Research Article Alpha-Thalassemia in North Morocco: Prevalence and Molecular Spectrum
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clashes Erupt on Morocco Border As Madrid Accuses Rabat of Blackmail Spain Moves Quickly to Return Most of the Migrants Who Reached Ceuta
Friday 15 International Friday, May 21, 2021 Clashes erupt on Morocco border as Madrid accuses Rabat of blackmail Spain moves quickly to return most of the migrants who reached Ceuta FNIDEQ, Morocco: Spain accused Morocco of “blackmail” yes- “it is not acceptable to put the lives of minors or of people of terday for allowing a record 8,000 migrants to reach the Spanish one’s own country, at risk.” North African enclave of Ceuta, sparking a crisis that saw clashes on the Moroccan side of the border overnight. Spanish authori- ‘I will try my luck again’ ties were caught by surprise on Monday when large numbers of Spain’s government said that around 5,600 of the 8,000 mi- mostly young people began swimming or using small inflatable grants had already been sent back, and there were no new entries boats to cross the frontier as the Moroccan border forces looked on Wednesday as anyone who reached Ceuta’s beach was imme- the other way, quickly leaving the tiny territory overwhelmed. diately returned. Some of the returned migrants said they hoped But Madrid moved quickly to return most of the migrants and to try cross over into Ceuta again if border controls were eased calm has largely returned the Spanish beach of Tarajal in Ceuta, once more. “I have no future here, I want to work to help my fam- where soldiers and armored vehicles have been deployed in ily,” 17-year-old Mohamed told AFP in Fnideq after being re- large numbers. turned from Ceuta. He left his studies and his family in Morocco The outskirts of the Moroccan border town of Fnideq were to try to enter Spain in search of a better life. -
V.4 Parta Compressed
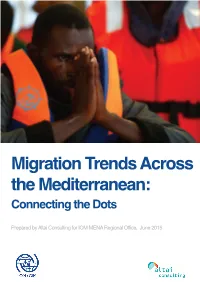
Migration Trends Across the Mediterranean: Connecting the Dots Prepared by Altai Consulting for IOM MENA Regional Office, June 2015 This report was prepared, researched, and written by Arezo Malakooti (Project Director), under the supervision of Eric Davin (Altai Partner). All field research was managed and conducted by Arezo Malakooti, with the exception of fieldwork with migrants in Libya, which was carried out by Altai’s local partner, Istishari Consulting. Assistance was also provided by Tahar Benattia, Marie-Cecile Darme, Souad Chatar and Matthew Burnard (all from Altai Consulting). We gratefully acknowledge IOM’s Middle East and North Africa Regional Office (Cairo) for its role in designing and framing this study, as well IOM country offices in Egypt, Italy, Libya, Malta, Morocco, Spain and Tunisia for their valuable input and assistance. UNHCR offices in all of the above-mentioned countries are also gratefully acknowledged for their time and expertise. We are also indebted to the numerous migrants, government representatives, humanitarians/aid workers, academic researchers and community members who shared their views on the various themes that this study covers. The image on the front cover of this report was graciously provided by the Migrant Offshore Aid Station (MOAS.eu)/ Darrin Zammit Lupi. Layout and graphic design by Marie-Cecile Darme. Altai Consulting provides strategy consulting and research services to private companies, governments and public institutions. Altai teams operate in more than 25 countries in Africa, the Middle East, Central Asia and Europe. Since its inception 12 years ago, Altai Consulting has developed a strong focus on migration and labour market related research and program evaluations. -

Leishmaniasis in Northern Morocco: Predominance of Leishmania Infantum Compared to Leishmania Tropica
Hindawi BioMed Research International Volume 2019, Article ID 5327287, 14 pages https://doi.org/10.1155/2019/5327287 Research Article Leishmaniasis in Northern Morocco: Predominance of Leishmania infantum Compared to Leishmania tropica Maryam Hakkour ,1,2,3 Mohamed Mahmoud El Alem ,1,2 Asmae Hmamouch,2,4 Abdelkebir Rhalem,3 Bouchra Delouane,2 Khalid Habbari,5 Hajiba Fellah ,1,2 Abderrahim Sadak ,1 and Faiza Sebti 2 1 Laboratory of Zoology and General Biology, Faculty of Sciences, Mohammed V University in Rabat, Rabat, Morocco 2National Reference Laboratory of Leishmaniasis, National Institute of Hygiene, Rabat, Morocco 3Agronomy and Veterinary Institute Hassan II, Rabat, Morocco 4Laboratory of Microbial Biotechnology, Sciences and Techniques Faculty, Sidi Mohammed Ben Abdellah University, Fez, Morocco 5Faculty of Sciences and Technics, University Sultan Moulay Slimane, Beni Mellal, Morocco Correspondence should be addressed to Maryam Hakkour; [email protected] Received 24 April 2019; Revised 17 June 2019; Accepted 1 July 2019; Published 8 August 2019 Academic Editor: Elena Pariani Copyright © 2019 Maryam Hakkour et al. Tis is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In Morocco, Leishmania infantum species is the main causative agents of visceral leishmaniasis (VL). However, cutaneous leishmaniasis (CL) due to L. infantum has been reported sporadically. Moreover, the recent geographical expansion of L. infantum in the Mediterranean subregion leads us to suggest whether the nonsporadic cases of CL due to this species are present. In this context, this review is written to establish a retrospective study of cutaneous and visceral leishmaniasis in northern Morocco between 1997 and 2018 and also to conduct a molecular study to identify the circulating species responsible for the recent cases of leishmaniases in this region. -

4. Impact on Agriculture
ReportNo. 15808-MOR Kingdom of Morocco Impact Evaluation Report Public Disclosure Authorized Socioeconomic Influence of Rural Roacds FoL:ulth High\vav\ Project [ oarn 2254-N( )PR June28, 1996 (iperition El%sEEalLation1 De)artnmen1t Public Disclosure Authorized Public Disclosure Authorized Document of the World Bank Public Disclosure Authorized Currency Equivalents Currency Unit = Dirham (Dh) US$1 = 8.63 Dh Abbreviations and Acronyms douars Hamlet or section of a larger village DRCR Directorate of Road and Road Traffic GDP Gross Domestic Product HDM Highway Design Model MLSS Morocco Living Standards Survey MPW Ministry of Public Works qx 100 Kilograms SUNABEL Sugar Factory VOC Vehicle Operating Costs The WorldBank Washington, D.C. 20433 U.S.A. Officeof the Director-General Operations Evaluation June 28, 1996 MEMORANDUlM TO THE EXECUTIVE DIRECTORS AND THE PRESIDENT SUBJECT: Impact Evaluation Report on Morocco Socioeconomic Influence of Rural Roads Fourth Highway Project (Loan 2254-MOR) Attached is the Impact Evaluation Report (IER) on the Morocco Fourth Highway project (Loan 2254, approved in FY83). The main objective of the impact evaluation was to understand the impact of rural roads, five to ten years after completion of the improvements carried out under the project. The study focused on impacts on: (i) transport infrastructure and services; (ii) agriculture; (iii) social services; and (iv) the environment. The impact study also assessed the economic benefits of the improvements and their sustainability. The study focused on four of the ten rural roads improved under the project; the sample roads were geographically distributed in the North, Center and Center-South of the country to represent a variety of climate, agricultural, and economic conditions. -

Estimation of Road's Exposure to Floods in the Province of Larache
ogy eol & G OPEN ACCESS Freely available online G e f o o p l h a y s n r i c u Journal of Geology & Geophysics s o J ISSN: 2381-8719 Research Article Estimation of Road’s Exposure to Floods in the Province of Larache, Morocco Meryem El Boukhari1*, Saida El Moutaki1, Abdessamad Ghafiri1, Hassan Oulidi Jarar2 and Khalid El Ouardi3 1Laboratory of Applied Geology, Geomatic and Environment, Ben Msick Faculty of Sciences, Hassan II University of Casablanca, Morocco; 2Hassania School of Public Works, Casablanca, Morocco; 3Mapping Technologies, Consulting Engineers Office, Rabat, Morroco ABSTRACT Generally, the road infrastructure suffers from significant damage caused by natural disasters (flood, earthquake, etc.). In particular, the Kingdom of Morocco experienced several interruptions of the road network during previous floods. In this sense, paper presents a new method for estimating the exposure’s degree of the road infrastructure to the risk of flooding. This method has been applied to the province of Larache. Based on the flood history, a model is developed to define areas exposed to flood hazard and deduce the exposure’s degree of each road to floods. Several results are obtained allowing a detailed mapping of flood risk in the province of Larache. Keywords: Flood hazard; Road network; Exposure; Larache; Mapping INTRODUCTION of exposure: high or moderate. While [13] derives the flood risk map from the geographical representation of the estimated water Flooding is a natural phenomenon that affects a portion of depth, and defines three levels of flood exposure: low, moderate the territory and creates risk for installations and humans [1]. -

Morocco and United States Combined Government Procurement Annexes
Draft Subject to Legal Review for Accuracy, Clarity, and Consistency March 31, 2004 MOROCCO AND UNITED STATES COMBINED GOVERNMENT PROCUREMENT ANNEXES ANNEX 9-A-1 CENTRAL LEVEL GOVERNMENT ENTITIES This Chapter applies to procurement by the Central Level Government Entities listed in this Annex where the value of procurement is estimated, in accordance with Article 1:4 - Valuation, to equal or exceed the following relevant threshold. Unless otherwise specified within this Annex, all agencies subordinate to those listed are covered by this Chapter. Thresholds: (To be adjusted according to the formula in Annex 9-E) For procurement of goods and services: $175,000 [Dirham SDR conversion] For procurement of construction services: $ 6,725,000 [Dirham SDR conversion] Schedule of Morocco 1. PRIME MINISTER (1) 2. NATIONAL DEFENSE ADMINISTRATION (2) 3. GENERAL SECRETARIAT OF THE GOVERNMENT 4. MINISTRY OF JUSTICE 5. MINISTRY OF FOREIGN AFFAIRS AND COOPERATION 6. MINISTRY OF THE INTERIOR (3) 7. MINISTRY OF COMMUNICATION 8. MINISTRY OF HIGHER EDUCATION, EXECUTIVE TRAINING AND SCIENTIFIC RESEARCH 9. MINISTRY OF NATIONAL EDUCATION AND YOUTH 10. MINISTRYOF HEALTH 11. MINISTRY OF FINANCE AND PRIVATIZATION 12. MINISTRY OF TOURISM 13. MINISTRY OF MARITIME FISHERIES 14. MINISTRY OF INFRASTRUCTURE AND TRANSPORTATION 15. MINISTRY OF AGRICULTURE AND RURAL DEVELOPMENT (4) 16. MINISTRY OF SPORT 17. MINISTRY REPORTING TO THE PRIME MINISTER AND CHARGED WITH ECONOMIC AND GENERAL AFFAIRS AND WITH RAISING THE STATUS 1 Draft Subject to Legal Review for Accuracy, Clarity, and Consistency March 31, 2004 OF THE ECONOMY 18. MINISTRY OF HANDICRAFTS AND SOCIAL ECONOMY 19. MINISTRY OF ENERGY AND MINING (5) 20. -

Activité 2: Aménagement Du Territoire Dans Un Contexte De Haut Risque
Document V1.0 Actions de la Fondation Ayesa au titre de l’activité 2 PRAVEMA Activité 2: Aménagement du territoire dans un contexte de haut risque Action 1: Définition du contexte de haut risque pour la population TABLE DES MATIERES 1. Introduction................................................................................. 1 2. Portée de l'étude. .......................................................................... 2 2.1. Critères de délimitation de la zone d'étude. .............................................. 3 2.2. Etude hydraulique simplifiée............................................................... 4 2.3. Zones du bassin historiquement inondables. ............................................. 6 2.4. Délimitation de la zone d'étude............................................................ 8 3. Organisation administrative................................................................ 9 3.1. Démographie ............................................................................. 10 3.2. Données socioéconomiques ............................................................. 15 4. Définition des contextes à haut risque d'inondation pour la population. ............. 23 5. Utilisation du sol.......................................................................... 29 5.1. Agglomérations principales. Larache et Ksar el Kébir. .................................. 36 5.2. Terrains inondables de l'Oued Loukkos entre le barrage Oued El Makhazine et son embouchure à Larache. ............................................................................... -

Report of the Sustainable Ocean Initiative Regional Capacity-Building Workshop for Northern Africa and the Mediterranean
CBD Distr. GENERAL CBD/SOI/WS/2018/3/2 29 January 2019 ENGLISH/FRENCH ONLY SUSTAINABLE OCEAN INITIATIVE CAPACITY- BULDING WORKSHOP FOR NORTHERN AFRICA AND THE MEDITERRANEAN Tangier, Morocco, from 15-19 October 2018 REPORT OF THE SUSTAINABLE OCEAN INITIATIVE REGIONAL CAPACITY-BUILDING WORKSHOP FOR NORTHERN AFRICA AND THE MEDITERRANEAN INTRODUCTION 1. The Conference of the Parties to the Convention on Biological Diversity, at its tenth meeting, adopted the Strategic Plan for Biodiversity 2011-2020, with its Aichi Biodiversity Targets (see decision X/2). The mission of the Strategic Plan is to take effective and urgent action to halt the loss of biodiversity in order to ensure that, by 2020, ecosystems are resilient and continue to provide essential services, thereby securing the planet’s variety of life, and contributing to human well-being and poverty eradication. 2. Recognizing this urgent need for training and capacity-building for developing country Parties, the Sustainable Ocean Initiative (SOI) came into existence in the margins of the tenth meeting of the Conference of the Parties, with the support of Japan, and in collaboration with various partners that were willing to provide the necessary expertise, technical and financial resources. The execution of SOI activities is coordinated by the Secretariat of the Convention on Biological Diversity. 3. SOI focuses on achieving a balance between conservation and sustainable use of marine and coastal biodiversity by applying an action-oriented, holistic and integrated capacity-building -

Bluetongue in Morocco 2004 to 2015
ISSN: 2474-3658 Youssef L et al. J Infect Dis Epidemiol 2017, 3:023 DOI: 10.23937/2474-3658/1510023 Volume 3 | Issue 1 Journal of Open Access Infectious Diseases and Epidemiology OVERVIEW ARTICLE Bluetongue in Morocco 2004 to 2015: An Overview Lhor Youssef1*, Kyriaki Nomikou2, Khayli Mounir1, Bouslikhane Mohammed3, Fassi Fihri Ouafaa3 and El Harrak Mehdi4 1National Office of Food Safety (ONSSA), Rabat, Morocco 2Vector-Borne Viral Diseases Programme, The Pirbright Institute, United Kingdom 3Institut Agronomique et vétérinaire Hassan II, Rabat, Morocco 4MCI Santé Animale, Morocco *Corresponding author: Lhor Youssef, National Office of Food Safety (ONSSA), Rabat, Morocco, E-mail: [email protected] Abstract Introduction Bluetongue (BT) is an infectious, arthropod borne viral disease With 18 million sheep, 5 million goats and 3.3 million of domestic and wild ruminants. BT is a notifiable disease of cattle, livestock represents the main livelihood for the huge socio-economic concern and of major importance in majority of the rural population in Morocco and plays the international trade of animals and animal products. Due to the segmented nature of genome, there is existence of a crucial role at both national and household levels. high diversity in BT virus serotypes too as a consequence of Over the year, Morocco enjoys a Mediterranean soft genetic reassortments. Until 2004, BT was considered as an climate in the green belt part of the country between exotic disease in Morocco. However, from 2004 to 2015, at the Mediterranean Sea in the North, the Atlantic Ocean least two BTV serotypes (BTV-1 and BTV-4) were reported in the West and Atlas Mountains in the Southeast. -
Geopolitical Overview of Conflicts 2016
Geopolitical overview of Spanish Institute for conflicts 2016 Strategic Studies MINISTERIO DE DEFENSA Geopolitical overview Spanish Institute for of conflicts 2016 Strategic Studies MINISTERIO DE DEFENSA SPANISH OFFICIAL PUBLICATIONS CATALOGUE http://publicacionesoficiales.boe.es Edita: SECRETARÍA GENERAL TÉCNICA http://publicaciones.defensa.gob.es/ © Author and Publisher, 2017 NIPO: 083-16-308-8 (print on demand) NIPO: 083-16-309-3 (e-book edition) Publication date: september 2017 The authors are solely responsible for the opinions expresed in the articles in this publication. The exploitation righits of this work are protected by the Spanish Intellectual Property Act. No parts of this publication may be produced, stored or transmitted in any way nor by any means, electronic, mechanical or print, including photo- copies or any other means without prior, express, written consent of the © copyright holders. ÍNDEX Page Introduction The role of the major powers in current conflicts ...................................................... 9 Miguel Ángel Ballesteros Martín Conflict trends ............................................................................................................................... 9 The resolutions of the Security Council as a gauge of its activity ...................................... 11 Russia’s comeback as a world power ...................................................................................... 13 The military policy of China as an emerging power ............................................................. -

DGAP Report Morocco Violence Extremism
German Council on Foreign Relations No. 4 January 2020 – first published in REPORT July 2019 Edited Volume Socio-Economic Development and Violent Extremism in Morocco Morocco’s Regional Policy, Migration and (De-)Radicalization – Policy Briefs from the Region and Europe Edited by Laura Lale Kabis-Kechrid 2 No. 4 | January 2020 – first published in July 2019 Socio-Economic Development and Violent Extremism in Morocco REPORT The following papers were written by participants of the workshop “Promotion of Think Tank Work on Violent Extremism and Morocco’s Regional Policy in Sub-Sahara Africa as well as the MENA Region” organized by the German Council on Foreign Relations’ Middle East and North Africa Program in the winter of 2018 and spring of 2019 in cooperation with the Rabat Social Studies Institute (RSSI). The workshop is part of the program’s project on the promotion of think tank work in the Middle East and North Africa, which aims to strengthen the scientific and technical capacities of civil society actors in the region and the EU who are engaged in research and policy analysis and advice. It is realized with the support of the German Federal Foreign Office and the Institute for Foreign Cultural Relations (ifa e.V.). The content of the papers does not reflect the opinion of the DGAP. Responsibility for the information and views expressed herein lies entirely with the authors. The editorial closing date was March 31, 2019. Authors: Clarisse Anceau, Tachfine Baida, Hamdi Echkaou, Meriem El Haitami, Abdelouahed Eloufir, Ingrid Heidlmayr-Chegdaly, Salim Hmimnat, Zilvinas Svedkauskas, and Lisa Watanabe Edited by Laura Lale Kabis-Kechrid No. -

Dossier Salubrité Et Sécurité Dans Les Bâtiments : Quel Règlement ?
N°30 / Mars 2015 / 30 Dh Dossier Salubrité et Sécurité dans les bâtiments : Quel règlement ? Architecture et Urbanisme L’urbanisme dans les 12 régions: Quelle vision ? Décoration d’Intérieur et Ameublement Cuisine: Quelles tendances déco 2015? Interview: Salon Préventica International : Une 2ème édition qui promet un grand nombre de Eric Dejean-Servières, commissaire nouveautés général, du salon Préventica International Casablanca Édito N°30 / Mars 2015 / 30 Dh Dossier Salubritéles et bâtiments Sécurité :dans Jamal KORCH Quel règlement ? Architecture et Urbanisme L’urbanisme dans les 12 régions: Quelle vision ? Décoration d’Intérieur et Ameublement Cuisine: Quelles tendances déco 2015? L’aménagement du territoire et le découpage Interview: Salon Préventica International : Une 2ème édition administratif : Y a-t-il une convergence ? qui promet un grand nombre de nouveautés al Eric Dejean-Servières,Casablanca commissaire général, du salon Préventica Internation e pas compromettre les n 2-15-40 fixant à 12 le nombre des Directeur de la Publication besoins des générations régions, leur dénomination, leur chef- Jamal KORCH futures, prendre en compte lieu, ainsi que les préfectures et les l’ensemble des efforts provinces qui les composent. Et sur ce Rédacteur en Chef N environnementaux des activités tracé que l’aménagement du territoire Jamal KORCH urbaines, assurer l’équilibre entre aura lieu en appliquant le contenu des [email protected] les habitants de la ville et ceux de différents documents y afférents. GSM: 06 13 46 98 92 la campagne,