Application 10/6/2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Cta ΠCumenica
2020 N. 2 ACTA 2020 ŒCUMENICA INFORMATION SERVICE OF THE PONTIFICAL COUNCIL FOR PROMOTING CHRISTIAN UNITY e origin of the Pontical Council for Promoting Christian Unity is closely linked with the Second Vatican Council. On 5 June 1960, Saint Pope John XXIII established a ‘Secretariat for Promoting Christian Unity’ as one of the preparatory commissions for the Council. In 1966, Saint Pope Paul VI conrmed the Secretariat as a permanent dicastery CUMENICA of the Holy See. In 1974, a Commission for Religious Relations with the Jews was established within the Secretariat. In 1988, Saint Pope John Paul II changed the Secretariats status to Pontical Council. Œ e Pontical Council is entrusted with promoting an authentic ecumenical spirit in the Catholic Church based on the principles of Unitatis redintegratio and the guidelines of its Ecumenical Directory rst published in 1967, and later reissued in 1993. e Pontical Council also promotes Christian unity by strengthening relationships CTA with other Churches and Ecclesial Communities, particularly through A theological dialogue. e Pontical Council appoints Catholic observers to various ecumenical gatherings and in turn invites observers or ‘fraternal delegates’ of other Churches or Ecclesial Communities to major events of the Catholic Church. Front cover Detail of the icon of the two holy Apostles and brothers Peter and Andrew, symbolizing the Churches of the East and of the West and the “brotherhood rediscovered” (UUS 51) N. 2 among Christians on their way towards unity. (Original at the Pontical -

Scanned Using Book Scancenter 5022
The RUTGERS ART REVIEW Published Annually by the Students of the Graduate Program in Art History at Rutgers university Spring 1984 Volume V II Corporate Matching Funds Martin Eidclberg Carrier Corporation Foundation. Inc. Mrs. Helmut von Erffa Citicorp Dino Philip Galiano Seth A. Gopin Lifetime Benefactor Daria K. Gorman Henfield Foundation Mary C. Gray Nathaniel Gurien Benefactors Marion Husid In memory of Mary Bartlett Linda R. Idetberger Cowdrey Nancy M. KatzolT John and Katherine Kenfield Patrons Mr. and Mrs. Sanford Kirschenbaum In memory of Frank S. Allmuth, Julia M. Lappegaard Class of 1920 Cynthia and David Lawrence Mr. and Mrs. John L. Ayer Patricia I..eightcn Olga and Oev Berendsen Deborah Leuchovius Robert P. and Marcelle Bergman Marion and Allan Maiilin Dianne M. Green Ricky A. Malkin Frima and Larry Hofrichter Tod A. Marder Robert S. Peckar Joan Marter Paul S. Sheikewiiz, M.D. Thomas Mohle Jeffrey Wechsler Roberto A. Moya Scott E. Pringle Supporters Eliot Rowlands Carol and Jerry Alterman Anita Sagarese Randi Joan Alterman John M. Schwebke Richard Derr John Beldon Scott Archer St. Clair Harvey Mr. and Mrs. Eugene Seitz William E. Havemeyer Marie A. Somma Dr. Robert Kaita and Ms. Chiu-Tze Jack and Helga Spector Lin James H. Stubblebine Mr. and Mrs. Edward J. Linky Richard and Miriam Wallman Mr. and Mrs. James McLachlan Harvey and Judith Waterman Barbara and Howard Mitnick Michael F. Weber Elizabeth M. Thompson Sarah B. Wilk Lorraine Zito*Durand Friends Department of Art History, University of Ann Conover, Inc. Delaware Keith Asszony The Pennsylvania State University, Renee and Matthew Baigell Department of Art History William and Elizabeth Bauer The Graduate School-New Brunswick, Naomi Boretz Rutgers University Phillip Dennis Cate Jane Voorhees Zimmerli Art Museum Zeau C. -

Archdiocese of Los Angeles
Clerical Sexual Abuse in the Archdiocese of Los Angeles AndersonAdvocates.com • 310.357.2425 Attorney Advertising “For many of us, those earlier stories happened someplace else, someplace away. Now we know the truth: it happened everywhere.” ~ Pennsylvania Grand Jury Report 2018 AndersonAdvocates.com • 310.357.2425 2 Attorney Advertising Table of Contents Purpose & Background ...........................................................................................9 History of the Archdiocese of Los Angeles ...........................................................12 Los Angeles Priests Fleeing the Jurisdiction: The Geographic Solution ....................................................................................13 “The Playbook for Concealing the Truth” ..........................................................13 Map ........................................................................................................................16 Archdiocese of Los Angeles Documents ...............................................................17 Those Accused of Sexual Misconduct in the Archdiocese of Los Angeles ..... 38-125 AndersonAdvocates.com • 310.357.2425 3 Attorney Advertising Clerics, Religious Employees, and Volunteers Accused of Sexual Misconduct in the Archdiocese of Los Angeles Abaya, Ruben V. ...........................................39 Casey, John Joseph .......................................49 Abercrombie, Leonard A. ............................39 Castro, Willebaldo ........................................49 Aguilar-Rivera, -
X X X X X X X X X X X X X X X X X
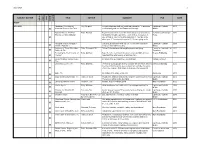
2/25/2020 1 SUBJECT MATTER TITLE AUTHOR SUMMARY PUB DATE DVD gdom VIDEO AUDIO OTHER OTHER AUDIO 2/12/2020 Abraham: Revealing the Ray, Stephen To understand our faith, we must understand the "Jewishness" Lighthouse Catholic 2011 x Historical Roots of our Faith of Christianity and our Old Testament Heritage Media Adam's Return: The Five Rohr, Richard Boys become men in much the same way across cultures, by St. Anthony Messenger 2006 Promises of Male Initiation integrating, through experience, each of these messages: 1. Press x Life is hard; 2. You are not that important; 3. Your life is not about you; 4. You are not in control; 5. You are going to die. Amazing Angels and Super Cat.Chat, designed for kids ages 3-11, to teach lessons for Lighthouse Catholic 2008 x Saints - Episode 1 living out their faith every day Media Authority of Those Who Have Rohr, Richard OFM Father Richard shares his insights on pain and dying Center for Loss and Life 2005 x Suffered, The Transition Becoming the Best Version of Kelly, Matthew Take life to the next level: who you become is infinitely more Beacon Publishing 1999 x Yourself important than what you do or what you have. Best of Catholic Answers Live, 47 answers to questions from non-Catholics Catholic Answers x The Best Way to Live, The Kelly, Matthew Perfect for young paople as they consider the life before them at Beacon Publishing 2012 the time of Confirmation; also an important reminder for adults x of any age, and one that is sure to help you refocus your life x Bible, The Recitation of the Bible on 64 cd's Zondervan 2001 Body and Blood of Christ, The Hahn, Dr. -

Summary of Sexual Abuse Claims in Chapter 11 Cases of Boy Scouts of America
Summary of Sexual Abuse Claims in Chapter 11 Cases of Boy Scouts of America There are approximately 101,135sexual abuse claims filed. Of those claims, the Tort Claimants’ Committee estimates that there are approximately 83,807 unique claims if the amended and superseded and multiple claims filed on account of the same survivor are removed. The summary of sexual abuse claims below uses the set of 83,807 of claim for purposes of claims summary below.1 The Tort Claimants’ Committee has broken down the sexual abuse claims in various categories for the purpose of disclosing where and when the sexual abuse claims arose and the identity of certain of the parties that are implicated in the alleged sexual abuse. Attached hereto as Exhibit 1 is a chart that shows the sexual abuse claims broken down by the year in which they first arose. Please note that there approximately 10,500 claims did not provide a date for when the sexual abuse occurred. As a result, those claims have not been assigned a year in which the abuse first arose. Attached hereto as Exhibit 2 is a chart that shows the claims broken down by the state or jurisdiction in which they arose. Please note there are approximately 7,186 claims that did not provide a location of abuse. Those claims are reflected by YY or ZZ in the codes used to identify the applicable state or jurisdiction. Those claims have not been assigned a state or other jurisdiction. Attached hereto as Exhibit 3 is a chart that shows the claims broken down by the Local Council implicated in the sexual abuse. -

Download Download
Journal of Arts & Humanities Volume 08, Issue 09, 2019: 16-30 Article Received: 02-08-2019 Accepted: 04-09-2019 Available Online: 06-09-2019 ISSN: 2167-9045 (Print), 2167-9053 (Online) DOI: http://dx.doi.org/10.18533/journal.v8i9.1714 Gospel Evangelist Portraits: Exemplars of an Enduring Christian Motif James W. Ellis1 ABSTRACT The Bible’s Gospel books offer accounts of the life of Jesus Christ and consequently they have been considered among the most important texts from antiquity onward. This essay uses iconographic methodology and historical contextualization to analyze a selective group of portraits and depictions of the Bible’s four Gospel Evangelists: Matthew, Mark, Luke, and John. Art historical literature has addressed Evangelist portraits, but has tended to focus on formal characteristics. This essay presents these visual relics in new contexts. The chosen Evangelist portraits come from a variety of sources: thousand-year-old Byzantine lectionaries, medieval illuminated manuscripts produced in the scriptoria of the Abbeys of Cluney and Helmarshausen, and Italian and French missals and books of hours. The essay also examines Northern Renaissance and Symbolist print cycles portraying the martyrdom of the Evangelist John and visions he described in his Apocalypse, or book of Revelation. This brief examination of select exemplars demonstrates the enduring significance of Evangelist portraits in Christian iconography and western art history, and suggests the variety of messages Evangelist portraits can convey. This essay’s findings and conclusions may lead to further, related research concerning the ways theologians and artists have used biblical portraits to comment both on religious and secular issues. -

Artists at Work Artists at Work
Artists at Work Artists at Work Deanna Petherbridge and Anita Viola Sganzerla edited by Ketty Gottardo and Rachel Sloan Contents First published to accompany Artists at Work The Courtauld Gallery, London, 3 May – 15 July 2018 The Courtauld Gallery is supported by the 7 Higher Education Funding Council for England (hefce) Foreword The programme of the Gilbert and Ildiko Butler Drawings Gallery is generously supported by The International Music and Art Foundation 9 Preface 11 Playful Images of Allegory and Actuality Copyright © 2018 Texts copyright © 2018 the authors deanna petherbridge All rights reserved. No part of this publication may be transmitted in any form or by any means, electronic or mechanical, including photocopy, recording or any storage or retrieval system, without the prior permission in writing from the copyright holder and publisher. 32 isbn 978-1-911300-44-1 British Library Cataloguing in Publication Data Catalogue A catalogue record for this book is available from the British Library anita viola sganzerla Produced by Paul Holberton Publishing 89 Borough High Street, London se1 1nl www.paulholberton.com 83 Designed by Laura Parker Bibliography and Photographic Credits Printing by Gomer Press, Llandysul front cover: Cat. 19 (detail) back cover: Cat. 7 (detail) frontispiece: Cat. 3 (detail, larger than actual size) Foreword Following A Civic Utopia, organised in 2016 with Drawing I wish to extend my warm thanks to Anita Viola Matter Trust, Artists at Work is the second exhibition in the Sganzerla, curator of the Katrin Bellinger collection, Gilbert and Ildiko Butler Drawings Gallery to present works who wrote the catalogue entries for this publication and chiefly from a single collection, other than The Courtauld’s contributed to many other aspects of the exhibition. -

El Greco's Saint Francisat the Bilbao Fine Arts Museum
El Greco’s Saint Francis at the Bilbao Fine Arts Museum Ana Sánchez-Lassa de los Santos José Luis Merino Gorospe This text is published under an international Attribution-NonCommercial-NoDerivs Creative Commons licence (BY-NC-ND), version 4.0. It may therefore be circulated, copied and reproduced (with no alteration to the contents), but for educational and research purposes only and always citing its author and provenance. It may not be used commercially. View the terms and conditions of this licence at http://creativecommons.org/licenses/by-ncnd/4.0/legalcode Using and copying images are prohibited unless expressly authorised by the owners of the photographs and/or copyright of the works. © of the texts: Bilboko Arte Ederren Museoa Fundazioa-Fundación Museo de Bellas Artes de Bilbao Photography credits © Archivo del Instituto Valencia de Don Juan, Madrid: fig. 2 © Bilboko Arte Ederren Museoa Fundazioa-Fundación Museo de Bellas Artes de Bilbao: figs. 1, 3, 4 and 10-25 © Fine Arts Museum of San Francisco. Donated by Samuel H. Kress Foundation: fig. 5 © Meadows Museum, Southern Methodist University, Dallas. Museum Purchase. Meadows Acquisition Fund with private donations and University funds: fig. 8 © Museo Diocesano de Arte Sacro, Vitoria-Gasteiz. Depósito de la Diputación Foral de Álava: fig. 9 © RMN-Grand Palais / Jacques Quecq d’Henripret: fig. 7 © The Art Institute of Chicago: fig. 6 Text published in: Buletina = Boletín = Bulletin. Bilbao : Bilboko Arte Eder Museoa = Museo de Bellas Artes de Bilbao = Bilbao Fine Arts Museum, no. 8, 2014, pp. 111-157. Sponsor: aint Francis in Prayer Before the Crucifix, by El Greco [fig. -

Chapman CV 2020
H. PERRY CHAPMAN Department of Art History tel (302) 831-2243 University of Delaware dept (302) 831-8415 318 Old College [email protected] Newark, DE 19716 EDUCATION Princeton University, M.F.A., 1978; Ph.D., 1983. Dissertation: “The Image of the Artist: Roles and Guises in Rembrandt's Self-Portraits.” (advisers: John Rupert Martin and Egbert Haverkamp- Begemann) Swarthmore College, B.A., High Honors, Phi Beta Kappa, 1975. APPOINTMENTS University of Delaware, Department of Art History, Instructor, 1982-83; Assistant Professor, 1983-89; Associate Professor, 1989-97; Professor, 1997-; Interim Chair, 2014-15. Institute of Fine Arts, New York University, Lecturer, Spring 2010. The Art Bulletin, Editor Designate, 1999-2000; Editor-in-Chief, 2000-2004. The American University, Department of Art History, Professorial Lecturer, Spring 1982. Swarthmore College, Art Department, Instructor, Spring 1981. CURATORIAL EXPERIENCE Denver Art Museum and The Newark Museum, Consultant for exhibition Art & Home: Dutch Interiors in the Age of Rembrandt, held in 2001-2002. The National Gallery of Art, Washington, DC, Guest Co-Curator for exhibition Jan Steen: Painter and Storyteller, held at the National Gallery and the Rijksmuseum, Amsterdam, in 1996-1997. FELLOWSHIPS, GRANTS AND AWARDS University of Delaware, Institute for Global Studies, International Travel Award, 2014. Summer Teachers Institute in Technical Art History (STITAH) 2012, Yale University, July 2012 (funded by the Samuel H. Kress Foundation), participant. University of Delaware, General University Research Grant, 2012. John Simon Guggenheim Foundation Fellow, 2004 (held in 2006). Center for Advanced Study in the Visual Arts, Samuel H. Kress Senior Fellow, 2004-2005. National Endowment for the Humanities, Fellowship for University Teachers, 1993-1994. -

TASTE and PRUDENCE in the ART of JUSEPE DE RIBERA by Hannah Joy Friedman a Dissertation Submitted to the Johns Hopkins Universit
TASTE AND PRUDENCE IN THE ART OF JUSEPE DE RIBERA by Hannah Joy Friedman A dissertation submitted to the Johns Hopkins University in conformity with the requirements for the degree of Doctor of Philosophy Baltimore, Maryland May, 2016 Copyright Hannah Joy Friedman, 2016 (c) Abstract: Throughout his long career in southern Italy, the Spanish artist Jusepe de Ribera (1591- 1652) showed a vested interest in the shifting practices and expectations that went into looking at pictures. As I argue, the artist’s evident preoccupation with sensory experience is inseparable from his attention to the ways in which people evaluated and spoke about art. Ribera’s depictions of sensory experience, in works such as the circa 1615 Five Senses, the circa 1622 Studies of Features, and the 1637 Isaac Blessing Jacob, approach the subject of the bodily senses in terms of evaluation and questioning, emphasizing the link between sensory experience and prudence. Ribera worked at a time and place when practices of connoisseurship were not, as they are today, a narrow set of preoccupations with attribution and chronology but a wide range of qualitative evaluations, and early sources describe him as a tasteful participant in a spoken connoisseurial culture. In these texts, the usage of the term “taste,” gusto, links the assessment of Ribera’s work to his own capacity to judge the works of other artists. Both taste and prudence were crucial social skills within the courtly culture that composed the upper tier of Ribera’s audience, and his pictures respond to the tensions surrounding sincerity of expression or acceptance of sensory experience in a novel and often satirical vein. -

Unclaimed Property for County: CLEVELAND 7/16/2019
Unclaimed Property for County: CLEVELAND 7/16/2019 OWNER NAME ADDRESS CITY ZIP PROP ID ORIGINAL HOLDER ADDRESS CITY ST ZIP 18 NORTH CONVENIENCE & CAFE 5245 FALLSTON RD LAWNDALE 28090-9128 15697848 PEPSI BOTTLING GROUP 1111 WESTCHESTER AVE ATTN: ROSEMARY WHITE PLAINS NY 10604 SHAY 2-013.F BLDG 1129 A R I PO BOX 3137 SHELBY 28151 15153951 STATE EMPLOYEES CREDIT UNION 1000 WADE AVE RALEIGH NC 27605 AAA MINI STORAGE 1157 2 EAST MARION STREET SHELBY 28150 15873583 ALTEC INC 210 INVERNESS CENTER DR BIRMINGHAM AL 35242 AARON RUSSEL SCHEFFEL 3655 GRIGG RD SHELBY 28150-7732 15211572 NAVIENT CORPORATION ATTN UNCLAIMED PROPERTY V1075 2001 RESTON VA 20191 EDMUND HALLEY DR ABDOW DOLORES A 214 WALL AVE SHELBY 28152-7711 15984804 DIRECTV LLC 1 AT&T WAY RM 2B228A BEDMINSTER NJ 07921 ABDUSSAMAD JUNAID 200 SPRUCE ST APT 1F KINGS MTN 28086-3674 14955370 NC DEPT OF REVENUE P O BOX 25000 IMPREST CASH FUND RALEIGH NC 27640 ABERNATHY JAMES 134 EZRA RD KINGSMTN 28086-9998 15905594 UNION SECURITY INS CO 260 INTERSTATE NORTH CIR SE ATLANTA GA 30339 ABERNATHY JAMES 134 EZRA RD KINGSMTN 28086-9998 15905591 UNION SECURITY INS CO 260 INTERSTATE NORTH CIR SE ATLANTA GA 30339 ABERNETHY HAVEN SKYLOR 5015 BOWEN DR SHELBY 28152 15361771 CLEVELAND COUNTY BOARD OF EDUCATION400 W MARION ST SHELBY NC 28150 ABSHER MARY 1652 CHERRYVILLE RD WACO 28169 14879325 PAYPAL INC 12312 PORT GRACE BLVD ATTN: LA VISTA NE 68128 UNCLAIMED PROPERTY ACA INCORPORATED 447 S LAFAYETTE ST SHELBY 28150 15284513 CLEVELAND COUNTY CSC C/O CLERK OF COURT 100 JUSTICE PLACE SHELBY NC 28150 ACCOR BARBARA -

Higher Education Allocation
HEERF II Allocations for Public and Nonprofit Institutions under CRRSAA section 314(a)(1) 1/13/2021 CARES Act Minimum Amount Section 314(a)(1)(E) Minimum Amount Maximum Amount for Emergency & Section for Student Aid for Institutional Financial Aid Grants 314(a)(1)(F) Portion (CFDA Portion (CFDA OPEID Institution Name School Type State Total Award to Students Allocation 84.425E Allocation) 84.425F Allocation) 00100200 Alabama Agricultural & Mechanical University Public AL $ 14,519,790 $ 4,560,601 $ 37,515 $ 4,560,601 $ 9,959,189 00100300 Faulkner University Private Non‐Profit AL $ 4,333,744 $ 1,211,489 $ 239,004 $ 1,211,489 $ 3,122,255 00100400 University of Montevallo Public AL $ 4,041,651 $ 1,280,001 $ ‐ $ 1,280,001 $ 2,761,650 00100500 Alabama State University Public AL $ 10,072,950 $ 3,142,232 $ 174,255 $ 3,142,232 $ 6,930,718 00100700 Central Alabama Community College Public AL $ 2,380,348 $ 611,026 $ 32,512 $ 611,026 $ 1,769,322 00100800 Athens State University Public AL $ 2,140,301 $ 422,517 $ 492,066 $ 492,066 $ 1,648,235 00100900 Auburn University Public AL $ 23,036,339 $ 7,822,873 $ 31,264 $ 7,822,873 $ 15,213,466 00101200 Birmingham‐Southern College Private Non‐Profit AL $ 1,533,280 $ 534,928 $ ‐ $ 534,928 $ 998,352 00101300 Calhoun Community College Public AL $ 10,001,547 $ 2,196,124 $ 332,365 $ 2,196,124 $ 7,805,423 00101500 Enterprise State Community College Public AL $ 2,555,815 $ 620,369 $ 45,449 $ 620,369 $ 1,935,446 00101600 University of North Alabama Public AL $ 8,666,299 $ 2,501,324 $ 137,379 $ 2,501,324 $ 6,164,975 00101700 Gadsden State Community College Public AL $ 7,581,323 $ 1,878,083 $ 219,704 $ 1,878,083 $ 5,703,240 00101800 George C.