Insert Document Title
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annual Report 20 07 Aviation Industry Association of New Zealand (Inc) Contents
AVIATION INDUSTRY ASSOCIATION OF NEW ZEALAND (INC) Annual Report 20 07 Aviation Industry Association of New Zealand (Inc) Contents General Association Officers 2 Past Officers/Life Members 3 President’s Report 5 Chief Executive Officer’s Report 13 Financial Statements 18 AIA Annual Conference Report 28 Aviation Training Report 52 Aviation Services Ltd 55 AIRCARE Annual Report 2007 57 List of Advertisers 60 Divisional Chair Reports NZAAA (Agricultural Aviation) 31 Air Rescue/Air Ambulance 34 Air Transport 35 Education and Research 37 Engineering 38 Flight Training 40 Annual Report Helicopter 42 Supply & Services 44 Tourist Flight Operators 49 20 Cover Photo: The Auckland Rescue Helicopter Trust’s BK117B2 ZK HLN over central Auckland being flown by the Trust’s Chief Pilot Dave Walley. The Single Pilot IFR, NVG Configured helicopter came into service with the Trust on 01January 2007 and completed its 300 hr check 01 July 2007. 07 ANNUAL REPORT 2007 2 Association Officers 2006–2007 Council Head Office President: Chief Executive: W.J. Funnell, Helicopter Services BOP Ltd I.S. King Vice-Presidents: W.P. Taylor, Eagle Airways Ltd Office Manager: W. Sattler, Ardmore Flying School Ltd P.A. Hirschman Immediate Past President: Membership Liaison Manager: D. Thompson, Dennis Thompson International Ltd D. Watson Councillors Technical Advisors: J. McGregor M. Chubb J. Lusty K. MacKenzie D. Webb B. Wyness P. Garden D. Lyon D. Morgan R. Wikaira F. Douglas D. Horrigan P. Mackay A. Peacock NZAAA Executive Officer: Divisional and Branch Chair J.F. Maber Agricultural Aviation Division Office Address: Chair: K.J. MacKenzie, MacKenzie Aviation Ltd Level 5 Deputy Chair & South Island Branch Chair: Agriculture House T. -

What Options Were Considered
What options were considered As part of the initial planning for the new runway, several options were identified and assessed before determining that the new runway is the most appropriate development to meet the future demand for air services for Perth. Planning Location for the new runway identified in the 1970s by a joint Commonwealth and State Government Committee Support growth Providing essential transport infrastructure capacity and supporting WA’s economic development Connecting people and places Furthering Western Australia’s social and cultural development and connecting WA to the world The new runway represents the best option to support the international competitiveness of the State’s critical export industries, including resources, tourism, international study and agriculture. When do we need a How is the new new runway? runway funded? The need for an additional runway at Perth Airport was Perth Airport is located on approximately 2,105 hectares of land owned by the first recommended more than 40 years ago by a joint Commonwealth of Australia. Commonwealth and State Government Committee In 1997, the airport was privatised investigating Perth’s planning requirements. under a long term lease with oversight remaining with the Commonwealth of Recent modelling shows that an additional runway is needed to meet Australia. Perth Airport is operated by the demand of intrastate, interstate and international services to and Perth Airport Pty Ltd, which is a wholly from Perth. The need for the new runway is driven by the demand for owned subsidiary of Perth Airport arrivals and departures in a given hour. Development Group Pty Ltd (PADG). -

State Planning Policy 5.3 Land Use Planning in the Vicinity of Jandakot Airport
State Planning Policy 5.3 Land Use Planning in the Vicinity of Jandakot Airport January 2017 Prepared under Part Three of the Planning and Development Act 2005 by the Western Australian Planning Commission click to follow 1. CITATION 1 APPENDIX 1 - BUILDING SITE ACCEPTABILITY 9 2. INTRODUCTION AND BACKGOUND 1 APPENDIX 2 2.1 Importance of - INDOOR DESIGN SOUND Disclaimer Jandakot Airport 1 This document has been produced by the LEVELS 10 Department of Planning on behalf of the 2.2 Aircraft noise Western Australian Planning Commission. Any measurement 1 APPENDIX 3: representation, statement, opinion or advice 2.3 Australian Noise NOTIFICATION ABOUT expressed or implied in this publication is Exposure Forecast 1 made in good faith and on the basis that the AIRCRAFT NOISE TO BE Government, its employees and agents are 2.4 Policy measures 1 PLACED ON PROPERTY TITLE 11 not liable for any damage or loss whatsoever which may occur as a result of action taken 3. APPLICATION or not taken, as the case may be, in respect FIGURE 1: FRAME AREA 12 of any representation, statement, opinion or OF THE POLICY 1 advice referred to herein. Professional advice 3.1 Other policies that should be obtained before applying the relate to this policy 1 GLOSSARY OF TERMS 13 information contained in this document to particular circumstances. 4. POLICY OBJECTIVES 2 REFERENCES 13 © Western Australian Planning Commission 5. POLICY MEASURES 2 Published by the Western Australian Planning Commission 5.1 Interpretation 2 Gordon Stephenson House 140 William Street 5.2 Areas below 20 ANEF 2 Perth WA 6000 5.3 Areas between 20 Locked Bag 2506 ANEF and 25 ANEF 3 Perth WA 6001 5.4 Areas above 25 ANEF 4 Published January 2017 6. -

Change 3, FAA Order 7340.2A Contractions
U.S. DEPARTMENT OF TRANSPORTATION CHANGE FEDERAL AVIATION ADMINISTRATION 7340.2A CHG 3 SUBJ: CONTRACTIONS 1. PURPOSE. This change transmits revised pages to Order JO 7340.2A, Contractions. 2. DISTRIBUTION. This change is distributed to select offices in Washington and regional headquarters, the William J. Hughes Technical Center, and the Mike Monroney Aeronautical Center; to all air traffic field offices and field facilities; to all airway facilities field offices; to all international aviation field offices, airport district offices, and flight standards district offices; and to the interested aviation public. 3. EFFECTIVE DATE. July 29, 2010. 4. EXPLANATION OF CHANGES. Changes, additions, and modifications (CAM) are listed in the CAM section of this change. Changes within sections are indicated by a vertical bar. 5. DISPOSITION OF TRANSMITTAL. Retain this transmittal until superseded by a new basic order. 6. PAGE CONTROL CHART. See the page control chart attachment. Y[fa\.Uj-Koef p^/2, Nancy B. Kalinowski Vice President, System Operations Services Air Traffic Organization Date: k/^///V/<+///0 Distribution: ZAT-734, ZAT-464 Initiated by: AJR-0 Vice President, System Operations Services 7/29/10 JO 7340.2A CHG 3 PAGE CONTROL CHART REMOVE PAGES DATED INSERT PAGES DATED CAM−1−1 through CAM−1−2 . 4/8/10 CAM−1−1 through CAM−1−2 . 7/29/10 1−1−1 . 8/27/09 1−1−1 . 7/29/10 2−1−23 through 2−1−27 . 4/8/10 2−1−23 through 2−1−27 . 7/29/10 2−2−28 . 4/8/10 2−2−28 . 4/8/10 2−2−23 . -

Aviation Safety Investigation Report 200303579
AVIATION SAFETY INVESTIGATION 200303579 Cessna 404, VH-ANV Jandakot Airport, WA 11 August 2003 Released under the provisions of the Transport Safety Investigation Act 2003. Front cover photo by George Canciani © ISBN 1 877071 92 7 March 2005 This report was produced by the Australian Transport Safety Bureau (ATSB), PO Box 967, Civic Square ACT 2608. Readers are advised that the ATSB investigates for the sole purpose of enhancing safety. Consequently, reports are confined to matters of safety significance and may be misleading if used for any other purpose. As ATSB believes that safety information is of greatest value if it is passed on for the use of others, copyright restrictions do not apply to material printed in this report. Readers are encouraged to copy or reprint for further distribution, but should acknowledge ATSB as the source. ii CONTENTS INTRODUCTION vii EXECUTIVE SUMMARY viii 1 FACTUAL INFORMATION 1 1.1 History of the flight 1 1.2 Injuries to persons 2 1.3 Damage to aircraft 3 1.4 Other damage 3 1.5 Personnel information 3 1.6 Aircraft information 3 1.6.1 Aircraft certification 4 1.6.2 Recent maintenance history 4 1.6.3 Engine and propeller information 4 1.6.4 Fuel system information 4 1.6.5 Quality of the fuel 5 1.6.6 Aircraft flight controls & associated systems information 6 1.6.7 Aircraft operating weight 6 1.6.8 Aircraft equipment configuration 7 1.7 Meteorological information 7 1.8 Aids to navigation 7 1.9 Communications 7 1.10 Aerodrome information 8 1.10.1 General 8 1.10.2 Runway 24R information 8 1.10.3 Published -
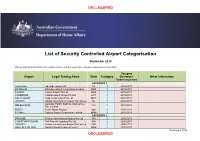
Airport Categorisation List
UNCLASSIFIED List of Security Controlled Airport Categorisation September 2018 *Please note that this table will continue to be updated upon new category approvals and gazettal Category Airport Legal Trading Name State Category Operations Other Information Commencement CATEGORY 1 ADELAIDE Adelaide Airport Ltd SA 1 22/12/2011 BRISBANE Brisbane Airport Corporation Limited QLD 1 22/12/2011 CAIRNS Cairns Airport Pty Ltd QLD 1 22/12/2011 CANBERRA Capital Airport Group Pty Ltd ACT 1 22/12/2011 GOLD COAST Gold Coast Airport Pty Ltd QLD 1 22/12/2011 DARWIN Darwin International Airport Pty Limited NT 1 22/12/2011 Australia Pacific Airports (Melbourne) MELBOURNE VIC 1 22/12/2011 Pty. Limited PERTH Perth Airport Pty Ltd WA 1 22/12/2011 SYDNEY Sydney Airport Corporation Limited NSW 1 22/12/2011 CATEGORY 2 BROOME Broome International Airport Pty Ltd WA 2 22/12/2011 CHRISTMAS ISLAND Toll Remote Logistics Pty Ltd WA 2 22/12/2011 HOBART Hobart International Airport Pty Limited TAS 2 29/02/2012 NORFOLK ISLAND Norfolk Island Regional Council NSW 2 22/12/2011 September 2018 UNCLASSIFIED UNCLASSIFIED PORT HEDLAND PHIA Operating Company Pty Ltd WA 2 22/12/2011 SUNSHINE COAST Sunshine Coast Airport Pty Ltd QLD 2 29/06/2012 TOWNSVILLE AIRPORT Townsville Airport Pty Ltd QLD 2 19/12/2014 CATEGORY 3 ALBURY Albury City Council NSW 3 22/12/2011 ALICE SPRINGS Alice Springs Airport Pty Limited NT 3 11/01/2012 AVALON Avalon Airport Australia Pty Ltd VIC 3 22/12/2011 Voyages Indigenous Tourism Australia NT 3 22/12/2011 AYERS ROCK Pty Ltd BALLINA Ballina Shire Council NSW 3 22/12/2011 BRISBANE WEST Brisbane West Wellcamp Airport Pty QLD 3 17/11/2014 WELLCAMP Ltd BUNDABERG Bundaberg Regional Council QLD 3 18/01/2012 CLONCURRY Cloncurry Shire Council QLD 3 29/02/2012 COCOS ISLAND Toll Remote Logistics Pty Ltd WA 3 22/12/2011 COFFS HARBOUR Coffs Harbour City Council NSW 3 22/12/2011 DEVONPORT Tasmanian Ports Corporation Pty. -

East Pilbara Shire Council Minutes Ordinary
Unconfirmed copy of Minutes of Meeting held on 25 August 2017 subject to confirmation at meeting to be held on 22 September 2017 EAST PILBARA SHIRE COUNCIL MINUTES ORDINARY COUNCIL MEETING NOTICE IS HEREBY GIVEN that an ORDINARY Meeting of the Council was held, in Council Chambers, Newman, 10.00 AM, FRIDAY, 25 AUGUST, 2017. Allen Cooper CHIEF EXECUTIVE OFFICER DISCLAIMER No responsibility whatsoever is implied or accepted by the Shire of East Pilbara for any act, omission or statement or intimation occurring during Council or Committee Meetings. The Shire of East Pilbara disclaims any liability for any loss whatsoever and howsoever caused arising out of reliance by any person or legal entity on any such act, omission or statement or intimation occurring during Council or Committee Meetings. Any person or legal entity who acts or fails to act in reliance upon any statement, act or omission made in a Council or Committee Meeting does so at that person’s or legal entity’s own risk. In particular and without derogating any planning application or application of a licence, any statement or intimation of approval made by any member or Officer of the Shire of East Pilbara during the course of any meeting is not intended to be and is not taken as notice of approval from the Shire of East Pilbara. The Shire of East Pilbara warns that anyone who has any application lodged with the Shire of East Pilbara must obtain and should only rely on WRITTEN CONFIRMATION of the outcome of the application and any conditions attaching to the decision made by the Shire of East Pilbara in respect of the application. -
Kangaroo Management in Wa
WESTERN AUSTRALIA tate ildlife Vol. 4 No. 2 Autumn, 1973 Some-C:hins S~.GA~.S to think abou-C: •••• Vol. 4 No. 2 AUTUMN, 1973 Most persons think that a state in order to be happy Issued by direction of the Hon. A. W. Bicker ought to be large; but even if they are right, they have no ton, M.L.A., Minister for Fisheries and Fauna. idea of what is a large and what a small state ... To the Director of Fisheries and Fauna: B.K. Bowen, size of states there is a limit, as there is to other things, B.Sc. plants, animals, implements; for none of these retain their Chief Warden of Fauna: H.B. Shugg, A.A.P.A., A.F.A.I.M. natural power when they are too large or too small, but they either wholly lose their nature, or are spoiled. The support of the public is an essential component in any conservation or reserve management programme-but an informed, ARISTOTLE, 322 B.C. educated public is needed to ensure its con- tinuing success. This publication is designed as a medium by which the various organisations, indivi duals, and wildlife management personnel may be kept informed of the work being carried out by this department; of depart mental policies and directions; and for pro moting a better understanding and apprecia tion of Western Australian wildlife and the role it plays in maintaining a suitable environment in which man can live. S.W.A.N.S. is published quarterly at the conclusion of each season by: Extension and Publicity Service, Department of Fisheries and Fauna, 108 Adelaide Terrace, IN THIS ISSUE ... -

ZK Aug 06.Pdf
New Zealand Aircraft Register Amendments Aug 2006 Reg Prev. Action Man. Model Serial No Name and Address Action Date Effect Date DeReg. Reason Mark Mark ZK-CAE Initial registration Vans RV 7A 70213 Mr A C Tompkins 56C Kerry Drive QUEENSTOWN 9197 03/08/2006 03/08/2006 ZK-FLD Initial registration Zenith Zenith CH 601- XL 6-5079 Mr S van Rooij 3 Dawn Rise HAMILTON 2001 21/08/2006 21/08/2006 ZK-GHW Initial registration Schempp-Hirth Discus-2T 11 M W & J C Walker Ladies Mile, R D 1 QUEENSTOWN 9197 29/08/2006 29/08/2006 VH-ZHW ZK-HIQ Initial registration Bell 206B 3534 Whirlwind Charters Limited PO Box 33070 AUCKLAND 1332 29/08/2006 29/08/2006 N246M ZK-IAY Initial registration Robinson R44 1318 Q E & P M Whiting-Okeefe Port Charles COROMANDEL 2851 18/08/2006 18/08/2006 C-FHSN ZK-IBC Initial registration Aerospatiale AS 350B2 4098 Oceania Aviation Limited P O Box 72 053 AUCKLAND 1730 24/08/2006 24/08/2006 ZK-IDF Initial registration Eurocopter AS 350 B3 4063 Heli-Works Queenstown Helicopters Limited PO Box 2211 QUEENSTOWN 9197 08/08/2006 08/08/2006 ZK-JOP Initial registration Pro Sport Aviation Sportlite 103 1 H Aarts 236 Kaharoa Road ROTORUA 09/08/2006 09/08/2006 ZK-JQC Initial registration Delore Skytrike/Mega DRA001 D C Anderson 133 Clifton Terrace CHRISTCHURCH 8008 21/08/2006 21/08/2006 ZK-KPA Initial registration Micro Aviation B22J Bantam 06-0304 Mr K N G Potter 15 Domain Road AUCKLAND 29/08/2006 29/08/2006 ZK-MFE Initial registration Bushby Midget Mustang M-1-2036 Mr M F S Elworthy 333 Gleniti Road TIMARU 8621 16/08/2006 16/08/2006 ZK-NEJ -
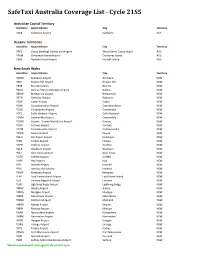
Safetaxi Australia Coverage List - Cycle 21S5
SafeTaxi Australia Coverage List - Cycle 21S5 Australian Capital Territory Identifier Airport Name City Territory YSCB Canberra Airport Canberra ACT Oceanic Territories Identifier Airport Name City Territory YPCC Cocos (Keeling) Islands Intl Airport West Island, Cocos Island AUS YPXM Christmas Island Airport Christmas Island AUS YSNF Norfolk Island Airport Norfolk Island AUS New South Wales Identifier Airport Name City Territory YARM Armidale Airport Armidale NSW YBHI Broken Hill Airport Broken Hill NSW YBKE Bourke Airport Bourke NSW YBNA Ballina / Byron Gateway Airport Ballina NSW YBRW Brewarrina Airport Brewarrina NSW YBTH Bathurst Airport Bathurst NSW YCBA Cobar Airport Cobar NSW YCBB Coonabarabran Airport Coonabarabran NSW YCDO Condobolin Airport Condobolin NSW YCFS Coffs Harbour Airport Coffs Harbour NSW YCNM Coonamble Airport Coonamble NSW YCOM Cooma - Snowy Mountains Airport Cooma NSW YCOR Corowa Airport Corowa NSW YCTM Cootamundra Airport Cootamundra NSW YCWR Cowra Airport Cowra NSW YDLQ Deniliquin Airport Deniliquin NSW YFBS Forbes Airport Forbes NSW YGFN Grafton Airport Grafton NSW YGLB Goulburn Airport Goulburn NSW YGLI Glen Innes Airport Glen Innes NSW YGTH Griffith Airport Griffith NSW YHAY Hay Airport Hay NSW YIVL Inverell Airport Inverell NSW YIVO Ivanhoe Aerodrome Ivanhoe NSW YKMP Kempsey Airport Kempsey NSW YLHI Lord Howe Island Airport Lord Howe Island NSW YLIS Lismore Regional Airport Lismore NSW YLRD Lightning Ridge Airport Lightning Ridge NSW YMAY Albury Airport Albury NSW YMDG Mudgee Airport Mudgee NSW YMER Merimbula -

2035 Master Plan August 2016
2035 Master Plan June 2016 2035 MASTER PLAN AUGUST 2016 CONTENTS 1.0 INTRODUCING OUR PLAN 3 5.7.2 Fire Rescue Building Location 18 5.8 Major Aircraft Maintenance 20 Our Vision, Our Mission 4 5.9 Engine Testing Bay 21 5.10 General Aviation 22 2.0 THE KEY ELEMENTS OF THE MASTER PLAN 5 5.11 Navigation Aids 23 5.12 Apron Demand Scenarios 24 3.0 PROTECTING OUR ENVIRONMENT 6 5.13 Apron Layouts 25 5.14 Planning 26 4.0 AERONAUTICAL FORECASTS 7 5.15 Helicopters 27 4.1 Passenger Projections 7 4.1.1 Estimated Passenger & Movements Forecast 7 THE TERMINAL 28 4.1.2 Capacity Projections 8 6.1 Current Terminal 28 4.1.3 Movement Projections 8 6.2 The New Terminal 29 6.3 Growth Beyond the New Terminal 31 5.0 AIRSIDE 9 5.1 Design Aircraft 9 LANDSIDE TRANSPORT 32 5.2 Constraints 10 7.1 External Access 33 5.3 Runway Strip Width and Taxiway Separation 11 7.2 Vehicle Volumes and Forecast 34 5.3.1 Runway Strip Width 11 7.3 Parking Volumes and Forecast 35 5.3.2 Taxiway Separation 11 5.4 Parallel Taxiway 12 LANDSIDE DEVELOPMENTF 36 5.5 Fuel Storage 13 8.1 Non-Aeronautical Commercial Development 36 5.5.1 Location Rationale 13 5.5.2 Dependency 13 Appendix One: Existing Airport Plan 37 5.6 Control Tower 15 5.6.1 Location of New Control Tower 17 Appendix Two: 2035 Master Plan 39 5.7 Rescue Fire 18 5.7.1 Part 139 Categorisation 18 nelson airport master plan page 2 We are pleased to be able to present our vision for the next 20 years at Nelson Airport. -

IFFR Book =7=Sect 2B
ROTARY IN ACTION 213 OPERATION INSPIRATION Rotary Club of Moorabbin The Rotary Club of Moorabbin Central in Victoria, runs a program over one day for relatively underprivileged secondary school students, called “Operation Inspiration”, where groups of around 30 students are given the opportunity to learn more about aviation and navigation, in an endeavour to improve their self esteem and motivation. The day includes a class briefing session, transport by Rotarians to Moorabbin airport, flights for all children, prizes and certificates, and a follow up on school projects. This program can be organised on a local community level, in conjunction with other Rotarians, the local Aero club, a police Air Wing, Air Training Corps, or a nearby Airforce base. FLYING SCHOLARSHIPS – New Zealand Fourteen high school received scholarships from the Rotary Club of Howick Somerville, N.Z. to attend the 38th annual Walsh Memorial Scout Flying School at Matamata for 14 days in January. The course covers all aspects of aviation from time flying, to theory lectures, and hands-on engineering and meteorology. Chair of the Scholarship Organising Committee, Past President John Simpson, said: “These scholarships give high school students the opportunity to achieve something special, as well as a head start towards possible vocation.” PP John, an air traffic controller with Airways Corporation of N.Z., is one of many people in the aviation industry volunteering time to assist the flying school. The Rotary Club of Howick Somerville is supported by a number of trusts including the June Gray and Chenery Memorial Trusts, along with several other Rotary clubs in New Zealand.