Formaldehyde Test Kit Utility
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Formaldehyde May Be Found in Cosmetic Products Even When Unlabelled
Open Med. 2015; 10: 323-328 Research Article Open Access Laura Malinauskiene*, Audra Blaziene, Anzelika Chomiciene, Marléne Isaksson Formaldehyde may be found in cosmetic products even when unlabelled Abstract: Concomitant contact allergy to formaldehyde reliable method for detecting formaldehyde presence in and formaldehyde-releasers remains common among cosmetic products. patients with allergic contact dermatitis. Concentration of free formaldehyde in cosmetic products within allowed Keywords: chromotropic acid; formaldehyde; formalde- limits have been shown to induce dermatitis from short- hyde-releaser; high-performance liquid chromatography term use on normal skin. DOI 10.1515/med-2015-0047 The aim of this study was to investigate the formalde- Received: February 2, 2015; accepted: May 28, 2015 hyde content of cosmetic products made in Lithuania. 42 samples were analysed with the chromotropic acid (CA) method for semi-quantitative formaldehyde deter- mination. These included 24 leave-on (e.g., creams, 1 Introduction lotions) and 18 rinse-off (e.g., shampoos, soaps) products. Formaldehyde is a well-documented contact allergen. Formaldehyde releasers were declared on the labels of 10 Over recent decades, the prevalence of contact allergy to products. No formaldehyde releaser was declared on the formaldehyde has been found to be 8-9% in the USA and label of the only face cream investigated, but levels of free 2-3% in European countries [1]. formaldehyde with the CA method was >40 mg/ml and Formaldehyde as such is very seldomly used in cosmetic when analysed with a high-performance liquid chromato- products anymore, but preservatives releasing formalde- graphic method – 532 ppm. According to the EU Cosmetic hyde in the presence of water are widely used in many directive, if the concentration of formaldehyde is above cosmetic products (e.g., shampoos, creams, etc.), topical 0.05% a cosmetic product must be labelled “contains medications and household products (e.g., dishwashing formaldehyde“. -

Allergic Contact Dermatitis from Formaldehyde Exposure
DOI: 10.5272/jimab.2012184.255 Journal of IMAB - Annual Proceeding (Scientific Papers) 2012, vol. 18, book 4 ALLERGIC CONTACT DERMATITIS FROM FORMALDEHYDE EXPOSURE Maya Lyapina1, Angelina Kisselova-Yaneva 2, Assya Krasteva2, Mariana Tzekova -Yaneva2, Maria Dencheva-Garova2 1) Department of Hygiene, Medical Ecology and Nutrition, Medical Faculty, 2) Department of Oral and Image Diagnostic, Faculty of Dental Medicine, Medical University, Sofia,Bulgaria ABSTRACT atmospheric air, tobacco smoke, use of cosmetic products Formaldehyde is a ubiquitous chemical agent, a part and detergents, and in less extend – water and food of our outdoor and indoor working and residential consumption (11, 81). It is released into the atmosphere environment. Healthcare workers in difficult occupations are through fumes from automobile exhausts without catalytic among the most affected by formaldehyde exposure. convertors and by manufacturing facilities that burn fossil Formaldehyde is an ingredient of some dental materials. fuels in usual concentration about 1-10 ppb. Uncontrolled Formaldehyde is well-known mucous membrane irritant and forest fires and the open burning of waste also give off a primary skin sensitizing agent associated with both contact formaldehyde. It is believed that the daily exposure from dermatitis (Type IV allergy), and immediate, anaphylactic atmospheric air is up to 0.1 mg (35, 43, 44). reactions (Type I allergy). Inhalation exposure to According to the WHO industrial emissions could formaldehyde was identified as a potential cause of asthma. appear at each step of production, use, transportation, or Quite a few investigations are available concerning health deposition of formaldehyde-containing products. issues for dental students following formaldehyde exposure. Formaldehyde emissions are detected from various Such studies would be beneficial for early diagnosis of industries – energy industry, wood and paper product hypersensitivity, adequate prophylactic, risk assessment and industries, textile production and finishing, chemical management of their work. -

Nomination Background: N-(3-Chloroallyl)Hexaminium Chloride
• NATIONAL TOXICOLOGY PROGRAM EXECUTIVE SUMMARY OF SAFETY AND TOXICITY INFORMATION N-(3-CHLOROALLYL)HEXAMINIUM CHLORIDE CAS Number 4080-31-3 July 16, 1991 Submitted to: NATIONAL TOXICOLOGY PROGRAM Submitted by: Arthur D. Little, Inc. Chemical Evaluation Committee Draft Report • • TABLE OF CONTENTS Page L NOMINATION HISTORY AND REVIEW .................... 1 II. CHEMICAL AND PHYSICAL DATA ....................... 3 III. PRODUCTION/USE ................................... 5 IV. EXPOSURE/REGULATORY STATUS...................... .10 V. TOXICOLOGICAL EFFECTS ........................... .11 VI. STRUCTURE ACTIVITY RELATIONSHIPS ..................48 VII. REFERENCES ..................................... : . ......... 49 APPENDIX I, ON-LINE DATA BASES SEARCHED ............ .53 APPENDIX II, SAFETY INFORMATION.................... .54 1 ,, .• • • OVERVJEWl Nomination History: N-(3-Chloroallyl)hexaminium chloride was originally nominated for carcinogenicity testing by the National Cancer Institute (NCI) in 1980 with moderate priority. In March 1980, the Chemical Evaluation Committee (CEC) recommended carcinogenicity testing. Due to budgetary cutbacks in 1982, this compound was reevaluated and recommended for in vitro cytogenetics and chemical disposition testing by the CEC, and was selected for chemical disposition testing by the Executive Committee. The renomination of this chemical in 1984 by the NCI was based on potentialfor significant human exposure and concern that it may be carcinogenic due to structural considerations. This recent nomination was -

University of Groningen Formaldehyde-Releasers In
University of Groningen Formaldehyde-releasers in cosmetics de Groot, Anton C.; White, Ian R.; Flyvholm, Mari-Ann; Lensen, Gerda; Coenraads, Pieter- Jan Published in: CONTACT DERMATITIS IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2010 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): de Groot, A. C., White, I. R., Flyvholm, M-A., Lensen, G., & Coenraads, P-J. (2010). Formaldehyde- releasers in cosmetics: relationship to formaldehyde contact allergy Part 1. Characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. CONTACT DERMATITIS, 62(1), 18-31. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. -
Imidazolidine-Based Metal Carbene Metathesis
Europäisches Patentamt *EP001180108B1* (19) European Patent Office Office européen des brevets (11) EP 1 180 108 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.7: C07F 15/00 of the grant of the patent: 27.08.2003 Bulletin 2003/35 (86) International application number: PCT/US00/14048 (21) Application number: 00937665.8 (87) International publication number: (22) Date of filing: 22.05.2000 WO 00/071554 (30.11.2000 Gazette 2000/48) (54) IMIDAZOLIDINE-BASED METAL CARBENE METATHESIS CATALYSTS IMIDAZOLIDIN ENTHALTENDE METALLCARBEN-KATALYSATOREN FÜR DIE METATHESE CATALYSEURS DE METATHESE DE CARBENE METALLIQUE A BASE D’IMIDAZOLIDINE (84) Designated Contracting States: (56) References cited: AT BE CH CY DE DK ES FI FR GB GR IE IT LI LU US-A- 5 831 108 MC NL PT SE • CHEMICAL ABSTRACTS, vol. 131, no. 21, 22 (30) Priority: 24.05.1999 US 135493 P November 1999 Columbus, Ohio, US; abstract 07.07.1999 US 142853 P no. 285987k, SCHOLL, M. et al.: "Synthesis and Activity of a New Generation of (43) Date of publication of application: Ruthenium-Based Olefin Metathesis Catalysts 20.02.2002 Bulletin 2002/08 Coordinated with 1,3-Dimesityl-4,5- -dihydroimidazol-2-ylidene Ligands" column 1, (73) Proprietor: CALIFORNIA INSTITUTE OF XP002901392; & Org. Lett., vol. 1, no. 6, 1999, TECHNOLOGY pages Pasadena, California 91125 (US) • CHEMICAL ABSTRACTS, vol. 131, no. 22, 29 November 1999 Columbus, Ohio, US; abstract (72) Inventors: no. 299544a, WESKAMP, T.: "Highly active • GRUBBS, Robert, H. ruthenium catalysts for olefin metathesis: the South Pasadena, CA 91030 (US) synergy of N-Heterocyclic carbenes and • SCHOLL, Matthias coordinatively labile ligands" page 567; column Arcadia, CA 91006 (US) 1, XP002901393; & Angew. -

Safety Assessment of Imidazolidinyl Urea As Used in Cosmetics
Safety Assessment of Imidazolidinyl Urea as Used in Cosmetics Status: Re-Review for Panel Review Release Date: May 10, 2019 Panel Meeting Date: June 6-7, 2019 The 2019 Cosmetic Ingredient Review Expert Panel members are: Chair, Wilma F. Bergfeld, M.D., F.A.C.P.; Donald V. Belsito, M.D.; Ronald A. Hill, Ph.D.; Curtis D. Klaassen, Ph.D.; Daniel C. Liebler, Ph.D.; James G. Marks, Jr., M.D., Ronald C. Shank, Ph.D.; Thomas J. Slaga, Ph.D.; and Paul W. Snyder, D.V.M., Ph.D. The CIR Executive Director is Bart Heldreth, Ph.D. This safety assessment was prepared by Christina L. Burnett, Senior Scientific Analyst/Writer. © Cosmetic Ingredient Review 1620 L Street, NW, Suite 1200 ♢ Washington, DC 20036-4702 ♢ ph 202.331.0651 ♢ fax 202.331.0088 ♢ [email protected] Distributed for Comment Only -- Do Not Cite or Quote Commitment & Credibility since 1976 Memorandum To: CIR Expert Panel Members and Liaisons From: Christina Burnett, Senior Scientific Writer/Analyst Date: May 10, 2019 Subject: Re-Review of the Safety Assessment of Imidazolidinyl Urea Imidazolidinyl Urea was one of the first ingredients reviewed by the CIR Expert Panel, and the final safety assessment was published in 1980 with the conclusion “safe when incorporated in cosmetic products in amounts similar to those presently marketed” (imurea062019origrep). In 2001, after considering new studies and updated use data, the Panel determined to not re-open the safety assessment (imurea062019RR1sum). The minutes from the Panel deliberations of that re-review are included (imurea062019min_RR1). Minutes from the deliberations of the original review are unavailable. -
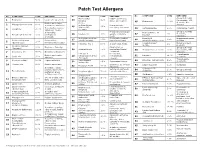
Patch Test Allergens
Patch Test Allergens No. COMPOUND CONC EXPOSURE No. COMPOUND CONC EXPOSURE No. COMPOUND CONC EXPOSURE Mixed dialkyl Rubber accelerator, Group B steroids: 1 Benzocaine 5.0% Local ester anesthetic 24 1.0% fluocinonide, TAC, thiourea assoc. w/ neoprene. 45 Budesonide 0.01% desonide. Also Rubber accelerator, Cl+Me- 2 Mercaptobenzothiazole 1.0% isothiazolinone Preservative in Group D. cutting oils, antifreeze 25 .01% In cosmetics, waxes, (Kathon CG, cosmetics, shampoos. Compositae mix 5.0% Compositae flowers. 3 Colophony 20.0% 46 adhesives. “Rosin.” 100ppm) Group D steroids: In hair dyes, Preservative in topical Hydrocortisone-17- 47 1% Temovate, 4 Paraphenylenediamine 1.0% photographic 26 Paraben mix 12% agents, cosmetics, butyrate Diprosone. chemicals foods. Methyldibromoglutar Preservative against Dimethylol In permanent press 27 0.5% 48 4.5% Imidazolidinyl urea Preservative, onitrile (MDBGN) bacteria and fungi dihydroxyethylene urea clothing. 5 2.0% (Germall 115) formaldehyde releaser Cocamidopropyl In hair and bath 28 Fragrance mix 1 8.0% In cosmetics, foods. 1% 49 ibetaine products. Cinnamic aldehyde 6 1.0% Fragrance. flavoring Disinfectant on (Cinnamyl) Group B steroids: 29 Glutaraldehyde 0.5% medical and dental 50 Triamcinolone acetonide 1.0% fluocinonide, TAC, 7 Amerchol L 101 50.0% Emulsifiers, Emollients equipment desonide. 2-Bromo-2- Preservative, Topical amide Rubber accelerator, 51 Lidocaine 15.0% 8 Carba mix 3.0% 30 nitropropane-l,3-diol 0.5% formaldehyde anesthetic. Adhesive (Bronopol) releaser. Topical amide Neomycin sulfate 20.0% Topical antibiotic. Sesquiterpene 52 Dibucaine hydrochloride 2.5% 9 0.1% Compositae flowers. anesthetic. 31 lactone Mix 10 Thiuram mix 1.0% Rubber accelerator Cosmetics, scents and Lauryl glucoside 3.0% surfactant Fragrance Mix II 14.0% 53 32 flavorings In leather, rubber, Clobetasol-17- plastics, disinfectants, Vehicle for cosmetics, 54 1.0% Group B steroids Formaldehyde 1.0% propionate 11 permanent press 33 Propylene glycol 30.0% topical medications. -

NIOSH Skin Notation Profiles Formaldehyde/Formalin
NIOSH Skin Notation Profiles Formaldehyde/Formalin IDSK [SK] SYS SYS (FATAL) DIR DIR (IRR) DIR (COR) SEN DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention SKNational Institute for Occupational Safety and Health NIOSH Skin Notation (SK) Profile Formaldehyde/Formalin [CAS No. 50–00–0] DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Institute for Occupational Safety and Health This document is in the public domain and may be freely copied or reprinted. Disclaimer Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites. Ordering Information To receive documents or other information about occupational safety and health topics, contact NIOSH at Telephone: 1–800–CDC–INFO (1–800–232–4636) TTY: 1–888–232–6348 E-mail: [email protected] or visit the NIOSH Web site at www.cdc.gov/niosh. For a monthly update on news at NIOSH, subscribe to NIOSH eNews by visiting www.cdc.gov/niosh/eNews. DHHS (NIOSH) Publication No. 2011–145 April 2011 Safer • Healthier • People™ ii Skin Notation Profiles | Formaldehyde/Formalin Foreword As the largest organ of the body, the skin performs multiple critical functions, such as serving as the primary barrier to the external environment. For this reason, the skin is often exposed to potentially hazardous agents, including chemicals, which may contribute to the onset of a spectrum of adverse health effects ranging from localized damage (e.g., irritant contact dermatitis and corrosion) to induction of immune-mediated responses (e.g., allergic contact dermatitis and pulmonary responses), or systemic toxicity (e.g., neurotoxicity and hepatoxicity). -

Relationship Between Formaldehyde and Quaternium15 Contact
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of Groningen University of Groningen Relationship between formaldehyde and quaternium-15 contact allergy. Influence of strength of patch test reactions de Groot, Anton C.; Blok, Janine; Coenraads, Pieter-Jan Published in: CONTACT DERMATITIS IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2010 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): de Groot, A. C., Blok, J., & Coenraads, P-J. (2010). Relationship between formaldehyde and quaternium-15 contact allergy. Influence of strength of patch test reactions. CONTACT DERMATITIS, 63(4), 187-191. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 12-11-2019 Contact Dermatitis 2010: 63: 187–191 © 2010 John Wiley & Sons A/S Printed in Singapore. -

Opinion of the Scientific Committee on Consumer Safety on Quaternium-15
SCCS/1344/10 Scientific Committee on Consumer Safety SCCS OPINION ON Quaternium-15 (cis-isomer) COLIPA n° P63 The SCCS adopted this opinion at its 13th plenary meeting of 13-14 December 2011 SCCS/1344/10 Opinion on quaternium-15 ___________________________________________________________________________________________ About the Scientific Committees Three independent non-food Scientific Committees provide the Commission with the scientific advice it needs when preparing policy and proposals relating to consumer safety, public health and the environment. The Committees also draw the Commission's attention to the new or emerging problems which may pose an actual or potential threat. They are: the Scientific Committee on Consumer Safety (SCCS), the Scientific Committee on Health and Environmental Risks (SCHER) and the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) and are made up of external experts. In addition, the Commission relies upon the work of the European Food Safety Authority (EFSA), the European Medicines Agency (EMA), the European Centre for Disease prevention and Control (ECDC) and the European Chemicals Agency (ECHA). SCCS The Committee shall provide opinions on questions concerning all types of health and safety risks (notably chemical, biological, mechanical and other physical risks) of non-food consumer products (for example: cosmetic products and their ingredients, toys, textiles, clothing, personal care and household products such as detergents, etc.) and services (for example: tattooing, artificial sun tanning, etc.). Scientific Committee members Jürgen Angerer, Ulrike Bernauer, Claire Chambers, Qasim Chaudhry, Gisela Degen, Elsa Nielsen, Thomas Platzek, Suresh Chandra Rastogi, Vera Rogiers, Christophe Rousselle, Tore Sanner, Jan van Benthem, Jacqueline van Engelen, Maria Pilar Vinardell, Rosemary Waring, Ian R. -
Formaldehyde and Formaldehyde Releasers
INVESTIGATION REPORT FORMALDEHYDE AND FORMALDEHYDE RELEASERS SUBSTANCE NAME: Formaldehyde IUPAC NAME: Methanal EC NUMBER: 200-001-8 CAS NUMBER: 50-00-0 SUBSTANCE NAME(S): - IUPAC NAME(S): - EC NUMBER(S): - CAS NUMBER(S):- CONTACT DETAILS OF THE DOSSIER SUBMITTER: EUROPEAN CHEMICALS AGENCY Annankatu 18, P.O. Box 400, 00121 Helsinki, Finland tel: +358-9-686180 www.echa.europa DATE: 15 March 2017 CONTENTS INVESTIGATION REPORT – FORMALDEHYDE AND FORMALDEHYDE RELEASERS ................ 1 1. Summary.............................................................................................................. 1 2. Report .................................................................................................................. 2 2.1. Background ........................................................................................................ 2 3. Approach .............................................................................................................. 4 3.1. Task 1: Co-operation with FR and NL ..................................................................... 4 3.2. Task 2: Formaldehyde releasers ........................................................................... 4 4. Results of investigation ........................................................................................... 6 4.1. Formaldehyde..................................................................................................... 6 4.2. Information on formaldehyde releasing substances and their uses ............................ 6 4.2.1. -

Imidazolidinyl Urea
Imidazolidinyl urea 39236-46-9 OVERVIEW This material was prepared for the National Cancer Institute (NCI) for consideration by the Chemical Selection Working Group (CSWG) by Technical Resources International, Inc. under contract no. N02-07007. Imidazolidinyl urea came to the attention of the NCI Division of Cancer Biology (DCB) as the result of a class study on formaldehyde releasers. Used in combination with parabens, imidazolidinyl urea is one of the most widely used preservative systems in the world and is commonly found in cosmetics. Based on a lack of information in the available literature on the carcinogenicity and genetic toxicology, DCB forwarded imidazolidinyl urea to the NCI Short-Term Toxicity Program (STTP) for mutagenicity testing. Based on the results from the STTP, further toxicity testing of imidazolidinyl urea may be warranted. INPUT FROM GOVERNMENT AGENCIES/INDUSTRY Dr. John Walker, Executive Director of the TSCA Interagency Testing Committee (ITC), provided information on the production volumes for this chemical. Dr. Harold Seifried of the NCI provided mutagenicity data from the STTP. NOMINATION OF IMIDAZOLIDINYL UREA TO THE NTP Based on a review of available relevant literature and the recommendations of the Chemical Selection Working Group (CSWG) held on December 17, 2003, NCI nominates this chemical for testing by the National Toxicology Program (NTP) and forwards the following information: • The attached Summary of Data for Chemical Selection • Copies of references cited in the Summary of Data for Chemical Selection • CSWG recommendations to: (1) Evaluate the chemical for genetic toxicology in greater depth than the existing data, (2) Evaluate the disposition of the chemical in rodents, specifically for dermal absorption, (3) Expand the review of the information to include an evaluation of possible break- down products, especially diazolidinyl urea and formaldehyde.