Effect of Cusp Inclination and Occlusal Dimension
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aging White-Tailed Deer by Tooth Wear and Replacement
Aging White-tailed deer by tooth wear and replacement Aging Characteristics • Physical Characteristics • Antler Size • Number of points not correlated with age • Body size and shape • Neck • Waist • Back • Behavior • Tooth wear and replacement- Harvested Deer Age Classes Born in May and June Fall harvest 6 months- fawn 1.5 yrs- yearling 2.5 yrs 3.5 yrs 4.5 yrs 5.5 yrs 6.5 yrs Tooth Wear The amount of visible dentine is an important factor in determining the age. The tooth wear and replacement method is not 100% accurate however, due to the differences in habitat. Tooth wear on a farmland deer may not be as fast as that of a deep woods buck. Severinghaus (1949) aging method Focus on lower jaw bone Adult deer 3 premolars and 3 molars 6 Months 4 teeth showing. 3rd premolar has three cusps 1.5 yrs •6 teeth •Third premolar •Third molar (last tooth) may still be erupting •Cusps of molars have sharp points. •Inset: Extremely worn third premolar may fool people into thinking deer is older. Actually, this tooth is lost after 1-1/2; years and replaced with a permanent two-cusped premolar. 2.5 yrs •Teeth are permanent •On the first molar (4th tooth) the cusps are sharp • Enamel > dentine • Third cusp (back cusp) of sixth tooth (third molar) is sharp. 3.5 yrs •Cusps show some wear •Dentine now thicker than enamel on cusp of fourth tooth (first molar). •Dentine of fifth tooth (second molar) usually not as wide as enamel. •Back cusp is flattened. 4.5 yrs •Cusp of fourth tooth (first molar) is gone. -

Frequency of Cusp of Carabelli in Orthodontic Patients Reporting to Islamabad Dental Hospital
ORIGINAL ARTICLE POJ 2016:8(2) 85-88 Frequency of cusp of carabelli in orthodontic patients reporting to Islamabad Dental Hospital Maham Niazia, Yasna Najmib, Muhammad Mansoor Qadric Abstract Introduction: Anatomic variation in the anatomy of maxillary molars can have clinical implications in dentistry ranging from predisposition to dental caries or loosely fitting orthodontic bands. The aim of this study was to determine the frequency of cusp of carabelli in permanent first molars of patients reporting to the Orthodontic department. Material and Methods: A total of 698 patients reporting to the Orthodontic Department, Islamabad Dental Hospital, were evaluated from their orthodontic records. Upper occlusal photographs and dental casts of these patients comprised the data. Results: 245 (35.1%) patients showed the presence of the cusp while 453 (64.9%) had no accessory cusp present. Larger proportion of females had cusp of carabelli when compared with males. Bilateralism was found in 75.1% subjects while unilateralism existed in 24.9%, both being higher in females. Among the unilateral cases, higher trend was observed on the right side then the left. Conclusions: It was concluded that the frequency of cusp of carabelli was less in a population sample of Islamabad than other Asian samples, but an opposite trend was seen when compared to a population sample of Khyber Phukhtunkhwa showing different prevalence rates in different ethnicities. Keywords: Cusp of carabelli; maxillary first molars; caries; orthodontic patients Introduction unilaterally or bilaterally. However it he Cusp of Carabelli is a small additional generally appears bilaterally5 but Hirakawa T cusp which is situated on the mesio- and Dietz found ‘rare’ unilateral cases.6 Its palatal surface of first maxillary molars and size varies from being the largest cusp of the tooth to a rudimentary elevation. -

Molar-Incisor Hypomineralization and Delayed Tooth Eruption
Winter 2017, Volume 6, Number 4 Case Report: Mandibular Talon Cusp Associated With Molar-Incisor Hypomineralization and Delayed Tooth Eruption ٭Katayoun Salem1 , Fatemeh Moazami2, Seyede Niloofar Banijamali3 1. Assistant Professor, Department of Pediatric Dentistry, Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. 2. Pedodontist, Tehran, Iran. 3. Postgraduate Student, Department of Pediatric Dentistry, Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. Use your device to scan and read the article online Citation: Salem K, Moazami F, Banijamali SN. Mandibular Talon Cusp Associated With Molar-Incisor Hypomineralization and Delayed Tooth Eruption. Journal of Dentomaxillofacial Radiology, Pathology and Surgery. 2017; 6(4):141-145. : http://dx.doi.org/10.32598/3dj.6.4.141 Funding: See Page 144 Copyright: The Author(s) A B S T R A C T Talon cusp is an odontogenic anomaly in anterior teeth, caused by hyperactivity of enamel Article info: in morphodifferentiation stage. Talon cusp is an additional cusp with several types based on Received: 25 Aug 2017 its extension and shape. It has enamel, dentin, and sometimes pulp tissue. Moreover, it can Accepted: 20 Nov 2017 cause clinical problems such as poor aesthetic, dental caries, attrition, occlusal interferences, Available Online: 01 Dec 2017 and periodontal diseases. Therefore, early diagnosis and effective treatment of talon cusp are essential. Maxillary incisors are the most commonly affected teeth. However, occurrence of mandibular talon cusp is a rare entity. We report a talon cusp in the lingual surface of the permanent mandibular left central incisor, in a 7-year-old Iranian boy. To our knowledge it is Keywords: the third case reported in Iranian patients. -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth. -

Anterior and Posterior Tooth Arrangement Manual
Anterior & Posterior Tooth Arrangement Manual Suggested procedures for the arrangement and articulation of Dentsply Sirona Anterior and Posterior Teeth Contains guidelines for use, a glossary of key terms and suggested arrangement and articulation procedures Table of Contents Pages Anterior Teeth .........................................................................................................2-8 Lingualized Teeth ................................................................................................9-14 0° Posterior Teeth .............................................................................................15-17 10° Posterior Teeth ...........................................................................................18-20 20° Posterior Teeth ...........................................................................................21-22 22° Posterior Teeth ..........................................................................................23-24 30° Posterior Teeth .........................................................................................25-27 33° Posterior Teeth ..........................................................................................28-29 40° Posterior Teeth ..........................................................................................30-31 Appendix ..............................................................................................................32-38 1 Factors to consider in the Aesthetic Arrangement of Dentsply Sirona Anterior Teeth Natural antero-posterior -
CHAPTER 5Morphology of Permanent Molars
CHAPTER Morphology of Permanent Molars Topics5 covered within the four sections of this chapter B. Type traits of maxillary molars from the lingual include the following: view I. Overview of molars C. Type traits of maxillary molars from the A. General description of molars proximal views B. Functions of molars D. Type traits of maxillary molars from the C. Class traits for molars occlusal view D. Arch traits that differentiate maxillary from IV. Maxillary and mandibular third molar type traits mandibular molars A. Type traits of all third molars (different from II. Type traits that differentiate mandibular second first and second molars) molars from mandibular first molars B. Size and shape of third molars A. Type traits of mandibular molars from the buc- C. Similarities and differences of third molar cal view crowns compared with first and second molars B. Type traits of mandibular molars from the in the same arch lingual view D. Similarities and differences of third molar roots C. Type traits of mandibular molars from the compared with first and second molars in the proximal views same arch D. Type traits of mandibular molars from the V. Interesting variations and ethnic differences in occlusal view molars III. Type traits that differentiate maxillary second molars from maxillary first molars A. Type traits of the maxillary first and second molars from the buccal view hroughout this chapter, “Appendix” followed Also, remember that statistics obtained from by a number and letter (e.g., Appendix 7a) is Dr. Woelfel’s original research on teeth have been used used within the text to denote reference to to draw conclusions throughout this chapter and are the page (number 7) and item (letter a) being referenced with superscript letters like this (dataA) that Treferred to on that appendix page. -

Molar Cusps in Southern Chinese John Y.K
16 The Open Anthropology Journal, 2010, 3, 16-19 Open Access Molar Cusps in Southern Chinese John Y.K. Ling and Ricky W.K. Wong* Orthodontics, University of Hong Kong, Hong Kong Abstract: Aim: To investigate the number of molar cusps of the Southern Chinese and compare these with studies in dif- ferent populations. Materials and Methods: The number of molar cusps of study casts of an unselected sample from a 12 year old Hong Kong Oral Health Survey of 12 year old children (n=459; 295 boys and 164 girls) were studied. Results: For upper first molars, 5-cusp molars were the most prevalent in males (39%) while 4-cusp molars were the most prevalent in females (39%). For lower first molars, 5-cusp molars were the most prevalent in both sexes (63%-72%). For lower second molars, 5-cusp molars were the most prevalent in both sexes (43%-53%). Conclusion: Different from traditionally described, the Southern Chinese has more 5-cusp lower second molars than the 4- cusp ones. Keywords: Molar cusp, Southern Chinese. INTRODUCTION the Aleuts, the frequency of 4 cusps is 100 % for the first molars, 69 % for the 2nd molars and 31 % for the 3rd mo- It is generally believed that the numerous morphologic lars. characteristics of the teeth are genetically determined [1, 2]. Detailed description and study of these traits could provide There are normally five main cusps on a lower molar. valuable information regarding phylogeny of man and dis- The fifth or disto-buccal cusp is the most variable, which tinctions between races and subraces [1, 3-12]. -

Concommitant Occurance of Dens Invaginatus and Talon Cusp: a Case Report
Case Report Concommitant occurance of dens invaginatus and talon cusp: A case report Ocorrência simultânea de dens invaginatus e cúspide talon: relato de caso Abstract Monica Yadav a Meghana S.M b a Purpose: Morphological dental anomalies of the maxillary lateral incisors are relatively Sandip R. Kulkarni common. However, their simultaneous occurrence is a relatively rare event. We report a case of dens invaginatus and talon cusp concurrently affecting maxillary lateral incisors. The etiology, pathophysiology, association with other dental anomalies, as well as various treatment a Department of Oral Pathology and Microbiology, modalities of these anomalies are discussed. Terna Dental College and Hospital, Nerul, Navi Case description: An 18-year-old male patient reported with a complaint of crowding of Mumbai, India maxillary front teeth. On intraoral examination, permanent dentition with Class I malocclusion b Department of Oral Pathology, Terna Dental with anterior crowding was observed. Tooth 12 showed a radiopaque invagination from College and Hospital, Nerul, Navi Mumbai, a lingual pit but confined to the crown of the tooth. This invagination was approximately India circular with a central core of radiolucency, which was consistent with the diagnosis of a dens invaginatus type I. Tooth 22 showed the talon cusp as a typical inverted cone with enamel and dentine layers and a pulp horn extending only into the base of the cusp. Talon cusp was treated by prophylactic enameloplasty to avoid plaque accumulation, the deep lingual pit was sealed using composite resin and regular clinical and radiographic follow-up was advised. Patient was scheduled for orthodontic treatment to correct crowding of maxillary anterior teeth. -
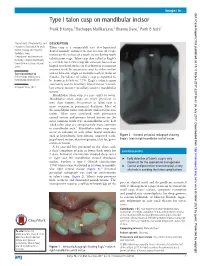
Type I Talon Cusp on Mandibular Incisor Pratik B Kariya,1 Rachappa Mallikarjuna,2 Bhavna Dave,1 Parth B Joshi1
Images in… BMJ Case Reports: first published as 10.1136/bcr-2017-220736 on 26 July 2017. Downloaded from Type I talon cusp on mandibular incisor Pratik B Kariya,1 Rachappa Mallikarjuna,2 Bhavna Dave,1 Parth B Joshi1 1Department of Pedodontics and DESCRIPTION Preventive Dentistry, K M Shah Talon cusp is a comparably rare developmental Dental College and Hospital, dental anomaly assumed to arise because of evagi- Vadodara, India nation on the surface of a tooth crown during tooth 2Pedodontics and Preventive calcification stage. Talon cusp also called as Eagle’s Dentistry, Child Dental Health, Oman Dental College, Muscat, is a well-defined extra cusp like structure located on Oman lingual or palatal surface of deciduous or permanent anterior teeth. Its occurrence may be either unilat- Correspondence to eral or bilateral, single or multiple teeth in males or Dr Rachappa Mallikarjuna, females. Prevalence of talon’s cusp is reported to mmrachappa@ gmail. com be between 0.06% to 7.7%. Eagle’s talon is most commonly seen in maxillary lateral incisor >maxil- Accepted 4 July 2017 lary central incisor> maxillary canine> mandibular incisor.1 Mandibular talon cusp is a rare entity to occur. Mandibular talon cusps are more prevalent in men than women. Occurrence in talon cusp is more common in permanent dentition. Most of the mandibular talon cusp shows unilateral presen- tation. Talon cusp associated with permanent central incisor and primary lateral incisor are the most common tooth type in mandibular arch. Left sided talon cusp are comparatively more common in mandibular arch.1 Mandibular talon cusp may occur in isolation or with other dental anomalies such as hypodontia, hyperdontia, impacted teeth, Figure 2 Intraoral periapical radiograph showing peg-shaped incisor, dens invaginatus, cleft lip, gemi- Eagle’s talon in right mandibular central incisor. -

Glossary of Commonly Used Dental Terms
Glossary of Commonly Used Dental Terms A • Abutment: A tooth or implant used to support a prosthesis. A crown unit used as part of a fixed bridge. • Abscess: A localized inflammation due to a collection of pus in the bone or soft tissue, usually caused by an infection. • Amalgam: A dental filling material, composed of mercury and other minerals, used to fill decayed teeth. • Alveoloplasty: A surgical procedure used to recontour the supporting bone struc tures in preparation of a complete or partial denture. • Anesthetic: A class of drugs that eliminated of reduces pain. See local anesthetic. • Anterior: Refers to the teeth and tissues located towards the front of the mouth (upper or lower incisors and canines). • Apex: The tip end of a root. • Apexification: A method of inducing apical closure, or the continual apical develop ment of the root of an incompletely formed tooth, in which the pulp is no longer vital. B • Bicuspid: A two-cuspid tooth found between the molar and the cuspid also known as an eye tooth or canine tooth. • Biopsy: A process of removing tissue to determine the existence of pathology. • Bitewing x-ray: X-rays taken of the crowns of teeth to check for decay. • Bleaching: The technique of applying a chemical agent, usually hydrogen peroxide, to the teeth to whiten them. • Bondin: A process to chemically etch the tooth's enamel to better attach ( bond ) composite filling material, veneers, or plastic/acrylic. • Bone loss: The breakdown and loss of the bone that supports the teeth, usually caused by infection or long-term occlusal ( chewing areas of the teeth ) stress. -

Research Article PREVALENCE of CUSP of CARABELLI IN
Available Online at http://www.recentscientific.com International Journal of CODEN: IJRSFP (USA) Recent Scientific International Journal of Recent Scientific Research Research Vol. 11, Issue, 06(A), pp. 38805-38807, June, 2020 ISSN: 0976-3031 DOI: 10.24327/IJRSR Research Article PREVALENCE OF CUSP OF CARABELLI IN MADURAI POPULATION Dr R.Saravanan Professor and HOD Department of Pedodontic CSI College of Dental Sciences and Research DOI: http://dx.doi.org/10.24327/ijrsr.2020.1106.5381 ARTICLE INFO ABSTRACT Article History: Aim: The aim of the study was to determine the prevalence of cusp of carabelli in permanent tooth among children at Madurai population. Received 4th Mrach, 2020 Materials And Methods: Total number 800 patients from three different ethnic groups – Hindu, Received in revised form 25th Islam, Christian were examined clinically and study casts were made. Permanent maxillary first April, 2020 molars were examined for the expression of Carabelli's trait. The occurrence of cusp of carabelli was Accepted 18th May, 2020 assessed by Dahlberg classification system. The data’s were collected and analyzed using SPSS Published online 28th June, 2020 software. Results: Cusp of Carabelli was present in 72% of the study population in maxillary first permanent Key Words: molar. Type 2 and Type 3 was the most frequently expressed and Type 6 was the least frequently Cusp of carabelli, permanent molar, expressed. The prevalence of cusp of carabelli among the ethnic groups was almost same. The Madurai population. expression of trait was bilateral in 60% of the study population. Conclusion: The prevalence of cusp of carabelli among the study population at Madurai was predominant. -

An Unusual Mandibular Second Molar Mimicking Maxillary First Molar – a Rare Occurrence Srinivasulu Sakamuri and Sreekanth Kumar Mallineni*
Case Report iMedPub Journals Periodontics and Prosthodontics 2018 www.imedpub.com Vol.4 No.1:01 ISSN 2471-3082 DOI: 10.21767/2471-3082.100037 An Unusual Mandibular Second Molar Mimicking Maxillary First Molar – A Rare Occurrence Srinivasulu Sakamuri and Sreekanth Kumar Mallineni* Narayana Dental College, Nellore, Andhra Pradesh, India *Corresponding author: Sreekanth Kumar Mallineni, Narayana Dental College, Nellore, Andhra Pradesh, India, Tel: +918985833533; E-mail: [email protected] Received date: December 02, 2017; Accepted date: December 20, 2017; Published date: January 03, 2018 Copyright: © 2018 Sakamuri S. This is an open-access article distributed under the terms of the creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited. Citation: Sakamuri S. An Unusual Mandibular Second Molar Mimicking Maxillary First Molar – A Rare occurrence. Periodon Prosthodon. 2018, Vol.4 No.1:01. molars. It has been reported that buccal accessory cusps are very rare in mandibular molars [2,9] and presence of an Abstract oblique ridge even rare in mandibular molars. As the variations in crown has not been reported in the literature, and the Dental anomalies are common in the permanent dentition purpose of the present case report was to describe an unusual when compared to the primary dentition, and more mandibular second molar with an oblique ridge and buccal common in the maxillary arch. These could be localized to cusp resembling the crown of the maxillary molar with cusp of one or two teeth and could be generalized, affected by all Caraballi. teeth most of the times, which might be apart from syndromic or systemic disorders.