Georgian Harm Reduction Network
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Ports Rail 3
68693 Public Disclosure Authorized Caucasus Transport Corridor for Oil and Oil Products Public Disclosure Authorized Public Disclosure Authorized Prepared by: ECSSD The World Bank Public Disclosure Authorized December 2008 Abbreviations and Acronyms ACG Azeri, Chirag and deepwater Gunashli (oil fields) ADDY Azerbaijan Railway AIOC Azerbaijan International Oil Consortium bpd Barrels per day BTC Baku-Tbilisi-Ceyhan (pipeline) CA or CAR Central Asian Region Caspar Azerbaijan State Caspian Shipping Company CIS Commonwealth of Independent States CNPC China National Petroleum Corporation CPC Caspian Pipeline Consortium (pipeline) dwt Deadweight ton FOB Free on board FSU Former Soviet Union GDP Gross Domestic Product GR Georgian Railway km Kilometer KCTS Kazakhstan Caspian Transport System KMG KazMunaiGaz KMTP Kazmortransflot kV Kilovolt MEP Middle East Petroleum MOU Memorandum of Understanding OECD Organization for Economic Co-operation and Development RTC Rail tank-car RZD Russian Railway SOCAR State Oil Company of Azerbaijan tpa Tons per annum (per year), metric TRACECA Transport Corridor Europe-Caucasus-Asia Vice President, Europe and Central Asia: Shigeo Katsu, ECAVP Country Director: Donna Dowsett-Coirolo, ECCU3 Sector Director: Peter D. Thomson, ECSSD Sector Manager, Transport: Motoo Konishi, ECSSD Task Team Leader: Martha Lawrence, ECSSD I II Table of Contents EXECUTIVE SUMMARY 1. CASPIAN OIL TRANSPORT MARKET DYNAMICS Outlook for Caspian Oil Production Transport Options for Caspian Oil 2. CAUCASUS RAIL CORRIDOR—PHYSICAL CONSTRAINTS Ports -

Georgia Transport Sector Assessment, Strategy, and Road Map
Georgia Transport Sector Assessment, Strategy, and Road Map The Asian Development Bank (ADB) is preparing sector assessments and road maps to help align future ADB support with the needs and strategies of developing member countries and other development partners. The transport sector assessment of Georgia is a working document that helps inform the development of country partnership strategy. It highlights the development issues, needs and strategic assistance priorities of the transport sector in Georgia. The knowledge product serves as a basis for further dialogue on how ADB and the government can work together to tackle the challenges of managing transport sector development in Georgia in the coming years. About the Asian Development Bank ADB’s vision is an Asia and Pacific region free of poverty. Its mission is to help its developing member countries reduce poverty and improve the quality of life of their people. Despite the region’s many successes, it remains home to two-thirds of the world’s poor: 1.7 billion people who live on less than $2 a day, with 828 million struggling on less than $1.25 a day. Georgia Transport Sector ADB is committed to reducing poverty through inclusive economic growth, environmentally sustainable growth, and regional integration. Based in Manila, ADB is owned by 67 members, including 48 from the region. Its main Assessment, Strategy, instruments for helping its developing member countries are policy dialogue, loans, equity investments, guarantees, grants, and technical assistance. and Road Map TRANSPORT AND COMMUNICATIONS. Georgia. 2014 Asian Development Bank 6 ADB Avenue, Mandaluyong City 1550 Metro Manila, Philippines www.adb.org Printed in the Philippines Georgia Transport Sector Assessment, Strategy, and Road Map © 2014 Asian Development Bank All rights reserved. -

Economic Prosperity Initiative
USAID/GEORGIA DO2: Inclusive and Sustainable Economic Growth October 1, 2011 – September 31, 2012 Gagra Municipal (regional) Infrastructure Development (MID) ABKHAZIA # Municipality Region Project Title Gudauta Rehabilitation of Roads 1 Mtskheta 3.852 km; 11 streets : Mtskheta- : Mtanee Rehabilitation of Roads SOKHUMI : : 1$Mestia : 2 Dushet 2.240 km; 7 streets :: : ::: Rehabilitation of Pushkin Gulripshi : 3 Gori street 0.92 km : Chazhashi B l a c k S e a :%, Rehabilitaion of Gorijvari : 4 Gori Shida Kartli road 1.45 km : Lentekhi Rehabilitation of Nationwide Projects: Ochamchire SAMEGRELO- 5 Kareli Sagholasheni-Dvani 12 km : Highway - DCA Basisbank ZEMO SVANETI RACHA-LECHKHUMI rehabilitaiosn Roads in Oni Etseri - DCA Bank Republic Lia*#*# 6 Oni 2.452 km, 5 streets *#Sachino : KVEMO SVANETI Stepantsminda - DCA Alliance Group 1$ Gali *#Mukhuri Tsageri Shatili %, Racha- *#1$ Tsalenjikha Abari Rehabilitation of Headwork Khvanchkara #0#0 Lechkhumi - DCA Crystal Obuji*#*# *#Khabume # 7 Oni of Drinking Water on Oni for Nakipu 0 Likheti 3 400 individuals - Black Sea Regional Transmission ZUGDIDI1$ *# Chkhorotsku1$*# ]^!( Oni Planning Project (Phase 2) Chitatskaro 1$!( Letsurtsume Bareuli #0 - Georgia Education Management Project (EMP) Akhalkhibula AMBROLAURI %,Tsaishi ]^!( *#Lesichine Martvili - Georgia Primary Education Project (G-Pried) MTSKHETA- Khamiskuri%, Kheta Shua*#Zana 1$ - GNEWRC Partnership Program %, Khorshi Perevi SOUTH MTIANETI Khobi *# *#Eki Khoni Tskaltubo Khresili Tkibuli#0 #0 - HICD Plus #0 ]^1$ OSSETIA 1$ 1$!( Menji *#Dzveli -

6. Imereti – Historical-Cultural Overview
SFG2110 SECOND REGIONAL DEVELOPMETN PROJECT IMERETI REGIONAL DEVELOPMENT PROGRAM IMERETI TOURISM DEVELOPMENT STRATEGY Public Disclosure Authorized STRATEGIC ENVIRONMENTAL, CULTURAL HERITAGE AND SOCIAL ASSESSMENT Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Tbilisi, December, 2014 ABBREVIATIONS GNTA Georgia National Tourism Administration EIA Environnemental Impact Assessment EMP Environmental Management Plan EMS Environmental Management System IFI International Financial Institution IRDS Imereti Regional Development Strategy ITDS Imereti Tourism Development Strategy MDF Municipal Development Fund of Georgia MoA Ministry of Agriculture MoENRP Ministry of Environment and Natural Resources Protection of Georgia MoIA Ministry of Internal Affairs MoCMP Ministry of Culture and Monument Protection MoJ Ministry of Justice MoESD Ministry of Economic and Sustaineble Developmnet NACHP National Agency for Cultural Heritage Protection PIU Project Implementation Unit PPE Personal protective equipment RDP Regional Development Project SECHSA Strategic Environmental, Cultural Heritage and Social Assessment WB World Bank Contents EXECUTIVE SUMMARY ........................................................................................................................................... 0 1. INTRODUCTION ........................................................................................................................................... 14 1.1 PROJECT CONTEXT ............................................................................................................................... -
Georgia Program Maps 10/31/2008
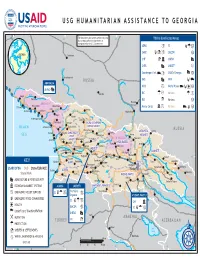
USG HUMANITARIAN ASSISTANCE TO GEORGIA 40° E 42° E The boundaries and names used on this map 44° E T'bilisi & Affected46° E Areas Majkop do not imply official endorsement or acceptance by the U.S. Government. ADRA a SC Ga I GEORGIA CARE a UMCOR a Cherkessk CHF IC UNFAO CaspianA Sea 44° CNFA A UNICEF J N 44° Kuban' Counterpart Int. Ea USAID/Georgia Aa N Karachayevsk RUSSIA FAO A WFP E ABKHAZIA E !0 Psou IOCC a World Vision Da !0 UNFAO A 0 Nal'chik IRC G J Various G a ! Gagra Bzyb' Groznyy RUSSIA 0 Pskhu IRD I Various a ! Nazran "ABKHAZIA" Novvy Afon Pitsunda 0 Omarishara Mercy Corps Ca Various E a ! Lata Sukhumi Mestia Gudauta!0 !0 Kodori Inguri Vladikavkaz Otap !0 Khaishi Kvemo-gulripsh Lentekhi !0 Tkvarcheli Dzhvari RACHA-LECHKHUMI-RACHA-LECHKHUMI- Terek BLACK Ochamchira Gali Tsalenjhikha KVEMOKVEMO SVANETISVANETI RUSSIA Khvanchkara Rioni MTSKHETA-MTSKHETA- Achilo Pichori Zugdidi SAMEGRELO-SAMEGRELO- Kvaisi Mleta SEA ZEMOZEMO Ambrolauri MTIANETIMTIANETI Pasanauri Alazani Khobi Tskhaltubo Tkibuli "SOUTH OSSETIA" Anaklia SVANETISVANETI Aragvi Qvirila SHIDASHIDA KARTLIKARTLI Senaki Kurta Artani Rioni Samtredia Kutaisi Chiatura Tskhinvali Poti IMERETIIMERETI Lanchkhuti Rioni !0 Akhalgori KAKHETIKAKHETI Chokhatauri Zestafoni Khashuri N Supsa Baghdati Dusheti N 42° Kareli Akhmeta Kvareli 42° Ozurgeti Gori Kaspi Borzhomi Lagodekhi KEY Kobuleti GURIAGURIA Bakhmaro Borjomi TBILISITBILISI Telavi Abastumani Mtskheta Gurdzhaani Belokany USAID/OFDA DoD State/EUR/ACE Atskuri T'bilisi Î! Batumi 0 AJARIAAJARIA Iori ! Vale Akhaltsikhe Zakataly State/PRM -

Realizing the Urban Potential in Georgia: National Urban Assessment
REALIZING THE URBAN POTENTIAL IN GEORGIA National Urban Assessment ASIAN DEVELOPMENT BANK REALIZING THE URBAN POTENTIAL IN GEORGIA NATIONAL URBAN ASSESSMENT ASIAN DEVELOPMENT BANK Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) © 2016 Asian Development Bank 6 ADB Avenue, Mandaluyong City, 1550 Metro Manila, Philippines Tel +63 2 632 4444; Fax +63 2 636 2444 www.adb.org Some rights reserved. Published in 2016. Printed in the Philippines. ISBN 978-92-9257-352-2 (Print), 978-92-9257-353-9 (e-ISBN) Publication Stock No. RPT168254 Cataloging-In-Publication Data Asian Development Bank. Realizing the urban potential in Georgia—National urban assessment. Mandaluyong City, Philippines: Asian Development Bank, 2016. 1. Urban development.2. Georgia.3. National urban assessment, strategy, and road maps. I. Asian Development Bank. The views expressed in this publication are those of the authors and do not necessarily reflect the views and policies of the Asian Development Bank (ADB) or its Board of Governors or the governments they represent. ADB does not guarantee the accuracy of the data included in this publication and accepts no responsibility for any consequence of their use. This publication was finalized in November 2015 and statistical data used was from the National Statistics Office of Georgia as available at the time on http://www.geostat.ge The mention of specific companies or products of manufacturers does not imply that they are endorsed or recommended by ADB in preference to others of a similar nature that are not mentioned. By making any designation of or reference to a particular territory or geographic area, or by using the term “country” in this document, ADB does not intend to make any judgments as to the legal or other status of any territory or area. -

Multifunctional Transshipment Terminal at Port of Poti, Georgia Updated Environmental and Social Impact Assessment
TRANSFORD LLC Multifunctional Transshipment Terminal at Port of Poti, Georgia Updated Environmental and Social Impact Assessment Tbilisi 2015 Contents 1 Introduction ................................................................................................................... 7 2 Updated ESIA ............................................................................................................... 8 3 Environmental and Social Objectives of the Report ..................................................... 10 4 Environmental and Social Impact Assessment Methodology ....................................... 10 5 Legal and Regulatory Framework ................................................................................ 11 5.1 Georgian legislation .............................................................................................. 11 5.2 Environmental Standards in Georgia .................................................................... 15 5.3 Environmental Impact Assessment in Georgia ..................................................... 17 5.4 IFC Performance Standards ................................................................................. 18 5.5 International Conventions ..................................................................................... 19 5.6 Marine sediment quality guidelines ....................................................................... 20 5.7 Gaps between Georgian legislation and IFC requirements ................................... 21 6 Project Description ..................................................................................................... -

Investment Opportunities in Manufacturing of Apparel Footwear
INVESTMENT OPPORTUNITIES IN MANUFACTURING OF APPAREL, FOOTWEAR AND BAGS IN GEORGIA 2019 GEORGIA COUNTRY OVERVIEW Area: 69,700 sq. km Population: 3.7 mln GDP 2018: USD 16.2 billions Life expectancy at GDP real growth rate 2018: 4.7 % birth 2018: 74 years GDP CAGR 2013-2018 (GEL): Georgian 4 % GDP per capita 2018: Literacy: 99.8 % USD 4346 Inflation rate (December) 2018 (Y-o-Y): 1.5% Capital: Tbilisi Total Public Debt to Nominal GDP (%) 2018: 42.2% Currency (code): Lari (GEL) INVESTMENT CLIMATE & 2 OPPORTUNITIES IN GEORGIA OVERVIEW OF MANUFACTURING SECTOR Georgia has a rich history of Contract manufacturing of apparel Footwear and bags manufacturing manufacturing apparel, textile is well developed in Georgia and sector has emerged recently and and footwear, dating back to existing factories produce apparel local manufacturers have started to Soviet times for famous international brands, export their products to different such as Moncler, Tommy Hilfiger, international markets Nike, Adidas, Mexx, Zara, Puma, Autograph, Lebek, Hawes & Curtis, M&S, HM, etc. In addition, leather production is also developing in Georgia and Georgian leather is already being exported to Italy and Turkey RUSSIA Zugdidi Anaklia BLACK Poti SEA Samtredia Batumi Ozurgeti Existing clusters Thriving locations TURKEY Main Roads ARMENIA AZERBAIJAN APPAREL BRANDS CURRENTLY PRODUCED IN GEORGIA Source: Geostat; KPMG Note: *-preliminary data INVESTMENT OPPORTUNITY 3 OF MANUFACTURING FOOTWEAR AND BAGS IN GEORGIA LIBERAL TRADE REGIMES Very simple and service oriented customs -

ANALYSIS of EMPLOYMENT and UNEMPLOYMENT in MUNICIPALITIES of GEORGIA (Target Municipalities: Lentekhi, Oni, Ambrolauri, Tskaltubo, Samtredia, Tsageri)77
European Scientific Journal December 2015 /SPECIAL/ edition Vol.2 ISSN: 1857 – 7881 (Print) e - ISSN 1857- 7431 ANALYSIS OF EMPLOYMENT AND UNEMPLOYMENT IN MUNICIPALITIES OF GEORGIA (Target municipalities: Lentekhi, Oni, Ambrolauri, Tskaltubo, Samtredia, Tsageri)77 Murtaz Kvirkvaia, Professor Grigol Robakidze University, Tbilisi, Georgia Abstract The article includes detailed employment and uniploymant analysis in each municipality. In the analysis we use results from household survey conducted by the National Statistics Service. More specific information about the labour market at the municipal level was collected through cooperation with local municipalities. For the analysis we used information from municipalities’ web pages, telephone conversations with stakeholders, personal meetings with experts and so on. It should also be noted that a certain part of the data obtained from municipalities and from administrative territorial units have an approximate nature, but based on these information it is possible to gain some valuable conclusions and make assumptions. Terms and reality of employment analysis is carried out not only at the level of the municipality but on the country and regional ones as well. Keywords: Labor market; Unemployment; Employment analysis; local municipalities; Economically Active population; Self-employed; Integrated household survey Introduction The target municipalities (Lentekhi, Oni, Ambrolauri, Tskaltubo, Samtredia, Tsageri) are located in specific regions of Georgia. For example, a municipality of Samtredia and Tskaltubo are in Imereti region, and the other four target municipalities are in Racha-Lechkhumi and Kvemo Svaneti region. For the evaluation of the general situation we consider the labor statistics on the country and regional level. Originally a brief analysis of the 77 This analysis was done under the UNDP/AF project. -

Georgian Economic Outlook
Georgian Economic Outlook Ministry of Economic Development of Georgia Country Overview Area: 69 700 sq km Population 2008 E: 4 630 841 Life expectancy: 76.51 years Official language: Georgian Literacy: 100% Capital: Tbilisi Currency (code): Lari (GEL) GDP 2008E: US$ 12.80 billion GDP - real growth rate 2008E: 2.1% GDP - Per Capita 2008 US$ 2 920.3 Inflation rate 2008 (average annual): 10.0% External debt to GDP 2008: 21.4% Ministry of Economic Development of Georgia Liberal Reforms for Long Term Sustainable Growth • Liberal Tax Code Only 6 taxes left Significant procedural and institutional reforms Simplified system of tax disputes discussion • Customs Reform Simplified customs procedures Simplified and sharply reduced the costs connected to the foreign trade Number of import tariffs were abolished on approximetaly 90% of products 3 tariff rates (0%, 5%, 12%) remained No quantitative restrictions (quotas) on imports and exports • Modernized system of Licenses and Permits Number of licenses and permits reduced by 84% Licenses and permits are only used in the production of highly risky goods and services, usage of natural resources and other specific activities Significantly simplified procedures of issuing licenses and permits Introduced “one-stop shop” and “silence is consent” principles Ministry of Economic Development of Georgia Liberal Reforms for Long Term Sustainable Growth • The reform of Technical Regulation System National mandatory standards system was replaced by the voluntary standards, giving entrepreneurs the -

Developments at Georgian Railway
Feature Developments at Georgian Railway Developments at Georgian Railway Teimuraz Gorshkov and George Bagaturia proposed in the 1830s when it was it was shipped to world markets. The last History of Georgian Railway realized that a railway from Poti on the major line between Georgia and Armenia Black Sea to Tbilisi (the capital of Georgia) was opened in 1899. Georgian Railway (GRW) Ltd. is located could carry a great deal of the trade Rapid development of Georgian industry in the South Caucasus at a key point on between northern Iran and Europe, and agriculture between 1924 and 1940 the ancient Silk Road between Europe and especially since it would be only half as was followed by construction of new Asia (Fig. 1). The Silk Road was more than long as a railway through Turkey. branch lines throughout the Georgian a trade route—it was a conduit for Construction of the first Trans-Caucasus regions. A connection with the Russian exchange of knowledge and culture that line started in 1865 and the first passenger railway network was begun during WWII contributed to the development of all train from Poti arrived at Tbilisi on 10 and opened in 1946 despite the war. countries in the region. Today’s GRW October 1872, marking the birth of GRW. Completion of the network between Baku, network has a similar function to the Silk The first trains covered the 310-km Tbilisi, and Batumi had a positive effect Road by serving as a transport artery journey in 15 hours. The next 20 years on the economies of Georgia and the linking the Black and Caspian seas. -

Highway E60 Samtredia – Grigoleti
iC group of companies Highway E60 Samtredia – Grigoleti Client: Project objectives Roads Department of the Ministry of Regional For the promotion of trade with the neighbouring countries and the Development and Infrastructure of Georgia development of tourism infrastructures the Georgian Government has given the highest priority to the East-West highway between the Caspian Sea and the Country: Black Sea. With funding from the European Investment Bank the construction Georgia supervision ensures that high quality construction is achieved and all works are carried out according to the engineering designs and works contracts. Duration: Project description From August 2013 to March 2021 Site supervision and technical assistance in the role of the FIDIC Engineer for the new construction of the highway section connecting the capital Tbilisi with the Services: Black Sea ports and cities of Batumi and Poti. Site supervision under FIDIC Project data The highway works for the dual carriageway with two lanes in each direction and a length of 60 km include one viaduct of 900 m length over the Rioni river valley, eight interchanges, 19 bridges, two overpasses and 189 underpasses. Project specifics Demanding geotechnical conditions along the alignment towards the black Sea cause massive settlements and led to changes in design and construction with soil improvement by means of vertical drains with a length of approximately ten million metres. The impact of the design changes on four construction contracts and the changed sequence of construction works