(Talon Cusp) on Maxillary Lateral Incisor- a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Management of Anterior Spacing with Peg Lateral by Interdisciplinary Approach : a Case Report
Case Report Management of Anterior Spacing with Peg Lateral by Interdisciplinary Approach : A Case Report Dr Sanjay Prasad Gupta Assistant Professor & Consultant Orthodontist, Department of Orthodontics, Tribhuvan University Teaching Hospital, Institute of Medicine, Kathmandu Correspondence: Dr Sanjay Prasad Gupta; Email: [email protected] ABSTRACT Anterior spacing is a common esthetic problem of patient during dental consultation. The most common etiology include tooth size and arch length discrepancy. Maxillary lateral incisors vary in form more than any other tooth in the mouth except the third molars. Microdontia is a condition where the teeth are smaller than the normal size. Microdontia of maxillary lateral incisor is called as “peg lateral”, that exhibit converging mesial and distal surfaces of crown forming a cone like shape. A carefully documented diagnosis and treatment plan are essential if the clinician is to apply the most effective approach to address the patient’s needs. A patient sometimes requires a multidisciplinary approach to correct the esthetics and to improve the occlusion. This case report describes the management of an adult female patient with a proclined upper anterior teeth, upper anterior spacing, deep bite and peg shaped upper right lateral incisor tooth through orthodontic and restorative treatment approach. Key words: Anterior spacing, Peg lateral, Esthetic, Interdisciplinary approach INTRODUCTION Peg shaped lateral incisors occur in approximately 2% to 5% of the general population, and women show a Maxillary lateral incisors vary in form more than any slightly higher frequency than men. Usually they are found other tooth in the mouth except the third molars. If the equally on the right and left, uni or bilaterally, however variation is too great, it is considered a developmental some studies have shown their bilateral occurrence anomaly.1 Developmental alterations which are most slightly higher than the unilateral occurrence. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Case Report Talon Cusp Type I: Restorative Management
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2015, Article ID 425979, 5 pages http://dx.doi.org/10.1155/2015/425979 Case Report Talon Cusp Type I: Restorative Management Rafael Alberto dos Santos Maia,1 Wanessa Christine de Souza-Zaroni,2 Raul Sampaio Mei,3 and Fernando Lamers2 1 Oral and Maxillofacial Surgery, HGU, University of Cuiaba,´ 78016-000 Cuiaba,´ MT, Brazil 2School of Dentistry, Cruzeiro do Sul University (UNICSUL), 08060-070 Sao˜ Paulo, SP, Brazil 3School of Dentistry, University Center of Grande Dourados (UNIGRAN), 79824-900 Dourados, MS, Brazil Correspondence should be addressed to Wanessa Christine de Souza-Zaroni; [email protected] Received 9 February 2015; Accepted 15 April 2015 Academic Editor: Carla Evans Copyright © 2015 Rafael Alberto dos Santos Maia et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The teeth are formed during intrauterine life (i.e., gestation) during the odontogenesis stage. During this period, the teeth move until they enter the oral cavity. This course covers various stages of dental development, namely, initiation, proliferation, histodif- ferentiation, morphodifferentiation, and apposition. The talon cusp is an anomaly that occurs during morphodifferentiation, and this anomaly may have numerous adverse clinical effects on oral health. The objective of this study was to report a case of “Talon Cusp Type I” and to discuss diagnostic methods, treatment options for this anomaly, and the importance of knowledge of this morphological change among dental professionals so that it is not confused with other morphological changes; such knowledge is required to avoid unnecessary surgical procedures, to perform treatments that prevent caries and malocclusions as well as enhancing aesthetics, and to improve the oral health and quality of life of the patient. -

Talon Cusp: a Case Report and Literature Review 1R Kalpana, 2M Thubashini
OMPJ R Kalpana, M Thubashini 10.5005/jp-journals-10037-1045 CASE REPORT Talon Cusp: A Case Report and Literature Review 1R Kalpana, 2M Thubashini ABSTRACT The prevalence of talon cusp varies with race, age, Talon cusp is a well‑delineated accessory cusp thought to and the criteria used to define this abnormality. A review arise as a result of evagination on the surface of a tooth before of the literature suggests that 75% of the cases are in the calcification has occurred. It is seen projecting from the cin permanent dentition and 25% in the primary dentition. gulum or cementoenamel junction of maxillary or mandibular anterior tooth. It is named due to its resemblance to eagle’s This anomaly has a greater predilection in the maxilla talon, which is the shape of eagle’s claw when hooked on to its (with more than 90% of the cases reported) than in the prey. The incidence is 0.04 to 8%. This article reports a case mandible (only 10% of the cases).7 In the permanent denti- of talon cusp on maxillary permanent lateral incisor. When it occurs on the facial aspect, the effects are mainly esthetic and tion, 55% of the cases involved maxillary lateral incisors, 4,8 functional and so early detection and treatment is essential in 33% involved central incisors and 4% involved canines. its management to avoid complications. The purpose of this article is to report a case of palatal Keywords: Talon cusp, Evagination, Maxillary lateral incisor. talon cusp on the permanent maxillary lateral incisor How to cite this article: Kalpana R, Thubashini M. -

Dental Anomalies: Foundational Articles and Consensus Recommendations, 2021
Dental Anomalies: Foundational Articles and Consensus Recommendations, 2021 Adekoya-Sofowora CA. Natal and neonatal teeth: a review. Niger Postgrad Med J 2008;15:38-41 Al-Ani AH, Antoun JS, Thomson WM, Merriman TR, Farella M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. Biomed Res Int. 2017:9378325. doi.org/10.1155/2017/9378325. Anthonappa RP, King NM, Rabie AB. Aetiology of supernumerary teeth: A literature review. Eur Arch Paediatr Dent. 2013;14:279-88. Dashash, M. Yeung CA, Jamous I, Blinkhorn A. Interventions for the restorative care of amelogenesis imperfecta in children and adolescents. Cochrane Database Syst Rev 2013;6:CD007157. Gallacher A, Ali R, Bhakta S. Dens invaginatus: diagnosis and management strategies. Br Dent J 2016;221:383-7. Gill DS, Barker CS. The multidisciplinary management of hypodontia: a team approach. Br Dent J 2015;218:143-9. Khalaf K, Miskelly J, Voge E, Macfarlane TV. Prevalence of hypodontia and associated factors: a systematic review and meta-analysis. J Orthod. 2014; 41:299-316. Lammi L. Arte S, Somer M, Javinen H, et al. Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am. J. Hum. Genet. 2004, 74:1043–1050. Marvin ML, Mazzoni S, Herron CM, Edwards S, et al. AXIN2-associated autosomal dominant ectodermal dysplasia and neoplastic syndrome. Am J Med Genet A. 2011,155 898–902. Seow WK. Developmental defects of enamel and dentine: Challenges for basic science research and clinical management. Aust Dent J 2014;59:143-54. Shields ED, Bixler D, El-Kafrawy AM. A proposed classification for heritable human dentine defects with a description of a new entity. -

Supernumerary Premolars Associated with Dens Evaginatus: Report of 2 Cases
C LINICAL P RACTICE Supernumerary Premolars Associated with Dens Evaginatus: Report of 2 Cases • Shiu-yin Cho, BDS, MDS • Abstract Dens evaginatus is a dental anomaly found predominantly in people of Mongoloid origin. Dentists practising in Western countries should also be aware of this condition because of the increasing migration of people from Asia. Supernumerary premolars are uncommon but may be found incidentally during radiographic examination of teeth with dens evaginatus. This article reports 2 cases of concomitant occurrence of supernumerary premolars and dens evaginatus. The presence of a supernumerary premolar in 1 quadrant is an indication for radiographic examination of all other premolar regions. MeSH Key Words: bicuspid/anomalies; tooth abnormalities/diagnosis; tooth, supernumerary/diagnosis © J Can Dent Assoc 2005; 71(6):390–93 This article has been peer reviewed. upernumerary teeth are teeth in excess of the number opment.1,14 Environmental factors, however, may also play a found in the normal series.1 The prevalence of super- part. The association of supernumerary premolars with dens S numerary teeth in the permanent dentition of the evaginatus has been reported only infrequently.10 This article white population is about 2% to 3%, and about 90% of all reports 2 cases of concomitant occurrence of supernumerary supernumerary teeth occur in the premaxilla.2–5 premolars and dens evaginatus. Supernumerary premolars have been reported to represent 3% to 9% of all supernumerary teeth, and their prevalence Case Reports ranges from 0.29% to 0.64%.4–7 Case 1 Dens evaginatus is a developmental anomaly that mani- A 12-year-old Chinese girl attended the author’s clinic fests as a tubercle emerging from the surface of the affected for a regular checkup. -

Dens Evaginatus: a Problem-Based Approach
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2015, Article ID 393209, 4 pages http://dx.doi.org/10.1155/2015/393209 Case Report Dens Evaginatus: A Problem-Based Approach A. Ayer,1 M. Vikram,1 and P. Suwal2 1 Department of Conservative Dentistry & Endodontics, B.P. Koirala Institute of Health Sciences, Dharan 56700, Nepal 2Department of Prosthodontics, B.P. Koirala Institute of Health Sciences, Dharan 56700, Nepal Correspondence should be addressed to A. Ayer; [email protected] Received 24 August 2015; Revised 25 November 2015; Accepted 26 November 2015 Academic Editor: Yousef S. Khader Copyright © 2015 A. Ayer et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Dens evaginatus is an uncommon developmental anomaly of human dentition characterized by the presence of tubercle on the occlusal surface of mandibular premolars and lingual surface of anterior teeth. Due to occlusal trauma this tubercle tends to fracture thus exposing the pathway to the pulp chamber of teeth. This case report is about the presentation of dens evaginatus in mandibular premolars bilaterally; among them tooth 44 was associated with chronic apical periodontitis. Fractured tubercle of three premolars was sealed with composite resin. Root canal treatment was performed with tooth 44. Routine endodontic treatment did not result in remission of infection. Therefore, culture and sensitivity tests were performed to identify the cause and modify treatment plan accordingly. Triple antibiotic paste was used as an intracanal medicament to disinfect the root canal that resulted in remission of infection. -

Aging White-Tailed Deer by Tooth Wear and Replacement
Aging White-tailed deer by tooth wear and replacement Aging Characteristics • Physical Characteristics • Antler Size • Number of points not correlated with age • Body size and shape • Neck • Waist • Back • Behavior • Tooth wear and replacement- Harvested Deer Age Classes Born in May and June Fall harvest 6 months- fawn 1.5 yrs- yearling 2.5 yrs 3.5 yrs 4.5 yrs 5.5 yrs 6.5 yrs Tooth Wear The amount of visible dentine is an important factor in determining the age. The tooth wear and replacement method is not 100% accurate however, due to the differences in habitat. Tooth wear on a farmland deer may not be as fast as that of a deep woods buck. Severinghaus (1949) aging method Focus on lower jaw bone Adult deer 3 premolars and 3 molars 6 Months 4 teeth showing. 3rd premolar has three cusps 1.5 yrs •6 teeth •Third premolar •Third molar (last tooth) may still be erupting •Cusps of molars have sharp points. •Inset: Extremely worn third premolar may fool people into thinking deer is older. Actually, this tooth is lost after 1-1/2; years and replaced with a permanent two-cusped premolar. 2.5 yrs •Teeth are permanent •On the first molar (4th tooth) the cusps are sharp • Enamel > dentine • Third cusp (back cusp) of sixth tooth (third molar) is sharp. 3.5 yrs •Cusps show some wear •Dentine now thicker than enamel on cusp of fourth tooth (first molar). •Dentine of fifth tooth (second molar) usually not as wide as enamel. •Back cusp is flattened. 4.5 yrs •Cusp of fourth tooth (first molar) is gone. -

Frequency of Cusp of Carabelli in Orthodontic Patients Reporting to Islamabad Dental Hospital
ORIGINAL ARTICLE POJ 2016:8(2) 85-88 Frequency of cusp of carabelli in orthodontic patients reporting to Islamabad Dental Hospital Maham Niazia, Yasna Najmib, Muhammad Mansoor Qadric Abstract Introduction: Anatomic variation in the anatomy of maxillary molars can have clinical implications in dentistry ranging from predisposition to dental caries or loosely fitting orthodontic bands. The aim of this study was to determine the frequency of cusp of carabelli in permanent first molars of patients reporting to the Orthodontic department. Material and Methods: A total of 698 patients reporting to the Orthodontic Department, Islamabad Dental Hospital, were evaluated from their orthodontic records. Upper occlusal photographs and dental casts of these patients comprised the data. Results: 245 (35.1%) patients showed the presence of the cusp while 453 (64.9%) had no accessory cusp present. Larger proportion of females had cusp of carabelli when compared with males. Bilateralism was found in 75.1% subjects while unilateralism existed in 24.9%, both being higher in females. Among the unilateral cases, higher trend was observed on the right side then the left. Conclusions: It was concluded that the frequency of cusp of carabelli was less in a population sample of Islamabad than other Asian samples, but an opposite trend was seen when compared to a population sample of Khyber Phukhtunkhwa showing different prevalence rates in different ethnicities. Keywords: Cusp of carabelli; maxillary first molars; caries; orthodontic patients Introduction unilaterally or bilaterally. However it he Cusp of Carabelli is a small additional generally appears bilaterally5 but Hirakawa T cusp which is situated on the mesio- and Dietz found ‘rare’ unilateral cases.6 Its palatal surface of first maxillary molars and size varies from being the largest cusp of the tooth to a rudimentary elevation. -

Molar-Incisor Hypomineralization and Delayed Tooth Eruption
Winter 2017, Volume 6, Number 4 Case Report: Mandibular Talon Cusp Associated With Molar-Incisor Hypomineralization and Delayed Tooth Eruption ٭Katayoun Salem1 , Fatemeh Moazami2, Seyede Niloofar Banijamali3 1. Assistant Professor, Department of Pediatric Dentistry, Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. 2. Pedodontist, Tehran, Iran. 3. Postgraduate Student, Department of Pediatric Dentistry, Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. Use your device to scan and read the article online Citation: Salem K, Moazami F, Banijamali SN. Mandibular Talon Cusp Associated With Molar-Incisor Hypomineralization and Delayed Tooth Eruption. Journal of Dentomaxillofacial Radiology, Pathology and Surgery. 2017; 6(4):141-145. : http://dx.doi.org/10.32598/3dj.6.4.141 Funding: See Page 144 Copyright: The Author(s) A B S T R A C T Talon cusp is an odontogenic anomaly in anterior teeth, caused by hyperactivity of enamel Article info: in morphodifferentiation stage. Talon cusp is an additional cusp with several types based on Received: 25 Aug 2017 its extension and shape. It has enamel, dentin, and sometimes pulp tissue. Moreover, it can Accepted: 20 Nov 2017 cause clinical problems such as poor aesthetic, dental caries, attrition, occlusal interferences, Available Online: 01 Dec 2017 and periodontal diseases. Therefore, early diagnosis and effective treatment of talon cusp are essential. Maxillary incisors are the most commonly affected teeth. However, occurrence of mandibular talon cusp is a rare entity. We report a talon cusp in the lingual surface of the permanent mandibular left central incisor, in a 7-year-old Iranian boy. To our knowledge it is Keywords: the third case reported in Iranian patients. -

Dens Evaginatus and Dens Invaginatus in Maxillary Lateral Incisor: Report of Two Cases
10.5005/jp-journals-10026-1037 ParasCASE Mull REPORT Gehlot et al Concurrent Occurrence of Developmental Anomalies— Dens Evaginatus and Dens Invaginatus in Maxillary Lateral Incisor: Report of Two Cases Paras Mull Gehlot, Vinutha Manjunath, MK Manjunath ABSTRACT • Type II (Semitalon): An additional cusp of a millimeter or Developmental anomalies affecting tooth morphology are common more but extending less than half the distance from the in the literature. Dens evaginatus (DE) occurring in anterior tooth, CEJ to the incisal edge. termed ‘talon cusp’ is a relatively rare developmental anomaly. It • Type III (Trace talon): Enlarged or prominent cingula and presents as an additional cusp that project predominantly from their variations, i.e. conical, bifid or tubercle-like. the lingual surface of primary or permanent anterior teeth. Dens invaginatus (DI) is a developmental anomaly resulting from infolding Histologically, it is composed of normal enamel and dentin of the tooth crown or root before calcification has occurred. and it may or may not contain pulpal tissue.2 Clinically DE Concurrent occurrence of DE and DI within the same tooth is 4 rare. The present article reports two cases with concurrent can pose esthetic and functional problems to the patient. occurrence of DE and DI in permanent maxillary lateral incisor. In Dens invaginatus (DI) is a developmental anomaly due to case 1 the DE and DI are associated with nonvital tooth and in a deepening or invagination of the enamel organ into the case 2 the DE and DI are associated with a vital tooth. The dental papilla prior to calcification of the dental tissues.5 management aspects are discussed. -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
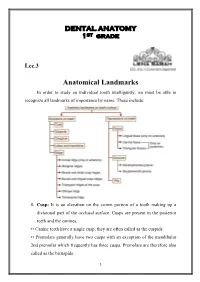
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth.