Actinic Keratosis Squamous Cell Carcinoma in Situ
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paraneoplastic Syndrome Presenting As Giant Porokeratosis in a Patient with Nasopharyngeal Cancer
Paraneoplastic Syndrome Presenting As Giant Porokeratosis in A Patient with Nasopharyngeal Cancer Fitri Azizah, Sonia Hanifati, Sri Adi Sularsito, Lili Legiawati, Shannaz Nadia Yusharyahya, Rahadi Rihatmadja Department of Dermatology and Venereology, Faculty of Medicine Universitas Indonesia / Dr. Cipto Mangunkusumo National General Hospital Keywords: porokeratosis, giant porokeratosis, paraneoplastic syndrome, nasopharyngeal Abstract: Giant porokeratosis is a rare condition in which the hyperkeratotic plaques of porokeratosis reach up to 20 cm in diameter. Porokeratosis is characterized clinically by hyperkeratotic papules or plaques with a thread-like elevated border. Although rare, porokeratosis has been reported in conjunction with malignancies suggesting a paraneoplastic nature. Associated malignancies reported were hematopoietic, hepatocellular, and cholangiocarcinoma. We report a case of giant porokeratosis in a patient with nasopharyngeal cancer responding to removal of the primary cancer by chemoradiotherapy. 1 INTRODUCTION regress completely after the treatment of malignancy, suggestive of paraneoplastic syndrome. Porokeratosis is a chronic progressive disorder of keratinization, characterized by hyperkeratotic papules or plaques surrounded by a thread-like 2 CASE elevated border corresponds to a typical histologic hallmark, the cornoid lamella . O regan, 2012) There Mr. SS, 68-year-old, was referred for evaluation of are at least six clinical variants of porokeratosis pruritic, slightly erythematous plaques with raised, recognized with known genetic disorder.1 Some hyperpigmented border of one and a half year clinical variant of porokeratosis has been reported in duration on the extensor surface of both legs. The the setting of immunosuppressive conditions, organ lesions shown minimal response to potent topical transplantation, use of systemic corticosteroids, and corticosteroids and phototherapy given during the infections, suggesting that impaired immunity may last 8 months in another hospital. -

Features of Reactive White Lesions of the Oral Mucosa
Head and Neck Pathology (2019) 13:16–24 https://doi.org/10.1007/s12105-018-0986-3 SPECIAL ISSUE: COLORS AND TEXTURES, A REVIEW OF ORAL MUCOSAL ENTITIES Frictional Keratosis, Contact Keratosis and Smokeless Tobacco Keratosis: Features of Reactive White Lesions of the Oral Mucosa Susan Müller1 Received: 21 September 2018 / Accepted: 2 November 2018 / Published online: 22 January 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract White lesions of the oral cavity are quite common and can have a variety of etiologies, both benign and malignant. Although the vast majority of publications focus on leukoplakia and other potentially malignant lesions, most oral lesions that appear white are benign. This review will focus exclusively on reactive white oral lesions. Included in the discussion are frictional keratoses, irritant contact stomatitis, and smokeless tobacco keratoses. Leukoedema and hereditary genodermatoses that may enter in the clinical differential diagnoses of frictional keratoses including white sponge nevus and hereditary benign intraepithelial dyskeratosis will be reviewed. Many products can result in contact stomatitis. Dentrifice-related stomatitis, contact reactions to amalgam and cinnamon can cause keratotic lesions. Each of these lesions have microscopic findings that can assist in patient management. Keywords Leukoplakia · Frictional keratosis · Smokeless tobacco keratosis · Stomatitis · Leukoedema · Cinnamon Introduction white lesions including infective and non-infective causes will be discussed -

Progressive Widespread Warty Skin Growths
DERMATOPATHOLOGY DIAGNOSIS Progressive Widespread Warty Skin Growths Patrick M. Kupiec, BS; Eric W. Hossler, MD Eligible for 1 MOC SA Credit From the ABD This Dermatopathology Diagnosis article in our print edition is eligible for 1 self-assessment credit for Maintenance of Certification from the American Board of Dermatology (ABD). After completing this activity, diplomates can visit the ABD website (http://www.abderm.org) to self-report the credits under the activity title “Cutis Dermatopathology Diagnosis.” You may report the credit after each activity is completed or after accumu- lating multiple credits. A 33-year-old man presented with progres- sive widespread warty skin growths that had been present copysince 6 years of age. Physical examination revealed numerous verrucous papules on the face and neck along with Figure 1. H&E, original magnification ×40. Figure 2. H&E, original magnification ×40. verrucous, tan-pink papules and plaques diffuselynot scattered on the trunk, arms, and legs. A biopsy of a lesion on the neck Dowas performed. H&E, original magnification ×200. The best diagnosisCUTIS is: a. condyloma acuminatum b. epidermodysplasia verruciformis c. herpesvirus infection d. molluscum contagiosum e. verruca vulgaris PLEASE TURN TO PAGE 99 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Mr. Kupiec is from the State University of New York (SUNY) Upstate Medical University, Syracuse. Dr. Hossler is from the Departments of Dermatology and Pathology, Geisinger Medical Center, Danville, Pennsylvania. The authors report no conflict of interest. Correspondence: Patrick M. Kupiec, BS, 50 Presidential Plaza, Syracuse, NY 13202 ([email protected]). 82 CUTIS® WWW.CUTIS.COM Copyright Cutis 2017. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. -
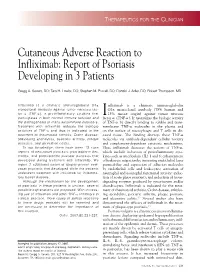
Cutaneous Adverse Reaction to Infliximab: Report of Psoriasis Developing in 3 Patients
THERAPEUTICS FOR THE CLINICIAN Cutaneous Adverse Reaction to Infliximab: Report of Psoriasis Developing in 3 Patients Gregg A. Severs, DO; Tara H. Lawlor, DO; Stephen M. Purcell, DO; Donald J. Adler, DO; Robert Thompson, MD Infliximab is a chimeric immunoglobulin G1k nfliximab is a chimeric immunoglobulin monoclonal antibody against tumor necrosis fac- G1k monoclonal antibody (75% human and tor a (TNF-a), a proinflammatory cytokine that I 25% mouse origin) against tumor necrosis participates in both normal immune function and factor a (TNF-a). It neutralizes the biologic activity the pathogenesis of many autoimmune disorders. of TNF-a by directly binding to soluble and trans- Treatment with infliximab reduces the biologic membrane TNF-a molecules in the plasma and activities of TNF-a and thus is indicated in the on the surface of macrophages and T cells in dis- treatment of rheumatoid arthritis, Crohn disease, eased tissue. The binding destroys these TNF-a ankylosing spondylitis, psoriatic arthritis, plaque molecules via antibody-dependent cellular toxicity psoriasis, and ulcerative colitis. and complement-dependent cytotoxic mechanisms. To our knowledge, there have been 13 case Thus, infliximab decreases the actions of TNF-a, reports of new-onset psoriasis, psoriasiform der- which include induction of proinflammatory cyto- matitis, and palmoplantar pustular psoriasis that kines such as interleukins (IL) 1 and 6; enhancement developed during treatment with infliximab. We of leukocyte migration by increasing endothelial layer report 3 additional cases of biopsy-proven new- permeability and expression of adhesion molecules onset psoriasis that developed while the patients by endothelial cells and leukocytes; activation of underwent treatment with infliximab for inflamma- neutrophil and eosinophil functional activity; induc- tory bowel disease. -

Incidental Focal Acantholytic Dyskeratosis in the Setting of Rosacea
Letter to the Editor http://dx.doi.org/10.5021/ad.2013.25.4.518 Incidental Focal Acantholytic Dyskeratosis in the Setting of Rosacea Sang-Yeon Park, Hae Jin Lee, Jae Yong Shin, Sung Ku Ahn Department of Dermatology, Yonsei University Wonju College of Medicine, Wonju, Korea Dear Editor: direct immunofluorescence (Fig. 2). In the serial sections, Focal acantholytic dyskeratosis (FAD) was first described we observe the same findings. Differential diagnosis for by Ackerman1 in 1972 as a distinct histopathological pat- the possibility of polymorphous light eruption, systemic tern associated with various cutaneous conditions, and lupus erythematosus, contact dermatitis, and dermatitis with classic histopathological findings including supra- artefacta should be considered. But given these clinical basal clefting, hyperkeratosis and parakeratosis, and the and histopathological features, a diagnosis of rosacea with presence of acantholytic and dyskeratotic cells at the FAD was reached. The patient was then admitted to epidermis. While FAD can be observed in many various hospital for treatment with doxycycline 100 mg and cutaneous lesions including benign and/or malignant antihistamines. After one week, the lesions had remarka- epithelial lesions, fibrohistiocytic lesions, inflammatory bly improved. The patient was then discharged, and lesions, melanocytic and/or follicular lesions2-4. These continued on the same therapeutic regimen for an histopathological findings may also extend into the additional month, bythe time all lesions were nearly surrounding tissues, which often appear to be clinically resolved. normal. A 42-year-old woman was presented to our To date, the etiology of FAD has been attributed to department with multiple erythematous pruritic papules numerous sources including hormones, viral infection, and tiny vesicles on her face. -

Diffuse Drug-Induced Dermatitis Following Sclerotherapy for Telangiectasias Libby MW, Caitlin WH, Deniz OA and Heller JA*
Case Report iMedPub Journals Journal of Vascular and Endovascular Surgery 2016 http://www.imedpub.com/ Vol.1 No.3:17 DOI: 10.21767/2573-4482.100017 Diffuse Drug-Induced Dermatitis following Sclerotherapy for Telangiectasias Libby MW, Caitlin WH, Deniz OA and Heller JA* Department of Surgery, Johns Hopkins Vein Center, Johns Hopkins Medical Centers, Baltimore, USA *Corresponding author: Jennifer A Heller, 10755 Falls Road, Pavilion 1 Suite 360, Lutherville, MD 21903, Tel: 4105500415; Email: [email protected] Received date: June 14, 2016; Accepted date: July 26, 2016; Published date: August 02, 2016 Copyright: © 2016 Libby MW, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Sclerotherapy is an effective treatment modality for the management of lower extremity telangiectasias. Although localized dermatologic reactions are known complications of this procedure, systemic reactions are rare. Here, we present a case of a diffuse drug eruption following sclerotherapy for the treatment of bilateral lower extremity telangiectasias. Salient clinical and physical exam findings are described. Management strategies for the treatment of drug eruptions are outlined. This is the first case report that we know of describing a diffuse drug eruption associated with sclerotherapy. It is important to recognize the possibility of diffuse drug eruptions secondary to sclerotherapy treatment so that expectant management may be initiated expeditiously in affected patients. Figure 1: Drug eruption following sclerotherapy. The patient was referred for evaluation by a dermatologist, Case Report who initially diagnosed diffuse dermatitis based on clinical A 64-year-old woman with hypertension and bilateral lower exam. -

Trichoscopic Findings in Various Scalp Alopecias Unilateral Truncal Acne A�Er Laminectomy Armoured Keloid Werner's Syndrome: a Rare En�Ty
JDA IJCD Indian Journal of Clinical Dermatology ` 800 - Jaipur Volume 2 | Issue 1 | May 2019 Four Monthly HIGHLIGHTS Sunscreens: The Current Scenario Trichoscopic Findings in Various Scalp Alopecias Unilateral Truncal Acne Aer Laminectomy Armoured Keloid Werner's Syndrome: A Rare Enty Clin of ica al l D rn e u r o m J a t n o a l i o d g n y I A Publication of Jaipur Dermatology Association Clin of ica JDA al l D rn e u r o m J a t n o INDIAN JOURNAL OF a l i o d g n y I CLINICAL DERMATOLOGY A Publication of Jaipur Dermatology Association EDITORIAL BOARD EDITORS DR. DINESH MATHUR DR. U S AGARWAL Prof & Head, Dept. of Skin, JNU Medical College Senior Professor, Ex. Sr. Prof & Head, Dept. of Skin, Dept. of Skin, STD & Leprosy STD & Leprosy, SMS Medical College Ex. Principal & Controller, Ex. Pro VC, RUHS SMS Medical College & Hospital, Jaipur Email: [email protected] Email: [email protected] EXECUTIVE EDITOR Dr. Puneet Agarwal Assistant Professor, Dept. of Skin, STD & Leprosy, SMS Medical College & Hospital, Jaipur Email: [email protected] ASSISTANT EDITORS Dr. Naushin Aara Assistant Professor Dept. of Skin, STD & Leprosy, SMS Medical College & Hospital, Jaipur Email: [email protected] Dr. Taniya Mehta Ex. Senior Resident Dept. of Skin, STD & Leprosy, SMS Medical College & Hospital, Jaipur Email: [email protected] JDA Indian Journal of Clinical Dermatology | Volume 02 | Issue 01 | May 2019 i Clin of ica JDA al l D rn e u r o m J a t n o INDIAN JOURNAL OF a l i o d g n y I CLINICAL DERMATOLOGY A Publication of Jaipur Dermatology Association Volume 02 | Issue 01 | August 2019 COPYRIGHT The entire contents of the Indian Journal of Clinical Dermatology are protected under Indian and International copyrights. -

Oral Cavity 3 J.W
Chapter 3 Oral Cavity 3 J.W. Eveson Contents 3.1 Embryonic Rests and Heterotopias . 72 3.5.4 Addison Disease . 88 3.1.1 Fordyce Granules/Spots . 72 3.5.5 Peutz Jeghers Syndrome . 89 3.1.2 Juxtaoral Organ of Chievitz . 72 3.5.6 Racial Pigmentation . 89 3.5.7 Laugier Hunziker Syndrome . 89 3.2. Vesiculo-Bullous Diseases . 72 3.5.8 Smoker’s Melanosis . 89 3.2.1 Herpes Simplex Infections . 72 3.5.9 Drug-Associated Oral Pigmentation . 90 3.2.2 Chickenpox and Herpes Zoster . 73 3.2.3 Hand-Foot-and-Mouth Disease . 73 3.6 Hyperplastic Lesions . 90 3.2.4 Herpangina . 74 3.6.1 Fibrous Hyperplasias . 90 3.2.5 Pemphigus Vulgaris . 74 3.6.2 Papillary Hyperplasia . 90 3.2.6 Pemphigus Vegetans . 74 3.6.3 Generalised Gingival Fibrous Hyperplasia . 91 3.2.7 Paraneoplastic Pemphigus . 75 3.6.4 Crohn’s Disease . 91 3.2.8 Mucous Membrane Pemphigoid . 75 3.6.5 Orofacial Granulomatosis . 92 3.2.9 Dermatitis Herpetiformis . 76 3.6.6 Chronic Marginal Gingivitis 3.2.10 Linear IgA Disease . 76 and Localised Gingival Fibrous Hyperplasia . 92 3.2.11 Erythema Multiforme . 77 3.6.7 Peripheral Giant Cell Granuloma (Giant Cell Epulis) . 93 3.3 Ulcerative Lesions . 77 3.6.8 Pyogenic Granuloma . 93 3.3.1 Aphthous Stomatitis 3.6.9 Pulse (Vegetable) Granuloma . 93 (Recurrent Aphthous Ulceration) . 77 3.3.2 Behçet Disease . 78 3.7 Benign Tumours and Pseudotumours . 94 3.3.3 Reiter Disease . 78 3.7.1 Giant Cell Fibroma . -

Pigmented Actinic Keratosis: Case Report and Review of an Uncommon Actinic Keratosis Variant That Can Mimic Melanoma
Open Access Case Report DOI: 10.7759/cureus.4721 Pigmented Actinic Keratosis: Case Report and Review of an Uncommon Actinic Keratosis Variant that can Mimic Melanoma Boya Abudu 1 , Antoanella Calame 2 , Philip R. Cohen 3 1. Internal Medicine, Kaiser Permanente Oakland Medical Center, Oakland, USA 2. Dermatology, Compass Dermatopathology, Inc., San Diego, USA 3. Dermatology, San Diego Family Dermatology, National City, USA Corresponding author: Boya Abudu, [email protected] Abstract Pigmented actinic keratosis is an uncommon variant of actinic keratosis that can mimic melanocytic lesions. A 54-year-old man who presented with a dark lesion on his nasal tip is described; biopsy of the lesion revealed a pigmented actinic keratosis that was treated with cryotherapy using liquid nitrogen. Pigmented actinic keratoses typically appear on sun-exposed areas of the skin as flat hyperpigmented lesions that grow in a centrifugal pattern. Dermoscopy reveals one or more pseudonetworks with hyperpigmented dots or globules. Histopathology shows atypical keratinocytes in the epidermal basal layer and increased melanin content in the epidermis and dermis. Treatment options include liquid nitrogen cryotherapy for solitary lesions and curettage, 5-fluorouracil, imiquimod, ingenol mebutate, photodynamic therapy, or superficial peels for extensive lesions. Categories: Dermatology, Pathology Keywords: actinic, immunoperoxidase, keratosis, lentigo, maligna, malignant, melanoma, pigmented, solar, spreading Introduction Pigmented actinic keratosis is an uncommon clinical variant of actinic keratosis [1-18]. This precancerous lesion can mimic not only melanocytic lesions but also other epithelial tumors [7-8,16-18]. The clinical and pathologic features of an actinic keratosis on the nasal tip of a man are described and the characteristics of this unique lesion are reviewed. -

In Psoriasis and Occurrence of Ψ-3 Antigen in Other Cutaneo
0022- 202X /85/8402-0l 00$02.00/ 0 THE JOURNAL OF INVESTIGATIVE DERMATOLOGY, 84 :100- 104 , 1985 Vol. 84, No.2 Copyright © 1985 by The Williams & Wilkins Co. Printed in U.S.A. Histologic Distribution of Staining by a Monoclonal Antibody ('1'-3) in Psoriasis and Occurrence of '1'-3 Antigen in Other Cutaneous Diseases AARON M . 8TREFLING, M.D., A. MERRILL KNAPP, B.A., AND JONATHAN N. MANSBRIDGE, PH.D. Department of Dermatology, Stanford University School of M edicine, Stanford, California, and Psoriasis Research Institute, Palo Alto, California., U.S.A. ~-3 is a monoclonal antibody that recognizes a does not correlate with any single histologic characteristic. The 135,000 molecular weight structural component of ma antibody appears to define a unique feature in the keratinocyte turing keratinocytes in psoriasis (the 'lt-3 antigen) but response to certain pathologic conditions. It may, thus, be a fails to bind to any constituent of keratinocytes in nor valuable addition to the array of antibodies reacting with the mal epidermis. This paper describes the occurrence of different keratins [16- 19) and other structural components. the ~-3 antigen in a variety of dermatopathologic con The study described in this paper was undertaken to charac ditions using immunoperoxidase (biotin-avidin-peroxi terize the range of benign and malignant dermatologic condi dase) and immunofluorescence methods which show ex tions under which t he W-3 antigen is expressed. cellent concordance. In 35 of 36 specimens of psoriasis vulgaris, 'lt-3 anti body consistently immunolabels the cytoplasm of kerat MATERIALS AND METHODS inocytes above the basal layer. -

The Best Diagnosis Is: A
DERMATOPATHOLOGY DIAGNOSIS H&E, original magnification ×40. The best diagnosis is: a. lichen striatus copy b. linear epidermolytic hyperkeratosis c. linear lichen planus d. linear porokeratosisnot e. linear psoriasis Do A H&E, original magnification ×CUTIS40. B H&E, original magnification ×200 for both. PLEASE TURN TO PAGE 120 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Jacqueline N. Graham, BS; Eric W. Hossler, MD Ms. Graham is from Northeast Ohio Medical University, Rootstown. Dr. Hossler is from the Departments of Dermatology and Pathology, Geisinger Medical Center, Danville, Pennsylvania. The authors report no conflict of interest. Correspondence: Jacqueline N. Graham, BS, 4249 Pine Dr, Rootstown, OH 44272 ([email protected]). 86 CUTIS® WWW.CUTIS.COM Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Dermatopathology Diagnosis Discussion Lichen Striatus ichen striatus (LS) is a benign, uncommon, self-limited, linear inflammatory skin disorder Lthat primarily affects children up to 15 years of age, most commonly around 2 to 3 years of age, and is seen more frequently in girls.1 It presents with a sudden eruption of asymptomatic small, flat- topped, lichenoid, scaly papules in a linear array on a single extremity. The lesions may be erythematous, flesh colored, or hypopigmented.1,2 Multiple lesions appear over days to weeks and coalesce into linear plaques in a continuous or interrupted pattern along the lines of Blaschko, indicating possible -

WSC 14-15 Conf 7 Layout
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2014-2015 Conference 7 22 October 2014 CASE I: B13-962 (JPC 4049563). performed at that time. The dog presented again in July 2013 with continued hematuria. On Signalment: 10-year-old spayed female Welsh ultrasound, the left renal cortex had a 2.2 cm, corgi dog, Canis familiaris. round, heterogeneous mass with multiple, internal, anechoic regions. History: The dog presented in 2011 for a 6-week history of hematuria. Urine culture was negative Gross Pathology: The renal cortex was and no signs of uroliths were seen on radiographs. extensively disrupted by coalescing, dark red, Ultrasound revealed two, 1.7 mm, mineralized blood-filled nodules ranging from 0.7 x 0.5 x 0.2 foci in the left renal pelvis, but the kidneys were cm to 2.5 x 2 x 2 cm. normal in shape and size. No further workup was Histopathologic Description: Kidney: The renal interstitium is markedly expanded by many, severely dilated, blood-filled vascular spaces lined by mature endothelial cells surrounded by abundant fibrous tissue. Some vascular spaces contain thrombi with fibrin arranged as lines of Zahn separated by red and white blood cells that are occasionally attached to the vascular wall by fibrous tissue. The intervening and adjacent renal parenchyma is markedly atrophic with replacement of many nephrons by fibrosis, many lymphocytes and plasma cells, and variable 1-1. Kidney, Welsh corgi: The cortex is expanded by large, ectatic, thin-walled vessels which efface renal parenchyma. (HE 6.3X) hemorrhage. Remaining tubules 1 WSC 2014-2015 1-2.