Emanuel Syndrome Information
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
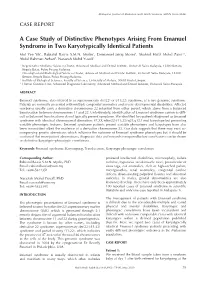
A Case Study of Distinctive Phenotypes Arising from Emanuel Syndrome in Two Karyotypically Identical Patients Mot Yee Yik1, Rabiatul Basria S.M.N
Malaysian Journal of Medicine and Health Sciences (eISSN 2636-9346) CASE REPORT A Case Study of Distinctive Phenotypes Arising From Emanuel Syndrome in Two Karyotypically Identical Patients Mot Yee Yik1, Rabiatul Basria S.M.N. Mydin2, Emmanuel Jairaj Moses1, Shahrul Hafiz Mohd Zaini2,3, Abdul Rahman Azhari4, Narazah Mohd Yusoff1 1 Regenerative Medicine Sciences Cluster, Advanced Medical and Dental Institute, Universiti Sains Malaysia, 13200 Bertam, Kepala Batas, Pulau Pinang Malaysia 2 Oncological and Radiological Sciences Cluster, Advanced Medical and Dental Institute, Universiti Sains Malaysia, 13200 Bertam, Kepala Batas, Pulau Pinang Malaysia, 3 Institute of Biological Sciences, Faculty of Science, University of Malaya, 50603 Kuala Lumpur. 4 Human Genetics Unit, Advanced Diagnostic Laboratory, Advanced Medical and Dental Institute, Universiti Sains Malaysia ABSTRACT Emanuel syndrome, also referred to as supernumerary der(22) or t(11;22) syndrome, is a rare genomic syndrome. Patients are normally presented with multiple congenital anomalies and severe developmental disabilities. Affected newborns usually carry a derivative chromosome 22 inherited from either parent, which stems from a balanced translocation between chromosomes 11 and 22. Unfortunately, identification of Emanuel syndrome carriers is diffi- cult as balanced translocations do not typically present symptoms. We identified two patients diagnosed as Emanuel syndrome with identical chromosomal aberration: 47,XX,+der(22)t(11;22)(q24;q12.1)mat karyotype but presenting variable phenotypic features. Emanuel syndrome patients present variable phenotypes and karyotypes have also been inconsistent albeit the existence of a derivative chromosome 22. Our data suggests that there may exist ac- companying genetic aberrations which influence the outcome of Emanuel syndrome phenotypes but it should be cautioned that more patient observations, diagnostic data and research is required before conclusions can be drawn on definitive karyotypic-phenotypic correlations. -

18 (2), 2015 77-82 a Case with Emanuel Syndrome
18 (2), 2015 l 77-82 DOI: 10.1515/bjmg-2015-0089 CASE REPORT A CASE WITH EMANUEL SYNDROME: EXTRA DERIVATIVE 22 CHROMOSOME INHERITED FROM THE MOTHER İkbal Atli E*, Gürkan H, Vatansever Ü, Ulusal S, Tozkir H *Corresponding Author: Emine İkbal Atli, Ph.D., Department of Medical Genetics, Faculty of Medicine, Trakya University, Campus Of Balkan, D100 Street, Edirne 22030, Turkey. Tel: +90-554-253-4030. Fax: +90- 284-223-4201. E-mail: [email protected] ABSTRACT INTRODUCTION Emanuel syndrome (ES) is a rare chromosomal Emanuel syndrome (ES) is an unbalanced disorder that is characterized by multiple congenital translocation syndrome, usually arising through a anomalies and developmental disabilities. Affected 3:1 meiosis I malsegregation during gametogenesis children are usually identified in the newborn period in a phenotypically balanced translocation normal as the offspring of balanced (11;22) translocation carrier. While the true mortality rate in Emanuel syn- carriers. Carriers of this balanced translocation usu- drome is unknown, long-term survival is possible [1]. ally have no clinical symptoms and are often identi- Emanuel syndrome is also referred to as derivative fied after the birth of offspring with an unbalanced 22 syndrome, derivative 11;22 syndrome, partial tri- form of the translocation, the supernumerary der(22) somy 11;22, or supernumerary der(22)t(11;22) syn- t(11;22) syndrome. We report a 3-year-old boy with drome [2]. In this partial duplication, 11(q23-qter) the t(11;22)(q23;q11) chromosome, transmitted in and 22(pter-q11) complex, congenital diaphragmatic an unbalanced fashion from his mother. -

Crouzon Syndrome with Ophthalmological Complications
Journal of Rawalpindi Medical College (JRMC); 2012;16(1):80-81 Case Report Crouzon Syndrome With Ophthalmological Complications Rahela Nasir Paediatric Department, Capital Hospital, CDA Islamabad. Crouzon Syndrome is characterized by premature bilateral optic atrophy. Other facial features included a craniosynostosis. It has an autosomal dominant inheritance prominent nose and deep and narrow palate. No but represents fresh mutation also. Other craniofacial digital abnormalities were seen. No dental aplasia was abnormalities include ocular proptosis caused by shallow present. Systemic examination revealed no orbits with or without divergent strabismus. There may be abnormality. increased intracranial pressure for which surgical morcellation procedures are indicated. A case of He was diagnosed as a case of Crouzon syndrome craniosynostosis is reported which is diagnosed as Crouzon with ocular complications on clinical basis. He was Syndrome with ocular complications on clinical grounds. investigated for microcephaly and suspected Split craniotomy was performed by a neurosurgeon to craniosynostosis. Radiographs of skull showed small relieve raised intracranial pressure and to enhance brain sized skull with early closure of sutures and fontanelle growth. Crouzon Syndrome was originally described in 1912 suggestive of craniosynstosis(Fig 2). A hammered- by Crouzon in a mother and her daughter. It is an autosomal silver (beaten metal/ copper beaten) appearance was dominant inherited disorder but represents fresh mutation also seen due to raised intracranial pressure and also. Crouzon syndrome is characterized by premature compression of the developing brain on the fused craniosynostosis which is quite variable but the coronal suture is nearly always bilaterally involved. Craniofacial bone. CT scan brain with contrast was done which abnormalities include brachycephaly, shallow orbits and confirmed the features suggestive of craniosynostosis maxillary hypoplasia. -

Updates on Myopia
Updates on Myopia A Clinical Perspective Marcus Ang Tien Y. Wong Editors Updates on Myopia Marcus Ang • Tien Y. Wong Editors Updates on Myopia A Clinical Perspective Editors Marcus Ang Tien Y. Wong Singapore National Eye Center Singapore National Eye Center Duke-NUS Medical School Duke-NUS Medical School National University of Singapore National University of Singapore Singapore Singapore This book is an open access publication. ISBN 978-981-13-8490-5 ISBN 978-981-13-8491-2 (eBook) https://doi.org/10.1007/978-981-13-8491-2 © The Editor(s) (if applicable) and The Author(s) 2020, corrected publication 2020 Open Access This book is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made. The images or other third party material in this book are included in the book's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the book's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specifc statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. -

Macrocephaly Information Sheet 6-13-19
Next Generation Sequencing Panel for Macrocephaly Clinical Features: Macrocephaly refers to an abnormally large head, OFC greater than 98th percentile, inclusive of the scalp, cranial bone and intracranial contents. Megalencephaly, brain weight/volume ratio greater than 98th percentile, results from true enlargement of the brain parenchyma [1]. Megalencephaly is typically accompanied by macrocephaly, however macrocephaly can occur in the absence of megalencephaly [2]. Both macrocephaly and megalencephaly can been seen as isolated clinical findings as well as clinical features of a mutli-systemic syndromic diagnosis. Our Macrocephaly Panel includes analysis of the 36 genes listed below. Macrocephaly Sequencing Panel ASXL2 GLI3 MTOR PPP2R5D TCF20 BRWD3 GPC3 NFIA PTEN TBC1D7 CHD4 HEPACAM NFIX RAB39B UPF3B CHD8 HERC1 NONO RIN2 ZBTB20 CUL4B KPTN NSD1 RNF125 DNMT3A MED12 OFD1 RNF135 EED MITF PIGA SEC23B EZH2 MLC1 PPP1CB SETD2 Gene Clinical Features Details ASXL2 Shashi-Pena Shashi et al. (2016) found that six patients with developmental delay, syndrome macrocephaly, and dysmorphic features were found to have de novo truncating variants in ASXL2 [3]. Distinguishing features were macrocephaly, absence of growth retardation, and variability in the degree of intellectual disabilities The phenotype also consisted of prominent eyes, arched eyebrows, hypertelorism, a glabellar nevus flammeus, neonatal feeding difficulties and hypotonia. BRWD3 X-linked intellectual Truncating mutations in the BRWD3 gene have been described in males with disability nonsyndromic intellectual disability and macrocephaly [4]. Other features include a prominent forehead and large cupped ears. CHD4 Sifrim-Hitz-Weiss Weiss et al., 2016, identified five individuals with de novo missense variants in the syndrome CHD4 gene with intellectual disabilities and distinctive facial dysmorphisms [5]. -
Research Institute Annual Report 2005
Research Annual Report 2005 The Joseph Stokes Jr. Research Institute of The Children’s Hospital of Philadelphia Embarking on a New Era ely to children is founded b xclusiv y Dr. F ted e ranc dica is W de . Le ital wi sp s, w ho it st h fir H ’s ew n so tio n na B ac he h T e an — d 5 5 R 8 .A 1 .F . P e n r o s e “... very large numbers of specialties moved towards the solution of each individual patient’s problem through highly diversified laboratory and clinical research.” - Joseph Stokes Jr., M.D., 1967 CONTENTS PURSUING RESEARCH PREEMINENCE 2 PROGRESS NOTES 30 SUPPORTING RESEARCH - STOKES CORE FACILITIES 40 INNOVATION FUELING PROGRESS 46 BUILDING THE INTELLECTUAL COMMUNITY 52 ADMINISTRATIVE ENHANCEMENTS 80 FINANCIAL/AWARD INFORMATION 84 WHO'S WHO AT STOKES 87 It is with great enthusiasm that we introduce the premier annual report for the Joseph Stokes Jr. Research Institute of The Children’s Hospital of Philadelphia. Stokes Institute has a rich and distinguished “bench to bedside” research history. The Institute serves as the home for more than 250 world-class investigators conducting innovative research in the laboratories and clinics across our campus. And, as you will see within the pages of this report, our investigators continue to advance the basic understanding of pediatric diseases and to develop new therapies that will benefit our patients and their families for generations to come. We’ve witnessed substantial growth in the Hospital’s research program over the last decade. -

Optical Genome Mapping As a Next-Generation
medRxiv preprint doi: https://doi.org/10.1101/2021.02.19.21251714; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Optical genome mapping as a next-generation cytogenomic tool for detection of structural and copy number variations for prenatal genomic analyses Nikhil Shri Sahajpal1#, Hayk Barseghyan2,3,4#, Ravindra Kolhe1, Alex Hastie4, Alka Chaubey1,4* 1Department of Pathology, Augusta University, Augusta, GA, USA 2Center for Genetic Medicine Research, Children’s National Hospital, Washington, DC, USA 3Genomics and Precision Medicine, School of Medicine and Health Sciences, George Washington University Washington, DC, USA 4Bionano Genomics Inc., San Diego, CA, USA # Equal contribution authors * Corresponding author: Alka Chaubey, PhD, FACMG Chief Medical Officer Bionano Genomics, Inc. 9540 Towne Centre Drive, Suite 100 San Diego, CA 92121 E: [email protected] C: (858) 337-2120 NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. medRxiv preprint doi: https://doi.org/10.1101/2021.02.19.21251714; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Abstract Global medical associations (ACOG, ISUOG, ACMG) recommend diagnostic prenatal testing for the detection and prevention of genetic disorders. -

2015-2020 Consolidated Plan for Washington County and the Cities of Beaverton and Hillsboro
Volume 2 2015-2020 Consolidated Plan for Washington County and the Cities of Beaverton and Hillsboro Cover photos of 2010-2015 CDBG and HOME projects: (Clockwise from the top left): City of North Plains Claxtar St. Waterline, Street and Sidewalk Improvements City of Hillsboro Walnut Park Improvements Northwest Housing Alternatives Alma Gardens Apartments, Hillsboro City of Hillsboro Dairy Creek Park Picnic Shelters and Accessibility Improvements WaCo LUT SW 173rd Sidewalk Improvements, Aloha City of Tualatin’s Juanita Pohl Center Centro Cultural de Washington County, Cornelius Bienestar, Inc.’s Juniper Gardens Apartments, Forest Grove Public Service activities funded by the City of Beaverton Home assisted by WaCo Office of Community Development’s Housing Rehabilitation Program Boys and Girls Aid Transitional Living Program, Beaverton Sequoia Mental Health Services Clinical Office Building (adjacent to Spruce Place Apartments) Copies of this document may be accessed online at: http://www.co.washington.or.us/CommunityDevelopment/Planning/2015-2020-consolidated-plan.cfm Approved by Washington County Board of Commissioners May 5, 2015 Minute Order #15-127 2015-2020 Consolidated Plan Volume 2 Washington County Consortium Washington County and The Cities of Beaverton and Hillsboro Oregon Prepared by Washington County Office of Community Development In collaboration with City of Beaverton Community Development Division and City of Hillsboro Planning Department Washington County 2015-2020 Consolidated Plan Volume 2 TABLE OF CONTENTS APPENDIX A: Supplementary Information for Introduction A.1 2010-2015 Consolidated Plan Objectives, Goals and Accomplishments ............................ 1 APPENDIX B: Supplementary Information for Chapter 2 Introductory Materials B.1 Citizen Participation Plan .................................................................................................... 3 B.2 Overview of the Con Plan Work Group ........................................................................... -

Sotos Syndrome
European Journal of Human Genetics (2007) 15, 264–271 & 2007 Nature Publishing Group All rights reserved 1018-4813/07 $30.00 www.nature.com/ejhg PRACTICAL GENETICS In association with Sotos syndrome Sotos syndrome is an autosomal dominant condition characterised by a distinctive facial appearance, learning disability and overgrowth resulting in tall stature and macrocephaly. In 2002, Sotos syndrome was shown to be caused by mutations and deletions of NSD1, which encodes a histone methyltransferase implicated in chromatin regulation. More recently, the NSD1 mutational spectrum has been defined, the phenotype of Sotos syndrome clarified and diagnostic and management guidelines developed. Introduction In brief Sotos syndrome was first described in 1964 by Juan Sotos Sotos syndrome is characterised by a distinctive facial and the major diagnostic criteria of a distinctive facial appearance, learning disability and childhood over- appearance, childhood overgrowth and learning disability growth. were established in 1994 by Cole and Hughes.1,2 In 2002, Sotos syndrome is associated with cardiac anomalies, cloning of the breakpoints of a de novo t(5;8)(q35;q24.1) renal anomalies, seizures and/or scoliosis in B25% of translocation in a child with Sotos syndrome led to the cases and a broad variety of additional features occur discovery that Sotos syndrome is caused by haploinsuffi- less frequently. ciency of the Nuclear receptor Set Domain containing NSD1 abnormalities, such as truncating mutations, protein 1 gene, NSD1.3 Subsequently, extensive analyses of missense mutations in functional domains, partial overgrowth cases have shown that intragenic NSD1 muta- gene deletions and 5q35 microdeletions encompass- tions and 5q35 microdeletions encompassing NSD1 cause ing NSD1, are identifiable in the majority (490%) of 490% of Sotos syndrome cases.4–10 In addition, NSD1 Sotos syndrome cases. -

KBG Syndrome Presenting with Brachydactyly Type E
Bone 123 (2019) 18–22 Contents lists available at ScienceDirect Bone journal homepage: www.elsevier.com/locate/bone Case Report KBG syndrome presenting with brachydactyly type E T ⁎ Renata Libiantoa,b,c, , Kathy HC Wud,e,f,g, Sophie Deveryd, John A Eismana,b,f,h, Jackie R Centera,b,f,h a Bone Division, Garvan Institute of Medical Research, Sydney, Australia b Department of Endocrinology, St Vincent's Hospital Sydney, Australia c Department of Medicine, The University of Melbourne, Australia d Clinical Genomics Unit, St Vincent's Hospital Sydney, Australia e Discipline of Genetic Medicine, University of Sydney, Australia f School of Medicine, UNSW, Sydney, Australia g Genomics and Epigenetics Division, Garvan Institute of Medical Research, Sydney, Australia h School of Medicine Sydney, University of Notre Dame, Australia ARTICLE INFO ABSTRACT Keywords: We report the case of a young woman who presented at age 10 years with height on the tenth centile, bra- KBG syndrome chydactyly type E and mild developmental delay. Biochemistry and hormonal profiles were normal. Differential ANKRD11 gene diagnoses considered included Albright hereditary osteodystrophy without hormone resistance (a.k.a pseu- Skeletal disorder dopseudohypoparathyroidism), 2q37 microdeletion syndrome and acrodysostosis. She had a normal karyotype Brachydactyly type E and normal FISH of 2q37. Whole genome sequencing (WGS) identified a mutation in the ANKRD11 gene as- sociated with KBG syndrome. We review the clinical features of the genetic syndromes considered, and suggest KBG syndrome be considered in patients presenting with syndromic brachydactyly type E, especially if short stature and developmental delay are also present. 1. Case support in a mainstream school for specific learning difficulties. -

Case Report Chromosomal Abnormalities in Syndromic Orofacial Clefts: Report of Three Children
Hindawi Case Reports in Genetics Volume 2018, Article ID 1928918, 5 pages https://doi.org/10.1155/2018/1928918 Case Report Chromosomal Abnormalities in Syndromic Orofacial Clefts: Report of Three Children Rathika Damodara Shenoy ,1 Vijaya Shenoy,1 and Vikram Shetty2 1 DepartmentofPediatrics,K.S.HegdeMedicalAcademy,Nitte(DeemedtobeUniversity),Karnataka,India 2Nitte Meenakshi Institute of Craniofacial Surgery, Nitte (Deemed to be University), Karnataka, India Correspondence should be addressed to Rathika Damodara Shenoy; [email protected] Received 15 March 2018; Revised 1 August 2018; Accepted 27 August 2018; Published 9 September 2018 Academic Editor: Silvia Paracchini Copyright © 2018 Rathika Damodara Shenoy et al. Tis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Tis case series of three children reports clinical features and chromosomal abnormalities seen in a craniofacial clinic. All presented with orofacial clef, developmental or intellectual disability, and dysmorphism. Emanuel syndrome or supernumerary der (22)t(11; 22), the prototype of complex small supernumerary marker disorders, was seen in one child. Duplication 4q27q35.2 with concomitant deletion 21q22.2q22.3 and duplication 12p13.33p13.32 with concomitant deletion 18q22.3q23 seen in the remaining two children are not reported in literature. Maternal balanced translocation was established in both of these children. 1. Introduction 2. Methods Orofacial clef (OFC) is a common congenital anomaly with Genomic DNA was extracted from whole blood treated a prevalence of 1 in 600 live-births. It includes clef lip, clef with EDTA by standard protocol using protein precipitation lip with palate (CLP), and clef palate (CP). -
Accelerating Matchmaking of Novel Dysmorphology Syndromes Through Clinical and Genomic Characterization of a Large Cohort
ORIGINAL RESEARCH ARTICLE © American College of Medical Genetics and Genomics Accelerating matchmaking of novel dysmorphology syndromes through clinical and genomic characterization of a large cohort Ranad Shaheen, PhD1, Nisha Patel, PhD1, Hanan Shamseldin, MSc1, Fatema Alzahrani, BSc1, Ruah Al-Yamany, MD1, Agaadir ALMoisheer, MSc1, Nour Ewida, BSc1, Shamsa Anazi, MSc1, Maha Alnemer, MD2, Mohamed Elsheikh, MD3, Khaled Alfaleh, MD3,4, Muneera Alshammari, MD4, Amal Alhashem, MD5, Abdullah A. Alangari, MD4, Mustafa A. Salih, MD4, Martin Kircher, MD6, Riza M. Daza, PhD6, Niema Ibrahim, BSc1, Salma M. Wakil, PhD1, Ahmed Alaqeel, MD7, Ikhlas Altowaijri, MD7, Jay Shendure, MD, PhD6, Amro Al-Habib, MD7, Eissa Faqieh, MD8 and Fowzan S. Alkuraya, MD1,9 Purpose: Dysmorphology syndromes are among the most common and C3ORF17). A significant minority of the phenotypes (6/31, 19%), referrals to clinical genetics specialists. Inability to match the dysmor- however, were caused by genes known to cause Mendelian pheno- phology pattern to a known syndrome can pose a major diagnostic chal- types, thus expanding the phenotypic spectrum of the diseases linked lenge. With an aim to accelerate the establishment of new syndromes to these genes. The conspicuous inheritance pattern and the highly and their genetic etiology, we describe our experience with multiplex specific phenotypes appear to have contributed to the high yield consanguineous families that appeared to represent novel autosomal (90%) of plausible molecular diagnoses in our study cohort. recessive dysmorphology syndromes at the time of evaluation. Conclusion: Reporting detailed clinical and genomic analysis of Methods: Combined autozygome/exome analysis of multiplex a large series of apparently novel dysmorphology syndromes will consanguineous families with apparently novel dysmorphology syn- likely lead to a trend to accelerate the establishment of novel syn- dromes.