes: the distal segment of chromosome 11q and the proximal segment of chromosome 22q. Most non-Robertsonian translocations are unique. Translocation t(11;22) is an exception. It is the most common non-Robertsonian translocation in humans. The structural similarity of the 22q11.2 segment and the 11q23 segment facilitates the exchange between these areas with formation of t(11;22)(q23; q11.2). As a result of the segregation 3:1 which is almost constant in this translocation1 the patient will have an additional chromosome der(22) which includes part of chromosome 22 (short arm, centromere and proximal segment of 11q [up to 22q11.2]) and the distal part of chromosome 11 (from 11q23 to the end of the long arm). This syndrome is usually called Emanuel syndrome after Beverly Emanuel who studied this condition for many years2. There is no doubt that several patients described in the early cytogenetic literature as persons with “trisomy 22” actually had ES. Sometimes the term “supernumerary der(22)t(11;22)” syndrome is used to describe this disorder3. page 1 ES is a relatively common pathology. At least 400 patients have been reported so far. The clinical manifestations of the syndrome include severe developmental delay, defects of the face, heart, kidneys and other systems. Most patients have prenatal hypoplasia and their physical parameters (weight, height) are much below those of their healthy peers. -

Emanuel Syndrome
Emanuel syndrome rarechromo.org Your child will bring you joy and pain, just as all children do. Rejoice in the small achievements. Most of what I have found out about Emanuel syndrome has been from my internet research. Why is it called Emanuel syndrome? Emanuel syndrome is named after Dr Beverly Emanuel, a cytogeneticist in Philadelphia, USA. In 2004, founding members of Chromosome 22 Central, an online parent support group for chromosome 22 disorders, successfully lobbied to have this name applied to the condition caused by having an extra chromosome called ‘derivative 22’. Dr Emanuel is recognised for her laboratory’s work on identifying the source of the derivative 22, how it is inherited, and for her association with the parent support group. However, the condition is so rare that many doctors may not have heard of it called by this name. Other names In the scientific literature, the name Emanuel syndrome is only starting to be used. Previously it has been referred to as derivative 22 syndrome, derivative 11;22 syndrome or partial trisomy 11;22. These names describe the fact that there are 47, instead of the usual 46, chromosomes present in the cells of the child’s body. The very early literature refers to the condition as trisomy 22 based on the incorrect assumption that the extra chromosome was a third 22 (hence the name trisomy). The extra chromosome is made up of the top and middle part of chromosome 22 and the bottom part of chromosome 11 (see diagram, left). This means that there are extra copies of many genes present on both chromosome 22 and 11.