Clinical Pharmacy Newsletter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplement Ii to the Japanese Pharmacopoeia Fifteenth Edition
SUPPLEMENT II TO THE JAPANESE PHARMACOPOEIA FIFTEENTH EDITION Official From October 1, 2009 English Version THE MINISTRY OF HEALTH, LABOUR AND WELFARE Notice: This English Version of the Japanese Pharmacopoeia is published for the conven- ience of users unfamiliar with the Japanese language. When and if any discrepancy arises between the Japanese original and its English translation, the former is authentic. The Ministry of Health, Labour and Welfare Ministerial Notification No. 425 Pursuant to Paragraph 1, Article 41 of the Pharmaceutical Affairs Law (Law No. 145, 1960), we hereby revise a part of the Japanese Pharmacopoeia (Ministerial Notification No. 285, 2006) as follows*, and the revised Japanese Pharmacopoeia shall come into ef- fect on October 1, 2009. However, in the case of drugs which are listed in the Japanese Pharmacopoeia (hereinafter referred to as “previous Pharmacopoeia”) [limited to those listed in the Japanese Pharmacopoeia whose standards are changed in accordance with this notification (hereinafter referred to as “new Pharmacopoeia”)] and drugs which have been approved as of October 1, 2009 as prescribed under Paragraph 1, Article 14 of the same law [including drugs the Minister of Health, Labour and Welfare specifies (the Ministry of Health and Welfare Ministerial Notification No. 104, 1994) as those ex- empted from marketing approval pursuant to Paragraph 1, Article 14 of the Pharmaceu- tical Affairs Law (hereinafter referred to as “drugs exempted from approval”)], the Name and Standards established in the previous Pharmacopoeia (limited to part of the Name and Standards for the drugs concerned) may be accepted to conform to the Name and Standards established in the new Pharmacopoeia before and on March 31, 2011. -

Consideration of Antibacterial Medicines As Part Of
Consideration of antibacterial medicines as part of the revisions to 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) Section 6.2 Antibacterials including Access, Watch and Reserve Lists of antibiotics This summary has been prepared by the Health Technologies and Pharmaceuticals (HTP) programme at the WHO Regional Office for Europe. It is intended to communicate changes to the 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) to national counterparts involved in the evidence-based selection of medicines for inclusion in national essential medicines lists (NEMLs), lists of medicines for inclusion in reimbursement programs, and medicine formularies for use in primary, secondary and tertiary care. This document does not replace the full report of the WHO Expert Committee on Selection and Use of Essential Medicines (see The selection and use of essential medicines: report of the WHO Expert Committee on Selection and Use of Essential Medicines, 2019 (including the 21st WHO Model List of Essential Medicines and the 7th WHO Model List of Essential Medicines for Children). Geneva: World Health Organization; 2019 (WHO Technical Report Series, No. 1021). Licence: CC BY-NC-SA 3.0 IGO: https://apps.who.int/iris/bitstream/handle/10665/330668/9789241210300-eng.pdf?ua=1) and Corrigenda (March 2020) – TRS1021 (https://www.who.int/medicines/publications/essentialmedicines/TRS1021_corrigenda_March2020. pdf?ua=1). Executive summary of the report: https://apps.who.int/iris/bitstream/handle/10665/325773/WHO- MVP-EMP-IAU-2019.05-eng.pdf?ua=1. -

WO 2010/025328 Al
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 4 March 2010 (04.03.2010) WO 2010/025328 Al (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/00 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, (21) International Application Number: CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, PCT/US2009/055306 DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, 28 August 2009 (28.08.2009) KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, (25) Filing Language: English NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, (26) Publication Language: English SE, SG, SK, SL, SM, ST, SV, SY, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: 61/092,497 28 August 2008 (28.08.2008) US (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (71) Applicant (for all designated States except US): FOR¬ GM, KE, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, ZM, EST LABORATORIES HOLDINGS LIMITED [IE/ ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, —]; 18 Parliament Street, Milner House, Hamilton, TM), European (AT, BE, BG, CH, CY, CZ, DE, DK, EE, Bermuda HM12 (BM). -

Computational Antibiotics Book
Andrew V DeLong, Jared C Harris, Brittany S Larcart, Chandler B Massey, Chelsie D Northcutt, Somuayiro N Nwokike, Oscar A Otieno, Harsh M Patel, Mehulkumar P Patel, Pratik Pravin Patel, Eugene I Rowell, Brandon M Rush, Marc-Edwin G Saint-Louis, Amy M Vardeman, Felicia N Woods, Giso Abadi, Thomas J. Manning Computational Antibiotics Valdosta State University is located in South Georgia. Computational Antibiotics Index • Computational Details and Website Access (p. 8) • Acknowledgements (p. 9) • Dedications (p. 11) • Antibiotic Historical Introduction (p. 13) Introduction to Antibiotic groups • Penicillin’s (p. 21) • Carbapenems (p. 22) • Oxazolidines (p. 23) • Rifamycin (p. 24) • Lincosamides (p. 25) • Quinolones (p. 26) • Polypeptides antibiotics (p. 27) • Glycopeptide Antibiotics (p. 28) • Sulfonamides (p. 29) • Lipoglycopeptides (p. 30) • First Generation Cephalosporins (p. 31) • Cephalosporin Third Generation (p. 32) • Fourth-Generation Cephalosporins (p. 33) • Fifth Generation Cephalosporin’s (p. 34) • Tetracycline antibiotics (p. 35) Computational Antibiotics Antibiotics Covered (in alphabetical order) Amikacin (p. 36) Cefempidone (p. 98) Ceftizoxime (p. 159) Amoxicillin (p. 38) Cefepime (p. 100) Ceftobiprole (p. 161) Ampicillin (p. 40) Cefetamet (p. 102) Ceftoxide (p. 163) Arsphenamine (p. 42) Cefetrizole (p. 104) Ceftriaxone (p. 165) Azithromycin (p.44) Cefivitril (p. 106) Cefuracetime (p. 167) Aziocillin (p. 46) Cefixime (p. 108) Cefuroxime (p. 169) Aztreonam (p.48) Cefmatilen ( p. 110) Cefuzonam (p. 171) Bacampicillin (p. 50) Cefmetazole (p. 112) Cefalexin (p. 173) Bacitracin (p. 52) Cefodizime (p. 114) Chloramphenicol (p.175) Balofloxacin (p. 54) Cefonicid (p. 116) Cilastatin (p. 177) Carbenicillin (p. 56) Cefoperazone (p. 118) Ciprofloxacin (p. 179) Cefacetrile (p. 58) Cefoselis (p. 120) Clarithromycin (p. 181) Cefaclor (p. -

Jp Xvii the Japanese Pharmacopoeia
JP XVII THE JAPANESE PHARMACOPOEIA SEVENTEENTH EDITION Official from April 1, 2016 English Version THE MINISTRY OF HEALTH, LABOUR AND WELFARE Notice: This English Version of the Japanese Pharmacopoeia is published for the convenience of users unfamiliar with the Japanese language. When and if any discrepancy arises between the Japanese original and its English translation, the former is authentic. The Ministry of Health, Labour and Welfare Ministerial Notification No. 64 Pursuant to Paragraph 1, Article 41 of the Law on Securing Quality, Efficacy and Safety of Products including Pharmaceuticals and Medical Devices (Law No. 145, 1960), the Japanese Pharmacopoeia (Ministerial Notification No. 65, 2011), which has been established as follows*, shall be applied on April 1, 2016. However, in the case of drugs which are listed in the Pharmacopoeia (hereinafter referred to as ``previ- ous Pharmacopoeia'') [limited to those listed in the Japanese Pharmacopoeia whose standards are changed in accordance with this notification (hereinafter referred to as ``new Pharmacopoeia'')] and have been approved as of April 1, 2016 as prescribed under Paragraph 1, Article 14 of the same law [including drugs the Minister of Health, Labour and Welfare specifies (the Ministry of Health and Welfare Ministerial Notification No. 104, 1994) as of March 31, 2016 as those exempted from marketing approval pursuant to Paragraph 1, Article 14 of the Same Law (hereinafter referred to as ``drugs exempted from approval'')], the Name and Standards established in the previous Pharmacopoeia (limited to part of the Name and Standards for the drugs concerned) may be accepted to conform to the Name and Standards established in the new Pharmacopoeia before and on September 30, 2017. -

Pharmaceutical Appendix to the Harmonized Tariff Schedule
Harmonized Tariff Schedule of the United States Basic Revision 3 (2021) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States Basic Revision 3 (2021) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names INN which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service CAS registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. -

Revision of Precautions
Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. Revision of Precautions Cefmenoxime hydrochloride (preparations for otic and nasal use), chloramphenicol (solution for topical use, oral dosage form), tetracycline hydrochloride (powders, capsules), polymixin B sulfate (powders), clindamycin hydrochloride, clindamycin phosphate (injections), benzylpenicillin potassium, benzylpenicillin benzathine hydrate, lincomycin hydrochloride hydrate, aztreonam, amoxicillin hydrate, ampicillin hydrate, ampicillin sodium, potassium clavulanate/amoxicillin hydrate, dibekacin sulfate (injections), sultamicillin tosilate hydrate, cefaclor, cefazolin sodium, cefazolin sodium hydrate, cephalexin (oral dosage form with indications for otitis media), cefalotin sodium, cefixime hydrate, cefepime dihydrochloride hydrate, cefozopran hydrochloride, cefotiam hydrochloride (intravenous injections), cefcapene pivoxil hydrochloride hydrate, cefditoren pivoxil, cefdinir, ceftazidime hydrate, cefteram pivoxil, ceftriaxone sodium hydrate, cefpodoxime proxetil, cefroxadine hydrate, cefuroxime axetil, tebipenem pivoxil, doripenem hydrate, bacampicillin hydrochloride, panipenem/betamipron, faropenem sodium hydrate, flomoxef sodium, fosfomycin calcium hydrate, meropenem hydrate, chloramphenicol sodium succinate, -

Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DIX to the HTSUS—Continued
20558 Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DEPARMENT OF THE TREASURY Services, U.S. Customs Service, 1301 TABLE 1.ÐPHARMACEUTICAL APPEN- Constitution Avenue NW, Washington, DIX TO THE HTSUSÐContinued Customs Service D.C. 20229 at (202) 927±1060. CAS No. Pharmaceutical [T.D. 95±33] Dated: April 14, 1995. 52±78±8 ..................... NORETHANDROLONE. A. W. Tennant, 52±86±8 ..................... HALOPERIDOL. Pharmaceutical Tables 1 and 3 of the Director, Office of Laboratories and Scientific 52±88±0 ..................... ATROPINE METHONITRATE. HTSUS 52±90±4 ..................... CYSTEINE. Services. 53±03±2 ..................... PREDNISONE. 53±06±5 ..................... CORTISONE. AGENCY: Customs Service, Department TABLE 1.ÐPHARMACEUTICAL 53±10±1 ..................... HYDROXYDIONE SODIUM SUCCI- of the Treasury. NATE. APPENDIX TO THE HTSUS 53±16±7 ..................... ESTRONE. ACTION: Listing of the products found in 53±18±9 ..................... BIETASERPINE. Table 1 and Table 3 of the CAS No. Pharmaceutical 53±19±0 ..................... MITOTANE. 53±31±6 ..................... MEDIBAZINE. Pharmaceutical Appendix to the N/A ............................. ACTAGARDIN. 53±33±8 ..................... PARAMETHASONE. Harmonized Tariff Schedule of the N/A ............................. ARDACIN. 53±34±9 ..................... FLUPREDNISOLONE. N/A ............................. BICIROMAB. 53±39±4 ..................... OXANDROLONE. United States of America in Chemical N/A ............................. CELUCLORAL. 53±43±0 -
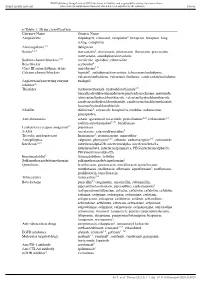
E-Table 1. Drug Classification Category Name Generic Name
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) Thorax e-Table 1. Drug classification Category Name Generic Name Antiplatelets clopidogrel, cilostazol, ticlopidine2, beraprost, beraprost–long acting, complavin Anticoagulants 2,3 dabigatran Statins1,2,3 atorvastatin2, simvastatin, pitavastatin, fluvastatin, pravastatin, rosuvastatin, amlodipine/atorvastatin Sodium channel blockers4,5† mexiletine, aprindine, cibenzoline Beta blocker acebutolol2 Class III antiarrhythmic drugs amiodarone1–6 Calcium channel blockers bepridil1, amlodipine/atorvastatin, telmisartan/amlodipine, valsartan/amlodipine, valsartan/cilnidipine, candesartan/amlodipine Angiotensin/converting enzyme enalapril inhibitor2‡ Thiazides trichlormethiazide, hydrochlorothiazide3,5, benzylhydrochlorothiazide/reserpine/carbazochrome, mefruside, telmisartan/hydrochlorothiazide, valsartan/hydrochlorothiazide, candesartan/hydrochlorothiazide, candesartan/trichlormethiazide, losartan/hydrochlorothiazide NSAIDs diclofenac2, celecoxib, loxoprofen, etodolac, nabumetone, pranoprofen Anti-rheumatics actarit, iguratimod, tofacitinib, penicillamine2–5, leflunomide1,3, sodium aurothiomalate2–6#, bucillamine Leukotriene receptor antagonist2* pranlukast 5-ASA mesalazine, salazosulfapyridine5 Tricyclic antidepressant Imipramine5, cromipramine, maprotiline Antiepileptics valproate, phenytoin2,3,5, ethotoin, carbamazepine2–5, zonisamide Interferon1,2,3 -

Directed Molecular Evolution of Fourth-Generation Cephalosporin Resistance in Wellington Moore Iowa State University
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2011 Directed molecular evolution of fourth-generation cephalosporin resistance in Wellington Moore Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the Medical Sciences Commons Recommended Citation Moore, Wellington, "Directed molecular evolution of fourth-generation cephalosporin resistance in" (2011). Graduate Theses and Dissertations. 10107. https://lib.dr.iastate.edu/etd/10107 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Directed molecular evolution of fourth-generation cephalosporin resistance in Salmonella and Yersinia by Wellington Moore A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Major: Biomedical Science (Pharmacology) Program of Study Committee: Steve Carlson, Major Professor Timothy Day Ronald Griffith Iowa State University Ames, Iowa 2011 ii TABLE OF CONTENTS LIST OF FIGURES………………………………………………………………………iii LIST OF TABLES………………………………………………………………………..iv ABSTRACT……………………………………………………………………………….v CHAPTER 1. INTRODUCTION…………………………………………………………1 Review of B-Lactam antimicrobials………………………………...………1 -

Extended Spectrum Beta-Lactamases
Extended spectrum beta-lactamases A. Beta-lactam antibiotics a. Structure b. Types c. Action d. Mechanism of resistances B. Beta-lactamases a. Classical beta-lactamases b. Extended spectrum beta-lactamases (ESBL) c. Non-TEM, non-SBV ESBL d. Inhibitor Resistant TEM (IRT) C. Definition, classification and properties of ESBL D. Epidemiology and risk factors E. Laboratory detection and identification of ESBLs a. Screening, phenotypic and genotypic methods b. Co-production of ESBL and AmpC beta-lactamases F. Beta-lactamase inhibitors G. Multiple drug resistance H. Treatment options against ESBL producers A. Beta-lactam antibiotics A β-lactam (beta-lactam) ring is a four-membered cyclic amide consisting of three carbon atoms and one nitrogen atom. It is named so, because the nitrogen atom is attached to the β-carbon relative to the carbonyl (C=O). Antibiotics possessing this structure are called beta-lactam antibiotics. Penams contain a β-lactam ring fused to a 5- membered ring, where one of the atoms in the ring is a sulfur and the ring is fully saturated. A carbapenam is a β-lactam compound that is a saturated carbapenem. They exist primarily as biosynthetic intermediates on the way to the carbapenem antibiotics. A clavam is a molecule similar to a penam, but with an oxygen atom substituted for the sulfur. Thus, they are also known as oxapenams. Carbapenems are very similar to the penams, but the sulfur atom of the unsaturated structure is replaced with a carbon atom. Penem is a type of unsaturated β-lactam, which is similar in structure to carbapenems but penems have a sulfur atom instead of carbon. -

Antibiotic Classes
Penicillins Aminoglycosides Generic Brand Name Generic Brand Name Amoxicillin Amoxil, Polymox, Trimox, Wymox Amikacin Amikin Ampicillin Omnipen, Polycillin, Polycillin-N, Gentamicin Garamycin, G-Mycin, Jenamicin Principen, Totacillin, Unasyn Kanamycin Kantrex Bacampicillin Spectrobid Neomycin Mycifradin, Myciguent Carbenicillin Geocillin, Geopen Netilmicin Netromycin Cloxacillin Cloxapen Paromomycin Dicloxacillin Dynapen, Dycill, Pathocil Streptomycin Flucloxacillin Flopen, Floxapen, Staphcillin Tobramycin Nebcin Mezlocillin Mezlin Nafcillin Nafcil, Nallpen, Unipen Quinolones Oxacillin Bactocill, Prostaphlin Generic Brand Name Penicillin G Bicillin L-A, First Generation Crysticillin 300 A.S., Pentids, Flumequine Flubactin Permapen, Pfizerpen, Pfizerpen- Nalidixic acid NegGam, Wintomylon AS, Wycillin Oxolinic acid Uroxin Penicillin V Beepen-VK, Betapen-VK, Piromidic acid Panacid Ledercillin VK, V-Cillin K Pipemidic acid Dolcol Piperacillin Pipracil, Zosyn Rosoxacin Eradacil Pivampicillin Second Generation Pivmecillinam Ciprofloxacin Cipro, Cipro XR, Ciprobay, Ciproxin Ticarcillin Ticar Enoxacin Enroxil, Penetrex Lomefloxacin Maxaquin Monobactams Nadifloxacin Acuatim, Nadoxin, Nadixa Generic Brand Name Norfloxacin Lexinor, Noroxin, Quinabic, Aztreonam Azactam, Cayston Janacin Ofloxacin Floxin, Oxaldin, Tarivid Carbapenems Pefloxacin Peflacine Generic Brand Name Rufloxacin Uroflox Imipenem, Primaxin Third Generation Imipenem/cilastatin Balofloxacin Baloxin Doripenem Doribax Gatifloxacin Tequin, Zymar Meropenem Merrem Grepafloxacin Raxar Ertapenem