India Fact Sheet
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Disastrous Impact of Coronavirus (COVID 19) on Tourism and Hospitality Industry in India
Journal of Xi'an University of Architecture & Technology ISSN No : 1006-7930 Disastrous impact of Coronavirus (COVID 19) on Tourism and Hospitality Industry in India Dr. Amit Kumar (UGC NET, PhD, M.Phil, M.Com) University Department of Commerce and Business Management, Ranchi University, Ranchi Abstract The purpose of the current paper is to review the tourism industry has been badly affected by the Corona virus epidemic. The lockdown has broken the back of the tourism industry across the country. This has created employment crisis in front of 38 million people associated with the industry. Crores of people in India are directly or indirectly connected to the tourism industry. Even before the lockdown, many airlines and travel companies had sent more than 35 percent of their employees on leave without salary. The Travel and Tourism sector accounted for 9.2 percent of India's GDP in 2018 and provided 2.67 crore jobs. ICC Director General Rajiv Singh said, "Due to the Corona Virus epidemic, bookings for the entire year have decreased by 18-20 per cent in 2020, while the average daily fare has come down by 12-14 per cent." The industry association has sought a series of reliefs from the central government, including extending the loan repayment proposal by the RBI by three months to six months and complete exemption in GST for one year for the tourism, travel and hospitality sectors. "The ICC has suggested creating a travel and tourism sustainability fund, which transfers direct benefits to prevent financial loss and employment cuts," the ICC said in a statement. -

Correlates of Gender Bias and Formal Employment in India: Insights for Quick Revival After Covid-19 Pandemic
CORRELATES OF GENDER BIAS AND FORMAL EMPLOYMENT IN INDIA: INSIGHTS FOR QUICK REVIVAL AFTER COVID-19 PANDEMIC Sonam Arora* ABSTRACT The COVID-19 pandemic has led to global despair, risking the well-being of individuals and progress of societies. Prior to the pandemic, the Indian economy was grappling with the triple burden of rising unemployment among the educated youth, declining female labour force participation, and slowing growth momentum beginning 2017–18.With negative growth projections and pervasive gender gaps in formal employment, Indian educated women will be adversely affected as they are highly participative in the unpaid and informal work. The Indian development scenario looks bleak as the pandemic is likely to accentuate the existing tribulations in the post- pandemic period. Attempting to identify vulnerable states and provide a forward-looking approach, this paper explores the inter-play of growth, higher education, and employment from a gender perspective. The findings also highlight that neither growth nor the ballooning educated labour force resulted in the disposal of gender bias in India’s labour market. Keywords: gender gaps, formal employment, higher education, COVID-19, India 1. INTRODUCTION India has one of the lowest female labour force participation rates (FLFPRs) in the world, with less than a third of women (15 years and above) working or actively looking for a job (World Bank, 2019). While India’s gross domestic * Ph. D. Scholar, National Institute of Educational Planning and Administration, India -16, E-mail: [email protected], [email protected] Manpower Journal, Vol. LIV, No. 1 & 2, January – June, 2020 62 Manpower Journal, Vol. -

The Star of Yoga Guidance from the Light
The Star of Yoga Guidance from the Light (From an upcoming book “Meditation For the Monkey Mind”) By Mas Vidal As we look up to the night sky we get a spectacular glimpse of the vast galaxy we see from earth. Stars abound through out the sky like mini suns each creating their own distinct light, some forming clusters and interesting configurations. There is an inherent quality in humanity to feel an attraction to light, be it sunlight or open spaces. It makes sense as we have come to understand the science behind energy we know that like attracts like. We realize there is great value that comes from being in the light, which breeds an optimism and greater awareness. In general people feel a kinship towards one another when they share something in common. A star’s light is symbolic of the highest ideal of every human being to live in love, light and harmony (sat, chit andanda) with nature and all aspects of life. The ancients have always looked to the stars for guidance, healing and understanding the cycles of nature. A star’s five points symbolize a connection to the five great elements (pancha maha bhutas) and reflects the gradation of energy from gross (earth) to subtle (sky). The mystical star of yoga provides guidance on the journey towards enlightenment as various pathways, with each empowering us to reach the culmination or purna as the true yogic ideal of living a fully integrated lifestyle. Such integration is based on a balance between spirit and ecology thus reminding us of the importance of responsibility in our thoughts, words and actions that can either connect us or create greater divide from the Divine. -

Odisha Pradesh Congress Seva Dal Office Bearers
Odisha Pradesh Congress Seva Dal Office Bearers Chief Organiser 1 Shri Biren Mohan Patnaik Shri Biren Mohan Patnaik Chief Organiser Chief Organiser Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal Congress Bhawan, Unit-2 A-91/1, Sahid Nagar Bhubaneshwar Opp.Aaykar Bhawan Odisha Bhubaneswar Tel: 09937010325, 09437010325 Odisha Mahila Organiser State Chief Instructor 1 Miss. Usha Rani Behera 1 Shri Ram Prasad Jaiswal Mahila Organiser Chief Instructor Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal At-Jobra Road At/PO-Panposh Basti Cuttack Rourela-4 Odisha Distt-Sundergarh Tel-07978216221 Odisha Tel-09437117047 State Treasuer State Office Incharge 1 Shri Ratnakar Behera 1 Shri Jyotish Kumar Sahoo Treasurer Office Incharge Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal Plot No.500/502 Plot No.743-P/12-A Near Krishna Tower Jameswar Bhawan Nayapalli,Bhubaneswar At/PO-Baramunda Odisha Bhubaneshwar Odisha Tel-9437307634 State Organisers 1 Shri Ashok Kumar Singh 2 Shri Rabindranath Behera Organiser Organiser Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal At//PO-Anakhia At/PO-Telengapentha Distt-Jagatsinghpur Distt-Cuttack Odisha Odisha Tel-09439956517 Tel-09438126788 3 Smt. Trupti Das 4 Shri Benudhar Nayak Organiser Organiser Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal At/PO-Tulsipur, Matha Sahi, At/PO-Daspalla Distt-Cuttack Distt-Nayagarh Odisha Odisha Tel-08895741510 Tel-08895412949 5 Smt. Bjaylaxmi Mahapatra 6 Ms. Nalini Behera Organiser Organiser Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal At/PO-Bentapada At-Khairpur Via-Athagarh PO-Banamallpur Distt-Cuttack Via-Balipatna Odisha Distt-Khurda Tel-09437276083 Odisha Tel-09438300987 7 Shri Madhab Biswal 8 Shri Munu Saraf Organiser Organiser Odisha Pradesh Congress Seva Dal Odisha Pradesh Congress Seva Dal Vill-Bankoi At/PO-Sunaripada Distt-Khurda Distt-Sundergarh Odisha Odisha Tel-09556102676 Tel-09937235678 9 Shri Rajendra Prasad 10 Md. -

Forecasting Transmission Dynamics of COVID-19 Epidemic in India Under Various Containment Measures
medRxiv preprint doi: https://doi.org/10.1101/2020.05.08.20095877; this version posted May 14, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Forecasting Transmission Dynamics of COVID-19 Epidemic in India Under Various Containment Measures- A Time-Dependent State-Space SIR Approach Vishal Deoa, b, Anuradha R. Chetiyab, Barnali Dekab and Gurprit Grovera aDepartment of Statistics, Faculty of Mathematical Sciences, University of Delhi, Delhi, India bDepartment of Statistics, Ramjas College, University of Delhi, Delhi, India Abstract Objectives Our primary objective is to predict the dynamics of COVID-19 epidemic in India while adjusting for the effects of various progressively implemented containment measures. Apart from forecasting the major turning points and parameters associated with the epidemic, we intend to provide an epidemiological assessment of the impact of these containment measures in India. Methods We propose a method based on time-series SIR model to estimate time-dependent modifiers for transmission rate of the infection. These modifiers are used in state-space SIR model to estimate reproduction number R0, expected total incidence, and to forecast the daily prevalence till the end of the epidemic. We consider four different scenarios, two based on current developments and two based on hypothetical situations for the purpose of comparison. Results Assuming gradual relaxation in lockdown post 17 May 2020, we expect the prevalence of infecteds to cross 9 million, with at least 1 million severe cases, around the end of October 2020. -
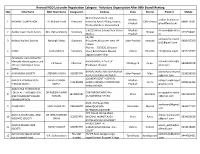
Revised NGO List Under Registration Category
Revised NGO List under Registration Category - Voluntary Organization After 80th Board Meeting SNo NGO Name NGO Head Name Designation Address State District Email id Mobile 48 Panchwati Ward, Opp. Madhya aadhar.foundation 1 AADHAR FOUNDATION ER. Mahesh Kinth President Narendra Ayush Dhaba, Poama, Chhindwara 8989173581 Pradesh @rediffmail.com P/o Kundali Kala, Parasia Road E-4/223,Arera Colony,Near 10 no. Madhya [email protected] 2 Aadhar Gyan Dhatri Samiti Mrs. Ratna Mukerji Secretary Bhopal 9755554401 Market Pradesh m S2/258 adityawelfaresocie 3 Aaditya Welfare Society Narsingh Yadav Secretary Bhojubeer,Bhojubeer,Near UP Uttar Pradesh Varanasi 9936437260 [email protected] College Plot No. - 70/3530, (Ground 4 AAINA Sneha Mishra Secretary Floor),Behind Hotel Mayfair Odisha Khordha [email protected] 9437017967 Lagoon,Jaydev Vihar Aakanksha Lions School for Mentally Handicapped a unit Awanti Vihar,,In front of aakankshalsmh@y 5 K K Nayak Chairman Chattisgarh Raipur 9826845678 of Lions Club Raipur Sewa Bhaktawar Bhawan ahoo.com Samiti KHARAGIPUR,GANGAUPUR,RAM akankshasocietyma 6 AAKANKSHA SOCIETY JITENDRA YADAV SECRETARY Uttar Pradesh Mau 9258038100 AUPUR SUWAH LINK MARG [email protected] 120 NEAR GOVT HOSPITAL AARIOLA PRAKASH PUNJ BALVEER SINGH Madhya balveer.singhrajput 7 CHAIRMAN HARDA,AWASTHI COMPOUND Harda 9009616393 SHIKSHA SAMITI RAJPUT Pradesh @yahoo.com HARDA,HARDA AAROGYAA FOUNDATION FOR HEALTH PROMOTION DR RAJESH KUMAR COAT BAZAR,WARD No aarogyaafoundatio 8 SECERETARY Bihar Sitamarhi 9934691872 AND COMMUNITY BASED SUMAN 13,MAHARANI STHAN -

India-U.S. Relations
India-U.S. Relations July 19, 2021 Congressional Research Service https://crsreports.congress.gov R46845 SUMMARY R46845 India-U.S. Relations July 19, 2021 India is expected to become the world’s most populous country, home to about one of every six people. Many factors combine to infuse India’s government and people with “great power” K. Alan Kronstadt, aspirations: its rich civilization and history; expanding strategic horizons; energetic global and Coordinator international engagement; critical geography (with more than 9,000 miles of land borders, many Specialist in South Asian of them disputed) astride vital sea and energy lanes; major economy (at times the world’s fastest Affairs growing) with a rising middle class and an attendant boost in defense and power projection capabilities (replete with a nuclear weapons arsenal and triad of delivery systems); and vigorous Shayerah I. Akhtar science and technology sectors, among others. Specialist in International Trade and Finance In recognition of India’s increasingly central role and ability to influence world affairs—and with a widely held assumption that a stronger and more prosperous democratic India is good for the United States—the U.S. Congress and three successive U.S. Administrations have acted both to William A. Kandel broaden and deepen America’s engagement with New Delhi. Such engagement follows decades Analyst in Immigration of Cold War-era estrangement. Washington and New Delhi launched a “strategic partnership” in Policy 2005, along with a framework for long-term defense cooperation that now includes large-scale joint military exercises and significant defense trade. In concert with Japan and Australia, the Liana W. -

Sources for the Study of Gurū Gobind Singh's Life and Times
G.S. Mann: Sources for Study 229 Sources for the Study of Guru Gobind Singh's Life and Times Gurinder Singh Mann University of California, Santa Barbara ___________________________________________________________ This essay surveys the sites, artifacts, and literary texts associated with Guru Gobind Singh's period (1675-1708). In the process, it introduces a set of sources of information as well as attempts at reorientation of the context that produced them. In a brief conclusion, the essay highlights the need for expanding and revising the current understanding of the Guru's life. ___________________________________________________________ The present day understanding of Guru Gobind Singh's life is constructed around three landmarks: his birth in Patna in eastern India, in 1666; his creation of the Khalsa ("Community of the Pure") at Anandpur, in the Punjab hills, in 1699; and his replacement of the office of the personal Guru with the Granth, the Sikh scripture, thereby elevating it to the position of the Guru Granth ("Book manifested as the Guru") at the time of his death, in Nanderh in south India, in 1708.1 The details that fill in the forty-two years of the Guru's life are culled from a variety of texts, which begin with the Dasam Granth ("the tenth book" or "book of the tenth [Guru]"), an anthology of poetry created largely between 1685 to 1698, and Sri Gur Sobha ("Praise of the Guru"), a poetic history of the period presently dated in 1711, and include eighteenth and nineteenth century writings culminating in Giani Gian Singh's synthetic narrative, Tvarikh Guru Khalsa ("History of the Guru Community"), completed in 1891.2 (For a brief review of this chronology of events see Appendix). -

Vaisnava Goddess As Plant: Tulasi in Text and Context John Carbone
Florida State University Libraries Electronic Theses, Treatises and Dissertations The Graduate School 2008 Vaisnava Goddess as Plant: Tulasi in Text and Context John Carbone Follow this and additional works at the FSU Digital Library. For more information, please contact [email protected] FLORIDA STATE UNIVERSITY COLLEGE OF ARTS AND SCIENCES VAISNAVA GODDESS AS PLANT: TULASI IN TEXT AND CONTEXT By JOHN CARBONE A Thesis submitted to the Department of Religion in partial fulfillment of the requirements for the degree of Master of Arts Degree Awarded: Spring Semester, 2008 The members of the Committee approve the Thesis of John Carbone defended on April 7, 2008. Kathleen M. Erndl Professor Directing Thesis Bryan Cuevas Committee Member Adam Gaiser Committee Member The Office of Graduate Studies has verified and approved the above named committee members. ii For Irina and Joseph iii ACKNOWLEDGEMENTS I wish to thank Kathy Neall for her help in editing this manuscript. iv TABLE OF CONTENTS List of Figures .................................................................................... vi Abstract .......................................................................................... vii Introduction……………………………………………………………………. 1 1. Tulasī as the Plant Form of Lakṣmī................................................... 9 Śrī and Lakṣmī in the Vedas .......................................................... 9 Purāṇic Śrī and Lakṣmī.................................................................. Yakṣa, Yakṣī, and Śrī’s Iconography ............................................ -

COVID-19 Pandemic Dynamics in India and Impact of the SARS-Cov-2 Delta
medRxiv preprint doi: https://doi.org/10.1101/2021.06.21.21259268; this version posted June 25, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. 1 COVID-19 pandemic dynamics in India and impact of the SARS-CoV-2 2 Delta (B.1.617.2) variant 3 Wan Yang1* and Jeffrey Shaman2 4 1Department of Epidemiology, 2Department of Environmental Health Sciences, Mailman School 5 of Public Health, Columbia University, New York, NY, USA 6 *Correspondence to: [email protected] 7 8 Abstract 9 The Delta SARS-CoV-2 variant has spread quickly since first being identified. To better 10 understand its epidemiological characteristics and impact, we utilize multiple datasets and 11 comprehensive model-inference methods to reconstruct COVID-19 pandemic dynamics in India, 12 where Delta first emerged. Using model-inference estimates from March 2020 to May 2021, we 13 estimate the Delta variant can escape adaptive immunity induced by prior wildtype infection 14 roughly half of the time and is around 60% more infectious than wildtype SARS-CoV-2. In 15 addition, our analysis suggests that the recent case decline in India was likely due to 16 implemented non-pharmaceutical interventions and weather conditions less conducive for 17 SARS-CoV-2 transmission during March – May, rather than high population immunity. Model 18 projections show infections could resurge as India enters its monsoon season, beginning June, if 19 intervention measures are lifted prematurely. -

Kirtan / Katha & Langar Seva Time Saturday 2Nd October Rehraas
Waheguru Ji Ka Khalsa Waheguru Ji Ki Fateh Programme for the month of October 2021 Date Programme - Kirtan / Katha & Langar Seva Time Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 6:30pm Saturday Kirtan - Hazoori Jatha 6:30pm - 7:30pm 2nd October Langar Seva - Mrs Jaswant Kaur Matharu & Family Sunday Asa ki Vaar - Hazoori Jatha 7:00am - 8:30am 3rd October Chah Seva - Guru Ka Khajana Wednesday Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 7:30pm 6th October Langar Seva - Guru Ka Khajana Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 6:30pm Saturday Kirtan - Hazoori Jatha 6:30pm - 7:30pm 9th October Langar Seva - Mr Inderjit Singh & Mrs Mandeep Kaur Dhamrait & Family Sunday Asa ki Vaar - Hazoori Jatha 7:00am - 8:30am 10th October Chah Seva - Guru Ka Khajana Wednesday Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 7:30pm 13th October Langar Seva - Guru Ka Khajana Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 6:30pm Saturday Kirtan - Hazoori Jatha 6:30pm - 7:30pm 16th October Langar Seva - Mr Karamjit Singh & Mr Balkar Singh & Mr Harwinder Singh & Santokh Singh Sangrand - Kattak Sunday Asa ki Vaar - Hazoori Jatha 7:00am - 8:30am 17th October Chah Seva - Guru Ka Khajana Puranmashi Wednesday Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 7:30pm 20th October Langar Seva - Guru Ka Khajana Rehraas Sahib & Kirtan - Hazoori Jatha 6:00pm - 6:30pm Kirtan - Hazoori Jatha 6:30pm - 7:30pm Saturday Langar Seva - Nirmal Singh, Sukhwinder Singh, Surinderpal Singh, 23rd October Raji Shah, Naninder Singh, Bahadur Singh, Varinder Singh, Sodhi Singh -

Strategies of the New Hindu Religious Movements
Sustainability 2010, 2, 3500-3519; doi:10.3390/su2113500 OPEN ACCESS sustainability ISSN 2071-1050 www.mdpi.com/journal/sustainability Article Education for a Sustainable Future: Strategies of the New Hindu Religious Movements Martin Haigh Department of Anthropology and Geography, Oxford Brookes University, Gipsy Lane Campus, Headington, Oxford, OX3 0BP, UK; E-Mail: [email protected]; Tel.: +44-1865-483785; Fax: +44-1865-483937 Received: 10 October 2010; in revised form: 8 November 2010 / Accepted: 10 November 2010 / Published: 17 November 2010 Abstract: Increasingly, sustainability is conceived as a crisis of the human mind and the key challenge for pro-sustainability education is developing sufficient motivation in learners. The spiritual aspirations of religious communities contain sufficient motivational force, which may be deployed for effective sustainability education. This paper explores the approaches to sustainability and sustainability education of some internationally-oriented Hindu religious movements. These include the rural education initiatives of Gandhian Sarvodaya, which emphasizes non-harming, self-reliance and personal ethics, ISKCON, which emphasizes devotional service, P.R. Sarkar‘s Ananda Marg, which emphasizes cooperative enterprise, the Tantric body re-imagined at the social scale, and Swami Vivekananda‘s Sri Ramakrishna Order, which emphasizes karma yoga, spiritual development through service to the God in each human. It also describes the British Hindu contribution to the UNDP/ARC‘s multi-faith sustainability initiative ―Many Heavens, One Earth‖; which is the ―Bhumi Project‖ and its two main campaigns, Green Temples and Compassionate Living. Keywords: community education; NGO; Hinduism; faith-based environmentalism; Sarvodaya; Gandhi; Vivekananda; PROUT; ISKCON; Ananda Marg; Karma Yoga; Bhakti Yoga; Bhumi Project 1.