Diphenhydramine and Pregnancy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
For Personal Use Only
SedatiWITH ANTIi ® Dowden Health Media CopyrightFor personal use only Initiate the antipsychotic at a reasonable, not overly high dose, then use a nonantipsychotic to help control insomnia, anxiety, and agitation For mass reproduction, content licensing and permissions contact Dowden Health Media. pSYCHIATRY i PSYCHOTICSon edation is a frequent side effect of antipsychot- ics, especially at relatively high doses. Antipsy- S chotics’ sedative effects can reduce agitation in acute psychosis and promote sleep in insomnia, but Manage, don’t long-term sedation may: • interfere with schizophrenia patients’ efforts to go accept adverse to work or school or engage in normal socialization • prevent improvement from psychosocial training, psychiatric rehabilitation, and other treatments. ‘calming’ eff ect This article discusses how to manage acute psycho- sis without oversedation and ways to address persistent sedation and chronic insomnia with less-sedating anti- Del D. Miller, PharmD, MD Professor of psychiatry psychotics or adjunctive medications. University of Iowa Carver College of Medicine Iowa City Neurobiology or psychopharmacology? Many patients experience only mild, transient som- nolence at the beginning of antipsychotic treatment, and most develop some tolerance to the sedating ef- fects with continued administration. Others may have persistent daytime sedation that interferes with nor- mal functioning. Sedation is especially common in elderly patients re- ceiving antipsychotics. Compared with younger patients, older patients receiving -

The Case of Ketamine Allergy
CASE REPORT The Case of Ketamine Allergy William Bylund, MD Department of Emergency Medicine, Naval Medical Center Portsmouth, Portsmouth, Virginia Liam Delahanty, MD Maxwell Cooper, MD Section Editor: Rick A. McPheeters, DO Submission history: Submitted April 3, 2017; Revision received June 29, 2017; Accepted July 11, 2017 Electronically published October 3, 2017 Full text available through open access at http://escholarship.org/uc/uciem_cpcem DOI: 10.5811/cpcem.2017.7.34405 Ketamine is often used for pediatric procedural sedation due to low rates of complications, with allergic reactions being rare. Immediately following intramuscular (IM) ketamine administration, a three-year-old female rapidly developed facial edema and diffuse urticarial rash, with associated wheezing and oxygen desaturation. Symptoms resolved following treatment with epinephrine, dexamethasone and diphenhydramine. This case presents a clinical reaction to ketamine consistent with anaphylaxis due to histamine release, but it is uncertain whether this was immunoglobulin E mediated. This is the only case reported to date of allergic reaction to IM ketamine, without co- administration of other agents. [Clin Pract Cases Emerg Med.2017;1(4):323–325.] INTRODUCTION cardiac monitor, end tidal CO2 (ETCO2) and pulse oximetry Ketamine is a common medication, used in isolation as well (POx), in addition to being placed on two liters nasal cannula as with other agents, for pediatric sedation in the emergency (NC). No intravenous (IV) access was obtained prior to sedation. department (ED). It is often turned to because of its efficacy, ease Seventy milligrams (4.4mg/kg) of ketamine was administered IM of use, and favorable safety profile. Common side effects of into the right thigh. -

Diphenhydramine Dosage Sheet Concord Pediatrics, P.A
Diphenhydramine Dosage Sheet Concord Pediatrics, P.A. (603) 224-1929 BRAND NAMES: Benadryl INDICATIONS: Treatment of allergic reactions, nasal allergies, hives and itching. FREQUENCY: Repeat every 6 hours as needed. Don't give more than 4 times a day. DOSAGE: Determine by using the table below. Please speak with a medical provider before giving Diphenhydramine to a child under 1 year old. Child’s Dose in mg Children’s Liquid Chewable/Fastmelts Tabs/Caps/Gels Weight (lb) (12.5mg/ 5mL) 12.5mg tablets 25mg tablets *12-16 lbs 6.25 mg 2.5 mL *17-19 lbs 9.375 mg 3.75 mL *20-24 lbs 10 mg 4 mL 25-37 lbs 12.5 mg 5 mL 1 tab 38-49 lbs 18.75 mg 7.5 mL 1.5 tabs 50-69 lbs 25 mg 10 mL 2 tabs 1 tab 70-99 lbs 37.5 mg 15 mL 3 tabs 1.5 tabs >100 lbs 50 mg 20 mL 4 tabs 2 tabs Table Notes: *AGE LIMIT: For allergies, don't use under 1 year of age (Reason: it's a sedative). For colds, not recommended at any age (Reason: no proven benefits) and should be avoided if under 4 years old. Avoid multi-ingredient products in children under 6 years of age (Reason: FDA recommendations 10/2008). MEASURING the DOSAGE: Syringes and droppers are more accurate than teaspoons. If possible, use the syringe or dropper that comes with the medicine. If not, medicine syringes are available at pharmacies. Regular spoons are not reliable. ADULT DOSAGE: 50 mg Why use Diphenhydramine? Antihistamines can be used to treat your child’s runny nose, itchy eyes, and sneezing due to allergies. -

Histamine and Antihistamines
ACTA FACULTATIS MEDICAE NAISSENSIS UDC: 615.218 DOI: 10.1515/afmnai-2015-0001 Review article Histamine and Antihistamines Nikola Stojković1, Snežana Cekić2, Milica Ristov3, Marko Ristić1, Davor Đukić1, Maša Binić1, Dragan Virijević1 1University of Niš, Faculty of Medicine, PhD student, Serbia 2Institute of Physiology, University of Niš, Faculty of Medicine , Serbia 3Doctor of Medicine SUMMARY In recent years, there has been a steady increase in the prevalence of allergic diseases. Allergic immune response represents a complex network of cellular events involving numerous immune cells and mediators. It represents the interaction of innate and acquired immune response. The key role in the immune cascade is taken by histamine, a natural component of the body, which in the allergic inflammatory response is releasesd by the mast cells and basophils. The aim of this study was to highlight the role of histamine in allergic immunological events, their effect on Th1 and Th2 subpopulation of lymphocytes and the production of the corresponding cytokines, as well as the role of histamine blockers in the treatment of these conditions. Histamine achieves its effect by binding to the four types of its receptors, which are widely distributed in the body. Histamine blockers block a numerous effects of histamine by binding to these receptors. As a highly selective second-generation antihistamine, cetirizine not only achieves its effects by binding to H1 receptors, but also attenuates numerous events during the inflammatory process. Knowledge of the effects -

Download Large Text CMI (PDF)
Children's Paedamin Antihistamine Oral Liquid Decongestant and Antihistamine Children 6-12 years Consumer Medicine Information What is in this leaflet? • Itchy, watery eyes Before you give • Nasal congestion Children's Paedamin This leaflet answers some common Children's Paedamin Decongestant Decongestant and questions about Children's and Antihistamine contains Antihistamine Paedamin® Decongestant and Diphenhydramine Hydrochloride Antihistamine. and Phenylephrine Hydrochloride. When you must not give it It does not contain all the available Diphenhydramine Hydrochloride Do not use Children's Paedamin information. It does not take the belongs to a group of medicines Decongestant and Antihistamine if place of talking to your doctor or called 'antihistamines'. you/ your child have an allergy to: pharmacist. Antihistamines help reduce allergic All medicines have risks and symptoms, such as sneezing, runny • any medicine containing benefits. Your doctor or pharmacist nose or itchy, watery eyes, by Diphenhydramine has weighed the risks of you/your preventing the effects of a substance Hydrochloride or other child taking Children's Paedamin called histamine. Histamine is antihistamines Decongestant and Antihistamine produced by the body in response to • any medicine containing against the benefits they expect it foreign substances that the body is Phenylephrine Hydrochloride will have for you. allergic to. • any of the ingredients listed at If you have any concerns about Phenylephrine Hydrochloride the end of this leaflet taking this medicine, ask your belongs to a group of medicines Some of the symptoms of an doctor or pharmacist. called decongestants. allergic reaction may include: Keep this leaflet with the It works by reducing congestion in • shortness of breath medicine. -

Chronic Pain Management Toolkit
Chronic Pain Management Urine Drug Testing Toolkit Screening (see chart on next page) Most guidelines recommend screening patients to determine risks of drug misuse and abuse and to mitigate those risks as much as possible. Unfortunately, there are no risk assessment tools that have been validated in multiple settings and populations. Screening is typically based on risk factors that can be identified through a thorough patient history, the use of prescription drug monitoring programs (PDMPs), the opioid risk tool (provided in this toolkit), and, on occasion, drug screening. However, it is important to standardize testing as cited risk factors (e.g. sociodemographic factors, psychological comorbidity, substance use disorders, etc.) might unfairly impact certain vulnerable populations. Involvement of the whole health care team and full disclosure and discussion of the screening protocol with patients is central to providing patient-centered and comprehensive pain management. Prior to drug testing, physicians should inform the patient of the reason(s) for testing, how often they will be tested, and what the results might mean. This gives patients an opportunity to disclose any additional drug or substance use which may help with identification of false positives and appropriate interpretation of test results. Physicians must understand the limitations of the urine and confirmatory tests available, including what substances are detected by a particular test, and the reasons for false-positive and false-negative tests. Changes in prescribing for a particular patient should not be based on the result of one abnormal screening test, but should only occur after looking at all available monitoring tools as well as repeating the drug screen with the most specific test available. -

Children with Respiratory Disorders: Asthma and Allergies
Oral Health Fact Sheet for Dental Professionals Children with Respiratory Disorders: Asthma and Allergies Asthma is a chronic respiratory disease associated with airway obstruction, with recurrent attacks of paroxysmal dyspnea, and wheezing due to spasmodic contraction of the bronchi. (ICD 9 code 493.2) Allergy is a hypersensitivity to an agent caused by an immunologic response to an initial exposure. (ICD 9 code 995.3) Prevalence • Asthma affects 9.3% of the population, higher in females and African-Americans Manifestations Clinical • Constriction of bronchi, coughing, wheezing, chest tightness, and shortness of breath Oral • Increased caries risk, enamel defects • Increased gingivitis and periodontal disease risk; and more calculus • Higher rates of malocclusion and increased: overjet, overbite, posterior crossbite; high palatal vault • Oral candidiasis, xerostomia, decreased salivary flow rate and salivary pH Other Potential Disorders/Concerns • none Management Medication SYMPTOM MEDICATION SIDE EFFECTS Breathing difficulties A. Bronchodilators (Β2-agonists) A. Oral candidiasis, xerostomia, decreased salivary flow rate B. Corticosteroids B. Oral candidiasis, dental caries C. Antihistamines C. Xerostomia D. Decongestants D. Xerostomia Sedation • Hydroxyzine and benzodiazepines recommended; avoid narcotics and barbiturates due to their histamine releasing properties → bronchospasm and potentiated allergic response. Intravenous sedation • Use extreme caution due to limited control of the airway. Avoid • Aspirin, other salicylates and NSAIDS (due to allergies) may provoke a severe exacerbation of bronchoconstriction; use acetaminophen. Behavioral Stress-management techniques; may use nitrous oxide in mild to moderate asthmatics after medical consultation. Anxiety can cause acute exacerbation. Children with Respiratory Disorders: Asthma and Allergies continued Dental Treatment and Prevention • Assess child’s risk of acute exacerbation/anaphylaxis during dental treatment prior to examination. -
OTC DOSING GUIDE Benadryl
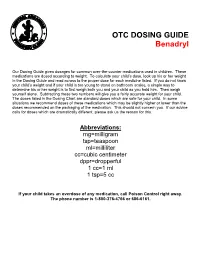
OTC DOSING GUIDE Benadryl Our Dosing Guide gives dosages for common over-the-counter medications used in children. These medications are dosed according to weight. To calculate your child’s dose, look up his or her weight in the Dosing Guide and read across to the proper dose for each medicine listed. If you do not know your child’s weight and if your child is too young to stand on bathroom scales, a simple way to determine his or her weight is to first weigh both you and your child as you hold him. Then weigh yourself alone. Subtracting these two numbers will give you a fairly accurate weight for your child. The doses listed in the Dosing Chart are standard doses which are safe for your child. In some situations we recommend doses of these medications which may be slightly higher or lower than the doses recommended on the packaging of the medication. This should not concern you. If our advice calls for doses which are dramatically different, please ask us the reason for this. Abbreviations: mg=milligram tsp=teaspoon ml=milliliter cc=cubic centimeter dppr=dropperful 1 cc=1 ml 1 tsp=5 cc If your child takes an overdose of any medication, call Poison Control right away. The phone number is 1-800-376-4766 or 686-6161. CHILDREN’S BENADRYL ALLERGY LIQUID (Generic Name: Diphenhydramine) (Antihistamine) NEVER GIVE TO INFANTS LESS THAN 6 MONTHS OLD. DO NOT GIVE TO CHILDREN LESS THAN 2 YEARS OLD UNLESS ADVISED BY A PHYSICIAN. Dosage: Every 4 -6 hours. -
Doxylamine Succinate-Pyridoxine Hydrochloride
Doxylamine succinate-pyridoxine hydrochloride This sheet is about exposure to doxylamine succinate-pyridoxine hydrochloride in pregnancy and while breastfeeding. This information should not take the place of medical care and advice from your healthcare providers. What is doxylamine succinate-pyridoxine hydrochloride? The combination of 10mg of doxylamine succinate and 10mg of pyridoxine hydrochloride is a medication used to treat nausea and vomiting of pregnancy (NVP), also called “morning sickness.” For more information on NVP, please see the MotherToBaby fact sheet Nausea and Vomiting of Pregnancy (https://mothertobaby.org/fact-sheets/nausea-vomiting-pregnancy-nvp/pdf/). Doxylamine succinate is an antihistamine. Antihistamines lessen the symptoms of allergic reactions and colds and help to treat insomnia (hard time sleeping). Pyridoxine hydrochloride is a form of vitamin B6. In the United States, the combination of doxylamine and pyridoxine has been sold under the name Diclegis® since 2013. In Canada, it has been sold under the brand name Diclectin®. Diclegis® and Diclectin® are delayed-release tablets available by prescription. Delayed-release means that the tablet coating prevents the ingredients from being absorbed too quickly by the body. Doxylamine succinate and/or pyridoxine hydrochloride may also be available as over-the- counter medicines. I take doxylamine succinate-pyridoxine hydrochloride. Can it make it harder for me to get pregnant? Based on the data available, it is not known if doxylamine succinate-pyridoxine hydrochloride can make it harder to become pregnant. I just found out I am pregnant. Should I stop taking doxylamine succinate-pyridoxine hydrochloride? Talk with your healthcare providers before making any changes to how you take your medication(s). -

Doxylamine/Pyridoxine
BonjestaTM (doxylamine/pyridoxine) – New Drug Approval • On November 7, 2016, the FDA approved Duchesnay’s Bonjesta (doxylamine/pyridoxine) for the treatment of nausea and vomiting of pregnancy in women who do not respond to conservative management. — Bonjesta has not been studied in women with hyperemesis gravidarum. • Bonjesta is a fixed dose combination product containing an antihistamine (doxylamine) and a vitamin B6 analog (pyridoxine). The exact mechanism of Bonjesta is not known. — Doxylamine/pyridoxine is also available as Diclegis®, which contains 10 mg of doxylamine and 10 mg of pyridoxine as delayed-release tablets for the same indication. • There have been no efficacy and safety trials for Bonjesta. However, a placebo-controlled study was conducted to support the safety and efficacy of 10 mg doxylamine succinate and 10 mg pyridoxine hydrochloride tablets (a different formulation and dosage strength than Bonjesta) in the treatment of nausea and vomiting of pregnancy. • Bonjesta is contraindicated in women with known hypersensitivity to doxylamine, other ethanolamine derivative antihistamines, or pyridoxine or any inactive ingredient in the formulation; monoamine oxidase (MAO) inhibitors intensify and prolong the adverse central nervous system effects of Bonjesta. • Warnings and precautions of Bonjesta include somnolence and concomitant medical conditions. • The most common adverse event (≥ 5% and exceeding placebo) with combination 10 mg doxylamine and 10 mg pyridoxine tablets was somnolence. • The recommended dose of Bonjesta is one tablet orally at bedtime on day 1. If the dose adequately controls symptoms the next day, the patient may continue taking one tablet daily at bedtime only. However, if symptoms persist on day 2, the dose may be increased to one tablet in the morning and one tablet at bedtime. -

Doxepin (Dox-E-Pin) Description: Tricyclic Antidepressant; Antihistamine Other Names for This Medication: Sinequan®, Silenor® Common Dosage Forms: Veterinary: None
Prescription Label Patient Name: Species: Drug Name & Strength: Directions (amount to give how often & for how long): Prescribing Veterinarian's Name & Contact Information: Refills: [Content to be provided by prescribing veterinarian] Doxepin (dox-e-pin) Description: Tricyclic Antidepressant; Antihistamine Other Names for this Medication: Sinequan®, Silenor® Common Dosage Forms: Veterinary: None. Human: 3 mg, 6 mg, 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, & 150 mg capsules; 10 mg/mL oral liquid concentrates. This information sheet does not contain all available information for this medication. It is to help answer commonly asked questions and help you give the medication safely and effectively to your animal. If you have other questions or need more information about this medication, contact your veterinarian or pharmacist. Key Information When used as an antihistamine, doxepin should be used on a regular, ongoing basis in animals that respond to it. This drug works better if used before exposure to an allergen (eg, pollens). When used for behavior modification, it may take several days to weeks to determine if doxepin is effective. May be given with or without food. If your animal vomits or acts sick after receiving the drug on an empty stomach, try giving the next dose with food or a small treat. If vomiting continues, contact your veterinarian. Most common side effects are sleepiness, dry mouth, and constipation. Be sure your animal always has access to plenty of fresh, clean water. Rare side effects that can be serious (contact veterinarian immediately) include abnormal bleeding, lack of an appetite, seizures, collapse, or profound sleepiness. -

Ketamine and Serotonin Syndrome: a Case Report
Residents’ Voices Ketamine and serotonin syndrome: A case report Clay Gueits, MD, and Martin Witkin, DO ong utilized as a rapid anesthetic, ket- with haloperidol (dose unknown) with amine has been increasingly used in reportedly good effect. On Day 7, she was Lsub-anesthetic doses for several psy- discharged home. chiatric indications, including depression, Upon returning home, she experienced suicidality, and chronic pain. Recently, persistent altered mental status. Her signifi- an intranasal form of esketamine—the cant other brought her to our hospital for fur- S-enantiomer of ketamine—was FDA- ther workup. Ms. O’s body temperature was Clay Gueits, MD approved for treatment-resistant depression. 37.6°C, and she was diaphoretic. Her blood Previously, researchers believed ketamine pressure was 154/100 mm Hg, and her heart mediated its analgesic and psychotropic rate was 125 bpm. On physical examination, effects solely via N-methyl-d-aspartate she had 4+ patellar and Achilles reflexes (NMDA) receptor antagonism, but emerg- with left ankle clonus and crossed adductors. ing research has described a seemingly more Her mental status exam showed increased complex receptor profile.1 One such ancillary latency of thought and speech, with bizarre pharmacologic mechanism is occupation of affect as evidenced by illogical mannerisms Martin Witkin, DO the serotonin receptor.1,2 However, there and appearance. She said she was “not feel- is sparse literature describing the possible ing myself” and would stare at walls for pro- Dr. Gueits is a PGY-2 Psychiatry extent of ketamine’s involvement in sero- longed periods of time, appearing internally Resident, Department of Psychiatry, tonin syndrome.3 Here, we describe a case preoccupied and confused.