Molar-Incisor Hypomineralization and Delayed Tooth Eruption
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
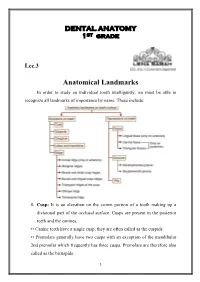
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Case Report Talon Cusp Type I: Restorative Management
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2015, Article ID 425979, 5 pages http://dx.doi.org/10.1155/2015/425979 Case Report Talon Cusp Type I: Restorative Management Rafael Alberto dos Santos Maia,1 Wanessa Christine de Souza-Zaroni,2 Raul Sampaio Mei,3 and Fernando Lamers2 1 Oral and Maxillofacial Surgery, HGU, University of Cuiaba,´ 78016-000 Cuiaba,´ MT, Brazil 2School of Dentistry, Cruzeiro do Sul University (UNICSUL), 08060-070 Sao˜ Paulo, SP, Brazil 3School of Dentistry, University Center of Grande Dourados (UNIGRAN), 79824-900 Dourados, MS, Brazil Correspondence should be addressed to Wanessa Christine de Souza-Zaroni; [email protected] Received 9 February 2015; Accepted 15 April 2015 Academic Editor: Carla Evans Copyright © 2015 Rafael Alberto dos Santos Maia et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The teeth are formed during intrauterine life (i.e., gestation) during the odontogenesis stage. During this period, the teeth move until they enter the oral cavity. This course covers various stages of dental development, namely, initiation, proliferation, histodif- ferentiation, morphodifferentiation, and apposition. The talon cusp is an anomaly that occurs during morphodifferentiation, and this anomaly may have numerous adverse clinical effects on oral health. The objective of this study was to report a case of “Talon Cusp Type I” and to discuss diagnostic methods, treatment options for this anomaly, and the importance of knowledge of this morphological change among dental professionals so that it is not confused with other morphological changes; such knowledge is required to avoid unnecessary surgical procedures, to perform treatments that prevent caries and malocclusions as well as enhancing aesthetics, and to improve the oral health and quality of life of the patient. -

Talon Cusp: a Case Report and Literature Review 1R Kalpana, 2M Thubashini
OMPJ R Kalpana, M Thubashini 10.5005/jp-journals-10037-1045 CASE REPORT Talon Cusp: A Case Report and Literature Review 1R Kalpana, 2M Thubashini ABSTRACT The prevalence of talon cusp varies with race, age, Talon cusp is a well‑delineated accessory cusp thought to and the criteria used to define this abnormality. A review arise as a result of evagination on the surface of a tooth before of the literature suggests that 75% of the cases are in the calcification has occurred. It is seen projecting from the cin permanent dentition and 25% in the primary dentition. gulum or cementoenamel junction of maxillary or mandibular anterior tooth. It is named due to its resemblance to eagle’s This anomaly has a greater predilection in the maxilla talon, which is the shape of eagle’s claw when hooked on to its (with more than 90% of the cases reported) than in the prey. The incidence is 0.04 to 8%. This article reports a case mandible (only 10% of the cases).7 In the permanent denti- of talon cusp on maxillary permanent lateral incisor. When it occurs on the facial aspect, the effects are mainly esthetic and tion, 55% of the cases involved maxillary lateral incisors, 4,8 functional and so early detection and treatment is essential in 33% involved central incisors and 4% involved canines. its management to avoid complications. The purpose of this article is to report a case of palatal Keywords: Talon cusp, Evagination, Maxillary lateral incisor. talon cusp on the permanent maxillary lateral incisor How to cite this article: Kalpana R, Thubashini M. -

Aging White-Tailed Deer by Tooth Wear and Replacement
Aging White-tailed deer by tooth wear and replacement Aging Characteristics • Physical Characteristics • Antler Size • Number of points not correlated with age • Body size and shape • Neck • Waist • Back • Behavior • Tooth wear and replacement- Harvested Deer Age Classes Born in May and June Fall harvest 6 months- fawn 1.5 yrs- yearling 2.5 yrs 3.5 yrs 4.5 yrs 5.5 yrs 6.5 yrs Tooth Wear The amount of visible dentine is an important factor in determining the age. The tooth wear and replacement method is not 100% accurate however, due to the differences in habitat. Tooth wear on a farmland deer may not be as fast as that of a deep woods buck. Severinghaus (1949) aging method Focus on lower jaw bone Adult deer 3 premolars and 3 molars 6 Months 4 teeth showing. 3rd premolar has three cusps 1.5 yrs •6 teeth •Third premolar •Third molar (last tooth) may still be erupting •Cusps of molars have sharp points. •Inset: Extremely worn third premolar may fool people into thinking deer is older. Actually, this tooth is lost after 1-1/2; years and replaced with a permanent two-cusped premolar. 2.5 yrs •Teeth are permanent •On the first molar (4th tooth) the cusps are sharp • Enamel > dentine • Third cusp (back cusp) of sixth tooth (third molar) is sharp. 3.5 yrs •Cusps show some wear •Dentine now thicker than enamel on cusp of fourth tooth (first molar). •Dentine of fifth tooth (second molar) usually not as wide as enamel. •Back cusp is flattened. 4.5 yrs •Cusp of fourth tooth (first molar) is gone. -

Frequency of Cusp of Carabelli in Orthodontic Patients Reporting to Islamabad Dental Hospital
ORIGINAL ARTICLE POJ 2016:8(2) 85-88 Frequency of cusp of carabelli in orthodontic patients reporting to Islamabad Dental Hospital Maham Niazia, Yasna Najmib, Muhammad Mansoor Qadric Abstract Introduction: Anatomic variation in the anatomy of maxillary molars can have clinical implications in dentistry ranging from predisposition to dental caries or loosely fitting orthodontic bands. The aim of this study was to determine the frequency of cusp of carabelli in permanent first molars of patients reporting to the Orthodontic department. Material and Methods: A total of 698 patients reporting to the Orthodontic Department, Islamabad Dental Hospital, were evaluated from their orthodontic records. Upper occlusal photographs and dental casts of these patients comprised the data. Results: 245 (35.1%) patients showed the presence of the cusp while 453 (64.9%) had no accessory cusp present. Larger proportion of females had cusp of carabelli when compared with males. Bilateralism was found in 75.1% subjects while unilateralism existed in 24.9%, both being higher in females. Among the unilateral cases, higher trend was observed on the right side then the left. Conclusions: It was concluded that the frequency of cusp of carabelli was less in a population sample of Islamabad than other Asian samples, but an opposite trend was seen when compared to a population sample of Khyber Phukhtunkhwa showing different prevalence rates in different ethnicities. Keywords: Cusp of carabelli; maxillary first molars; caries; orthodontic patients Introduction unilaterally or bilaterally. However it he Cusp of Carabelli is a small additional generally appears bilaterally5 but Hirakawa T cusp which is situated on the mesio- and Dietz found ‘rare’ unilateral cases.6 Its palatal surface of first maxillary molars and size varies from being the largest cusp of the tooth to a rudimentary elevation. -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth. -

Anterior and Posterior Tooth Arrangement Manual
Anterior & Posterior Tooth Arrangement Manual Suggested procedures for the arrangement and articulation of Dentsply Sirona Anterior and Posterior Teeth Contains guidelines for use, a glossary of key terms and suggested arrangement and articulation procedures Table of Contents Pages Anterior Teeth .........................................................................................................2-8 Lingualized Teeth ................................................................................................9-14 0° Posterior Teeth .............................................................................................15-17 10° Posterior Teeth ...........................................................................................18-20 20° Posterior Teeth ...........................................................................................21-22 22° Posterior Teeth ..........................................................................................23-24 30° Posterior Teeth .........................................................................................25-27 33° Posterior Teeth ..........................................................................................28-29 40° Posterior Teeth ..........................................................................................30-31 Appendix ..............................................................................................................32-38 1 Factors to consider in the Aesthetic Arrangement of Dentsply Sirona Anterior Teeth Natural antero-posterior -
CHAPTER 5Morphology of Permanent Molars
CHAPTER Morphology of Permanent Molars Topics5 covered within the four sections of this chapter B. Type traits of maxillary molars from the lingual include the following: view I. Overview of molars C. Type traits of maxillary molars from the A. General description of molars proximal views B. Functions of molars D. Type traits of maxillary molars from the C. Class traits for molars occlusal view D. Arch traits that differentiate maxillary from IV. Maxillary and mandibular third molar type traits mandibular molars A. Type traits of all third molars (different from II. Type traits that differentiate mandibular second first and second molars) molars from mandibular first molars B. Size and shape of third molars A. Type traits of mandibular molars from the buc- C. Similarities and differences of third molar cal view crowns compared with first and second molars B. Type traits of mandibular molars from the in the same arch lingual view D. Similarities and differences of third molar roots C. Type traits of mandibular molars from the compared with first and second molars in the proximal views same arch D. Type traits of mandibular molars from the V. Interesting variations and ethnic differences in occlusal view molars III. Type traits that differentiate maxillary second molars from maxillary first molars A. Type traits of the maxillary first and second molars from the buccal view hroughout this chapter, “Appendix” followed Also, remember that statistics obtained from by a number and letter (e.g., Appendix 7a) is Dr. Woelfel’s original research on teeth have been used used within the text to denote reference to to draw conclusions throughout this chapter and are the page (number 7) and item (letter a) being referenced with superscript letters like this (dataA) that Treferred to on that appendix page. -

Prevalence of Dental Anomalies in Indonesian Individuals with Down Syndrome
Pesquisa Brasileira em Odontopediatria e Clínica Integrada 2019; 19:e5332 DOI: http://doi.org/10.4034/PBOCI.2019.191.147 ISSN 1519-0501 ORIGINAL ARTICLE Prevalence of Dental Anomalies in Indonesian Individuals with Down Syndrome Luly Anggraini1, Mochamad Fahlevi Rizal2, Ike Siti Indiarti3 1Faculty of Dentistry, Universitas Indonesia, Jakarta Pusat, Indonesia. 0000-0002-9018-8873 2Department of Pediatric Dentistry, Faculty of Dentistry, Universitas Indonesia, Jakarta Pusat, Indonesia. 0000-0001-6654-7744 3Department of Pediatric Dentistry, Faculty of Dentistry, Universitas Indonesia, Jakarta Pusat, Indonesia. 0000-0001-6776-912X Author to whom correspondence should be addressed: Mochamad Fahlevi Rizal, Department of Pediatric Dentistry, Faculty of Dentistry, Universitas Indonesia, Jalan Salemba Raya No.4, Jakarta Pusat, Jakarta 10430, Indonesia. Phone: +62 81311283838. E-mail: [email protected]. Academic Editors: Alessandro Leite Cavalcanti and Wilton Wilney Nascimento Padilha Received: 24 April 2019 / Accepted: 27 September 2019 / Published: 16 October 2019 Abstract Objective: To determine the frequency distribution of dental anomalies in people with Down syndrome. Material and Methods: This cross-sectional study was developed in Jakarta, Indonesia, and evaluated 174 individuals with Down syndrome aged 14-53 years. Were collected information regarding the tooth number, tooth size, shape, and structure. Descriptive statistics were used to calculate the absolute and relative frequencies. The Pearson chi-square test was used in bivariate analysis. The significance threshold was set at 5%. Results: There were 70 female subjects (40.2%) and 104 male subjects (59.8%) with an average age of 19.2 years. In terms of anomalies of tooth number, hypodontia (80.9%), supernumerary teeth (12.4%), and combined hypodontia and supernumerary teeth (12.4%) were identified. -

Dens Evaginatus of Anterior Teeth (Talon Cusp): Report of Five Cases
Restorative Dentistry Dens evaginatus of anterior teeth (talon cusp): Report of five cases Juan J. Segura-Egea, DDS, MD, PhD1/Alicia Jiménez-Rubio, DDS, MD, PhD2/ José V. Ríos-Santos, DDS, MD, PhD3/Eugenio Velasco-Ortega, DDS, MD, PhD3 The talon cusp, or Dens evaginatus of anterior teeth, is a relatively rare dental developmental anomaly characterized by the presence of an accessory cusplike structure projecting from the cingulum area or ce- mentoenamel junction. This occurs in either maxillary or mandibular anterior teeth in both the primary and permanent dentition. This article reports five cases of talon cusp, two of them bilateral, affecting perma- nent maxillary central and lateral incisors and canines that caused clinical problems related to caries or occlusal interferences. (Quintessence Int 2003;34:xxx–xxx) Key words: dens evaginatus, dental anomalies, occlusal interference, talon cusp ens evaginatus is a developmental anomaly char- volved (67%), followed by the central incisors (24%) Dacterized by the presence of an extra cusp, occur- and canines (9%).7,8 ring more frequently in mandibular premolars.1 In ca- Family histories of cases reported previously re- nines and incisors, Dens evaginatus originates usually vealed that sometimes talon cusp affected patients who in the palatal cingulus as a tubercle projecting from had consanguineous parents.6,9 Moreover, there are sev- the palatal surface; however, the anomaly also has af- eral dates [Au: What is meant by “dates?” Reports?] fected the labial surface of the tooth.2,3 Mitchell4 first in the literature that support the hereditary character of described this dental anomaly as a “process of horn- talon cusp: the anomaly has been described affecting like shape, curving from the base downward to the two siblings,10,11 two sets of female twins,12 and two cutting edge” on the lingual surface of an maxillary family members,9 and the prevalence of talon cusp is central incisor of a female patient. -

Gemination with Talon's Cusp on Mandibular Central Incisor
OLGU SUNUMU / CASE REPORT Gülhane Tıp Derg 2016;58: 105-107 © Gülhane Askeri Tıp Akademisi 2016 doi: 10.5455/gulhane. 162948 Gemination with talon’s cusp on mandibular central incisor: An unusual occurrence Dr Renita Lorina Castelino(*), Anusha Rangare Laxmana(**), Sham Kishor Kannepady(**), Preethi Balan(***), Fazil KA(***) Introduction ÖZET Fetal taşikardi en iyi bilinen non-immun hidrops fetalis nedenidir. Fetal taşikardi A developing tooth can undergo variations and fluctuations tedavi edilmezse hidrops fetalise ve fetal kayıba neden olabilmektedir. Hidrops fetaliste prognoz antiaritmik tedaviye hızlı yanıta, gebelik haftasına, fetusun iyilik during tooth development and can result in various haline ve yüksek kardiyovasküler profil skora (KVPS) bağlıdır. Biz burada SVT’ ye developmental anomalies. It can be either in the primary or sekonder gelişen 28 haftalık hidropslu fetusu olgu olarak sunduk. Biz KVPS’u in the permanent dentition. The terms “double teeth”, “double tartışmak amacıyla bu olgu sunumunu sunduk . Olgumuz da Digoksin ve sotalol [1,2,3] den oluşan kombine maternal antiaritmik tedavinin 1. günde fetal taşikardinin formations”, “joined teeth”, “fused teeth”or “dental twinning” başarılı şekilde sinüs ritmine dönüştüğü izlendi fakat fetusun iyilik hali gittikçe are often used to describe the anomaly of conjoined tooth. The bozulup hidrops fetalis ağırlaştı ve tedavinin 21. günü fetal kayıp gerçekleşti. Fetusun kardiyovasküler profil skoru (KVPS) 7/10 ( cilt ödemi 2 puan, duktus terms like germination, schizodontia, connation, synodontia, venozusta revers atriyal A dalgası 1 puan kayıp) idi. Ve bu yaşamla bağdaşır kabul linking tooth [4] have also been suggested in literature. edilebilir bir skordu. Fakat olgumuzda hayatla bağdaşır (7/10) KVPS olmasına rağmen fetal kayıp oluşmuştur. -

Unusual Case Report of Mandibular Talons Cusp
ACTA SCIENTIFIC DENTAL SCIENCES (ISSN: 2581-4893) Volume 2 Issue 12 December 2018 Case Report Unusual Case Report of Mandibular Talons Cusp Suruchi Kadoo Deshpande1 and Nilesh Deshpande2* 1General Dentist, Sunny Medical Centre, A NMC Company, Sharjah, UAE 2Pediatric Dentist, Sunny Medical Centre, A NMC company, Sharjah, UAE *Corresponding Author: Nilesh Deshpande, Pediatric Dentist, Sunny Medical Centre, A NMC company, Sharjah, UAE. Received: October 08, 2018; Published: November 09, 2018 Abstract Talon cusp is a dental anomaly also known as an Eagle’s talon. It is an additional cusp on an anterior tooth which occurs due to evagination on the surface of a crown before calcification. The exact etiology is unknown. The incidence of talon cusp is very less cases bilateral. Double teeth appearance is a typical radiological diagnostic feature. The anomaly rarely found in mandibular denti- which is even lesser in mandibular anteriors. Maxillary incisors are most commonly involved teeth, usually unilateral but in some tion. This article we are reporting an unusual case of talon cusp of permanent mandibular central incisors. Keywords: Talons Cusp; Anomaly; Evagination Introduction The prevalence of this anomaly in the population varies be- Talon cusp, also known as Eagle’s talon, is a manifestation of tween 1% and 8% [5,6]. It is most frequently found in permanent dens evaginatus in the anterior teeth [1]. The incidence has been 94%. Among the incisors, the laterals (55%) and most affected . found to range from less than 1% to 6% of the population, in which teeth 77%, with the maxillary incisors being the most affected [7] (65%) and may be unilateral or bilateral [8].