A Longitudinal Analysis on the Prevalence of Overweight and Underweight Students in Aomori Prefecture in Relation to Gender, Birth Year and District
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
View Oirase’S Fresh Greenery in Spring and the Changing Colors of Tsutanuma in Autumn
Aomori’s Nature Parks Majestic & Breathtaking Aomori Nature Parks Website http://www.shirakami-visitor.jp/aomoris-nature-parks The eternal colors of the four seasons continuing into future 01 The Milky Way at the Kayano Highlands Towada-Hachimantai National Park Aomori is an unexplored location in the north with flowers blossoming in spring and the blue ocean shining in summer. When the trees turn a burning red in autumn, it will soon be winter, a world of white and silver. The incredible scenery of mother nature will steal your heart. Be in awe of nature As one interacts with nature, slowly walking along a mountain road or shore, one begins to feel in awe of nature’s majesty. Enclosed by the ocean on three sides, Shimokita Hanto Aomori’s the climate differs between the Sea of Japan side and Quasi-National Park the Pacific Ocean side, allowing Aomori to boast of a wide variety of landscapes and plants. Nature Parks Aomori has 11 nature parks with outstanding scenery. Sanriku Fukko Towada-Hachimantai Tsugaru (Reconstruction) Quasi-National Park National Park National Park Asamushi-Natsudomari Ashino Chishogun Prefectural Natural Park Prefectural Natural Park National Park Iwaki Kogen Prefectural Natural Park Towada-Hachimantai National Park Shimokita Hanto Tsugaru Quasi-National Park Quasi-National Park Shirakami-Sanchi Natural World Heritage Site Kuroishi Onsenkyo Prefectural Natural Park Sanriku Fukko Tsugaru Shirakami (Reconstruction) Prefectural Natural Park Quasi-National Park National Park Owani Ikarigaseki Onsenkyo Nakuidake Prefectural -

Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-On Kai Museum of Natural History
Bull. Natl. Mus. Nat. Sci., Ser. A, 35(1), pp. 9–54, March 22, 2009 Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-on Kai Museum of Natural History Keiichi Matsuura1, Gento Shinohara2 and Masanori Nakae1 1 Collection Center, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected]; [email protected] 2 Department of Zoology, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected] Abstract The fish collection of the Saito Ho-on Kai Museum of Natural History was transferred to the National Museum of Nature and Science, Tokyo in February 2006. Ninety percent of the fish collection contains specimens collected from the Tohoku District during the period from 1930 to 1933 when natural environments of Japan were in good condition for various groups of fishes. The fish specimens from the Tohoku District were classified into 361 species/subspecies of 273 genera belonging to 131 families of 31 orders. A list of the species is shown with remarks on distribution. Key words: Fish specimens, Saito Ho-on Kai Museum, Tohoku District, inventory. stead of natural sicence. The museum has tried to Introduction keep its activity at the level before the war, but it The Saito Ho-on Kai Museum was established failed to do so because of financial difficulties. In in November 1933 in Sendai City, Miyagi Pre- 2005, the Saito Ho-on Kai Museum of Natural fecture, Japan. -
Wine, Beer, Whisky, Etc
Current as of January 1, 2021 Compiled by Sendai Regional Taxation Bureau Brewery Excludes breweries listed on the Aomori Wine, Beer, "Aomori Brewery MAP (SAKE)". MAP whisky, etc. However, breweries that produce continuously distilled shochu (New type or shochu group Ko), specialty shochu (Authentic type or shochu group Otsu), and beer are listed in duplicate. Legend ㉑ 279 Shinkansen Kazamaura JR Line Oma Private Railway Town Village Expressway Major National Highway City Boundary Sai Shinkansen Station JR and Private Railway Stations Village Higashidoori Mutsu City Village Ominato Station Shimokita Station 279 Ominato Line Imabetsu 338 ⑳ Town Sotogahama Town Nakadomari Okutsugaru-Imabetsu Station Town 338 Sotogahama Yokohama Goshogawara TsugaruTown Line Town City Kanita Station Yomogita Nakadomari Village Town Hokkaido Shinkansen Rokkasho 339 280 ①② Village 4 Noheji ⑲ Goshogawara Aomori Port Station Tsugaru City Hiranai Town City Shin-Aomori Aomori Station Noheji Town Tohoku Ajigasawa Station 101 Goshogawara Town Station Aoimori Railway394 Line Station Ou Misawa Main 103 4 Line Shichinohe-Towada City Tsuruta 338 Town ⑰ Aomori Airport Station Itayanagi Shichinohe Misawa Airport Itayanagi Town Namioka Station Aomori City Town Tohoku Shinkansen Station 394 Misawa Station Ajigasawa Town Fujisaki Kuroishi Kawabe Station Town Station 394 Oirase Town Fukaura Station Hirosaki Inakadate Hachinohe Port City ④ VillageKonan ③ Railway Kuroishi 102 Rokunohe 45 Gono Line Fukaura ⑤ City Hon- ⑯ ⑦ Hiraka 4 Town Town Towada City ⑱ Hachinohe Same Station ⑧ Station Station ⑪ ⑨ 454 Hachinohe Hirosaki Station Station ⑬ Mutsu-Minato Station Nishimeya Hirakawa Hachinohe Line Village Gonohe Town Owani⑫ City 454 ⑥⑩ Town ⑮ 7 282 Shingo Village ⑭ Hashikami Nanbu Hachinohe Town Town City Sannohe Town Name of City, Town, and Village No. -
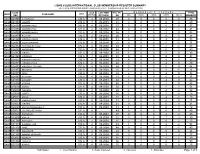
Lions Clubs International Club Membership Register Summary the Clubs and Membership Figures Reflect Changes As of September 2004
LIONS CLUBS INTERNATIONAL CLUB MEMBERSHIP REGISTER SUMMARY THE CLUBS AND MEMBERSHIP FIGURES REFLECT CHANGES AS OF SEPTEMBER 2004 CLUB CLUB LAST MMR FCL YR MEMBERSHI P CHANGES TOTAL DIST IDENT NBR CLUB NAME STATUS RPT DATE OB NEW RENST TRANS DROPS NETCG MEMBERS 5485 024946 AJIGASAWA 332 A 4 09-2004 28 0 0 0 0 0 28 5485 024953 AOMORI 332 A 4 09-2004 61 2 0 0 0 2 63 5485 024954 AOMORI CHUO 332 A 4 09-2004 57 0 0 0 0 0 57 5485 024955 AOMORI UTOU 332 A 4 09-2004 43 0 0 0 -2 -2 41 5485 024956 AOMORI HAKKO 332 A 4 09-2004 58 2 0 0 -2 0 58 5485 024959 FUJISAKI 332 A 4 09-2004 20 1 0 0 0 1 21 5485 024960 HIROSAKI CHUO 332 A 4 09-2004 41 0 0 0 -3 -3 38 5485 024961 GOSHOGAWARA 332 A 4 09-2004 72 0 0 0 -1 -1 71 5485 024962 HACHINOHE CHUO 332 A 4 09-2004 69 0 0 0 -1 -1 68 5485 024963 HACHINOHE 332 A 4 09-2004 48 1 0 0 0 1 49 5485 024967 HIRAKA 332 A 4 09-2004 33 1 0 0 -1 0 33 5485 024969 HIROSAKI 332 A 4 09-2004 84 0 0 0 0 0 84 5485 024970 HIROSAKI CHERRY 332 A 4 09-2004 53 4 0 0 0 4 57 5485 024971 HIROSAKI TO O 332 A 4 09-2004 40 2 0 0 -2 0 40 5485 024972 HIROSAKI TSUGARU 332 A 4 08-2004 64 0 0 0 0 0 64 5485 024975 IMABETSU 332 A 4 09-2004 25 1 0 0 -2 -1 24 5485 024979 IWAKI 332 A 4 09-2004 38 2 0 0 -2 0 38 5485 024987 KIZUKURI 332 A 4 09-2004 31 0 0 0 0 0 31 5485 024989 KUROISHI 332 A 4 07-2004 62 1 0 1 -2 0 62 5485 024994 MISAWA 332 A 4 09-2004 45 1 0 0 -1 0 45 5485 025002 MUTSU 332 A 4 09-2004 50 2 0 0 -1 1 51 5485 025003 NAMIOKA 332 A 4 08-2004 24 2 0 0 -4 -2 22 5485 025009 OHATA 332 A 4 09-2004 16 1 0 0 -1 0 16 5485 025014 OWANI 332 A 4 09-2004 -

Nord-Honshū (Tōhoku)
TM Nord-Honshū (Tōhoku) Tōhoku Vorwort Selbst Besuchern, die schon in Japan waren, ist die Region Tōhoku, die den nördlichen Teil der Hauptinsel Honshū umfasst, oft gänzlich unbekannt. Dabei findet man hier all das, was Japan so faszinierend macht, und zudem ohne Besuchermassen. Bis vor kurzem war der Norden Honshūs tatsächlich schwierig zu bereisen – die öffentlichen Verkehrsmittel waren nicht so gut ausgebaut wie im südlichen Teil von Honshū, und auch die englisch- sprachige Ausschilderung ließ noch zu wünschen übrig. Dies alles ist nun im Vorfeld der Olympischen Sommerspiele in Tokio 2020 in Angriff genommen worden. Tōhoku begeistert mit großartigen Landschaften wie den Heiligen Drei Bergen Dewa San- zan in Yamagata, der berühmten Bucht von Matsushima nahe der Stadt Sendai, oder mit der Mondlandschaft um den Vulkan Osorezan. Für kulturell Interessierte bieten die UNESCO Weltkulturerbe-Stätten von Hiraizumi einen Einblick in vergangene Feudalzei- ten. Zahlreiche Feste wie das berühmte Nebuta Matsuri in Aomori oder das Reiter-Festi- val Soma Nomaoi locken jedes Jahr zigtausende Besucher in die Region. FASZINIEREND — BUNT — JAPAN Kurz: es gibt hier Vieles zu entdecken in einer bisher wenig besuchten Region Japans. Das findet inzwischen auch Lonely Planet: für das Jahr 2020 steht Tōhoku an dritter Stelle WIR FLIEGEN SIE HIN! unter den vom Lonely Planet an Top 10 gesetzten Regionen weltweit. Mit diesem Booklet möchten wir Ihren Appetit wecken – schauen Sie selbst, was Tōhoku Ihnen alles zu bieten GOEntdecken Sie Japans viele Facetten und tauchen Sie hat! ein in unvergessliche Erlebnisse. Viel Freude beim Entdecken wünscht Ihnen das JNTO Frankfurt-Team! Erleben Sie Japan bereits bei uns an Bord — 4x täglich und nonstop mit ANA von Deutschland nach Tokio und darüber hinaus. -

Mutsu ONE Trail
Imabetsu Town Tsugaruhamana Station Imabetsu Town Tsugaruhamana Station Sotogahama Town Top Mast Aomori City WA-RASSE A full 250-km walking Mutsu ONE Trail trip around Mutsu Bay ̶8 Model Routes to Enjoy the Mutsu Bay̶ Sotogahama Town Tappizaki Sotogahama Town Top Mast Aomori City ASPAM Aomori City Asamushi Onsen Designated as Tsugaru Quasi-National Park, this area Takanozaki in Imabetsu is a stunning, scenic spot with Tamamatsu Beach in Yomogita is widely known for its You can walk through Aoiumi Park in Aomori while This leaflet introduces the eight model routes to enjoy the “Mutsu allows you to walk all the way while enjoying the sea mysterious-looking and oddly-shaped rocks jutting out everywhere. “crystal-clear water.” Between Yomogita and Aburakawa enjoying a gentle sea breeze and a view of the Mutsu Mutsu ONE Trail The one-kilometer row of black pines in Tairadate, Sotogahama, is ONE Trail.” There are a myriad of ways to enjoy it, depending on breeze nearby. You can see Hokkaido to the north, in Aomori, the road runs closely along the sea, allowing Bay. The sunset from Asamushi Beach will fascinate called “Matsumae Kaido” because the Matsumae clan used to you to walk while viewing the Shimokita Peninsula to the Suggested Travel Itineraries when and where you visit. You can start from any point according Tappizaki to the west, and the Shimokita Peninsula to travel along this road during the Edo period under the Tokugawa visitors, because it looks as if the sun is being drawn into north, Asamushi to the west on other side of the coast, the east. -

By Municipality) (As of March 31, 2020)
The fiber optic broadband service coverage rate in Japan as of March 2020 (by municipality) (As of March 31, 2020) Municipal Coverage rate of fiber optic Prefecture Municipality broadband service code for households (%) 11011 Hokkaido Chuo Ward, Sapporo City 100.00 11029 Hokkaido Kita Ward, Sapporo City 100.00 11037 Hokkaido Higashi Ward, Sapporo City 100.00 11045 Hokkaido Shiraishi Ward, Sapporo City 100.00 11053 Hokkaido Toyohira Ward, Sapporo City 100.00 11061 Hokkaido Minami Ward, Sapporo City 99.94 11070 Hokkaido Nishi Ward, Sapporo City 100.00 11088 Hokkaido Atsubetsu Ward, Sapporo City 100.00 11096 Hokkaido Teine Ward, Sapporo City 100.00 11100 Hokkaido Kiyota Ward, Sapporo City 100.00 12025 Hokkaido Hakodate City 99.62 12033 Hokkaido Otaru City 100.00 12041 Hokkaido Asahikawa City 99.96 12050 Hokkaido Muroran City 100.00 12068 Hokkaido Kushiro City 99.31 12076 Hokkaido Obihiro City 99.47 12084 Hokkaido Kitami City 98.84 12092 Hokkaido Yubari City 90.24 12106 Hokkaido Iwamizawa City 93.24 12114 Hokkaido Abashiri City 97.29 12122 Hokkaido Rumoi City 97.57 12131 Hokkaido Tomakomai City 100.00 12149 Hokkaido Wakkanai City 99.99 12157 Hokkaido Bibai City 97.86 12165 Hokkaido Ashibetsu City 91.41 12173 Hokkaido Ebetsu City 100.00 12181 Hokkaido Akabira City 97.97 12190 Hokkaido Monbetsu City 94.60 12203 Hokkaido Shibetsu City 90.22 12211 Hokkaido Nayoro City 95.76 12220 Hokkaido Mikasa City 97.08 12238 Hokkaido Nemuro City 100.00 12246 Hokkaido Chitose City 99.32 12254 Hokkaido Takikawa City 100.00 12262 Hokkaido Sunagawa City 99.13 -

Aomori Cycling
AOMORI CYCLING Up close and personal with the incredible nature and culture of Aomori Aomori Cycling Up close and personal with the incredible nature and culture of Aomori Surrounded by ocean on all sides and blessed by incredible nature such as Shirakami-Sanchi and Lake Towada, each region in Aomori Prefecture enjoys its own unique history, culture and delicacies. Cycling Aomori is the perfect way to discover the intricacies of these individual regions. If you are ready, then jump on your bike and let's head off to explore the beauty of Aomori! 9 1 Course 1 NATSUDOMARI 11 2 Course 2 TOWADA・OIRASE 13 3 Course 3 HIROSAKI 15 4 Course 4 NISHIKAIGAN 17 5 Course 5 OKU-TSUGARU AOMORI 19 6 Course 6 SHIMOKITA 21 7 Course 7 LAKE OGAWARA CYCLING 23 Course 8 HACHINOHE Up close and personal with the incredible nature and culture of Aomori 8 25 33 27 35 29 37 31 7 8 03 02 04 05 06 01/The masses of blue net stored at the port are shellfish baskets, used for cultivating scallops. It's like riding through a maze. 02/Old fishing vessels of all shapes and sizes are dotted around the Natsudomari Peninsula. 03/Showing off the size of the scallops at "Hotate Hiroba," which has a giant scallop as its signboard. You can learn about scallop cultivation on the second floor.04 /At Yogoshiyama Forest Park you can see over 3,000 varieties of succulents. 05/Two men and a cat taking a break from cycling beside the tetrapod seawall. -

50Must See Sites
21 Watch the sunset on Miss Veedol Beach. 36 See the Golden Line on Route 103 in the Hakkodas during the spring. 22 Visit the burial place of Christ. 37 See the fall colors at the Hirosaki Chrysanthemum Festival. 23 Check out Sakura Yabusame, an archery festival, in Towada. 38 Mountain bike through the trail at the Matsuminotaki Falls. 24 See the flower horse sculpture at the Towada City Art Museum. 39 Take in the beauty of the Kuji Sea Cliffs. 25 Check out Osorezan, also known as fear mountain. 40 See the Aomori-ken dog at the Aomori Art Musuem. 26 Have a picnic in the Statue of Liberty Park in Misawa. 41 Catch an ice hockey game in Hachinohe. 27 Collect sand dollars at Sand Dollar Beach. 42 Ride the Tsugaru Tetsudo Stove Train. 28 Go horseback riding in Towada. 43 Participate in a tea ceremony. 29 See the stalagmites in the Ryusendo Caves. 44 Enjoy a day at the beach at Tanesashi in Hachinohe. 30 Go fishing in the Pacific Ocean. 45 Ski or snowboard the 5 kilometer ski run at Appi Resort. must see sites 31 Go scuba diving off Cape Tappi. 46 Take a nice, easy walk along the Tsuta Nature Trail in the Hakkodas. 32 Sled down the astro turf slide in the Misawa Citizens Park. 47 Ride the go carts at Tonami Clan Memorial Tourist Village. 50 33 Shop for kimonos at a second hand store. 48 Take pictures of Miroku Falls near Takko-Machi. near 34 See the beautiful Juniko Lakes in Fukaura. -

Approved List of Japanese Fishery Fbos for Export to Vietnam Updated: 11/6/2021
Approved list of Japanese fishery FBOs for export to Vietnam Updated: 11/6/2021 Business Approval No Address Type of products Name number FROZEN CHUM SALMON DRESSED (Oncorhynchus keta) FROZEN DOLPHINFISH DRESSED (Coryphaena hippurus) FROZEN JAPANESE SARDINE ROUND (Sardinops melanostictus) FROZEN ALASKA POLLACK DRESSED (Theragra chalcogramma) 420, Misaki-cho, FROZEN ALASKA POLLACK ROUND Kaneshin Rausu-cho, (Theragra chalcogramma) 1. Tsuyama CO., VN01870001 Menashi-gun, FROZEN PACIFIC COD DRESSED LTD Hokkaido, Japan (Gadus macrocephalus) FROZEN PACIFIC COD ROUND (Gadus macrocephalus) FROZEN DOLPHIN FISH ROUND (Coryphaena hippurus) FROZEN ARABESQUE GREENLING ROUND (Pleurogrammus azonus) FROZEN PINK SALMON DRESSED (Oncorhynchus gorbuscha) - Fresh fish (excluding fish by-product) Maekawa Hokkaido Nemuro - Fresh bivalve mollusk. 2. Shouten Co., VN01860002 City Nishihamacho - Frozen fish (excluding fish by-product) Ltd 10-177 - Frozen processed bivalve mollusk Frozen Chum Salmon (round, dressed, semi- dressed,fillet,head,bone,skin) Frozen Alaska Pollack(round,dressed,semi- TAIYO 1-35-1 dressed,fillet) SANGYO CO., SHOWACHUO, Frozen Pacific Cod(round,dressed,semi- 3. LTD. VN01840003 KUSHIRO-CITY, dressed,fillet) KUSHIRO HOKKAIDO, Frozen Pacific Saury(round,dressed,semi- FACTORY JAPAN dressed) Frozen Chub Mackerel(round,fillet) Frozen Blue Mackerel(round,fillet) Frozen Salted Pollack Roe TAIYO 3-9 KOMABA- SANGYO CO., CHO, NEMURO- - Frozen fish 4. LTD. VN01860004 CITY, - Frozen processed fish NEMURO HOKKAIDO, (excluding by-product) FACTORY JAPAN -

Distribution of the Japanese Yellow Bunting Emberiza Sulphurata on Shimokita and Tsugaru Peninsulas, Aomori Prefecture 総合政策 第○巻第○号(201●) 総合政策 第○巻第○号(201●)
View metadata, citation and similar papers at core.ac.uk brought to you by CORE 短報 Distribution総合政策 第 of the Japanese 21 巻(2020)pp.109-114 yellow bunting Emberiza sulphurata on Shimokita andJournal Tsugaru of Peninsulas,Policy Studies Aomori Prefecture B5版 新様式 総合政策 第○巻第○号(201●) pp.1-20 Journal of Policy Studies Distribution of the Japanese yellow bunting Emberiza sulphurata on Shimokita and Tsugaru Peninsulas, Aomori Prefecture ✻ Yoshio Kaneko Abstract The Japanese yellow bunting Emberiza sulphurata breeds only in Japan and is distributed mainly in northern Japan. I made observations on the species on Shimokita and Tsugaru Peninsulas which are the northernmost parts of mainland Honshu. The species was frequently found in both peninsulas and occurred in areas lower than 60 m in altitude. According to the IUCN Redlist, the species breeds from 600 m to 1,500 m. Since it can be found in the areas lower than 600 m on Shimokita, Tsugaru and elsewhere, IUCN’s description needs to be rectified. Considering the occurrence in a wide range of altitudes, the population of the Japanese yellow bunting may be larger than once believed. K ey words northern Japan, altitudinal distribution, habitat, IUCN Redlist Introduction The Japanese yellow bunting Emberiza sulphurata is a small passerine bird species belonging to the family Emberizidae (Fig. 1). The species is known to breed only in Japan. It is distributed and breeds mainly in northern Japan. There is no breeding record from Hokkaido. It used to be thought to breed in limited areas such as Mt. Fuji. However, it has recently become known that the species is fairly common in northern Japan, especially in the Fig. -

Tsugaru Port Tourist Information
Tsugaru Port Tourist Information http://www.mlit.go.jp/kankocho/cruise/ Lake Juniko (Aoike Pond) Lake Juniko is the collective name for the 33 lakes and ponds found around the UNESCO World Heritage Site Shirakami Sanchi. Among these Aoike Pond is a mysterious blue color, as if someone has poured blue ink into it, and the decayed large beech trees in the water reach across the pond. The pond's appearance changes depending the sun and the angle from which you look at it. Matsukami, Fukaura-machi, Nishitsugaru-gun, Aomori Location/View 038-2206 Access Roughly a 90 minute drive from the port (65km) Season April – November Awone Shirakami Juniko http://www.shirakami-jyuniko.jp/ Related links Fukaura Town http://www.town.fukaura.lg.jp/index.html Contact Us: Fukaura Town, Tourism Division TEL: 0173-74-4412 Tsuru no Mai Bridge Tsuru no Mai Bridge was built in 1994 and at over 300 meters in length it is the longest wooden triple-arched bridge in Japan. Its reflection on Tsugaru Fujimi Lake is refined and beautiful, and there is great view of Mt. Iwaki in the distance. 81-150 Mawarizeki-osawa, Tsuruta-machi, Kitatsugaru- Location/View gun, Aomori 038-3542 Access Roughly a 25 minute drive from the port (15km) Season Year-round Tsuruta Town's Tourism Web Magazine "Medetai Tsuruta": Related links https://www.medetai- tsuruta.jp/spot/sightseeing/tsurunomaibridge.html Contact Us: Tsuruta Town, Tourism Planning Division TEL: 0173-22-2111 Tachineputa no Yakata Goshogawara Tachineputa Festival is held annually in Goshogawara from August 4th to August 8th, and the large floats from the festival are on display here.