Aandp1ch10lecture.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Intrinsic Hand Muscles of the Japanese Monkey, Macaca Fuscata
Anthropol.Sci. 102(Suppl.), 85-95,1994 Intrinsic Hand Muscles of the Japanese Monkey, Macaca fuscata TOSHIHIKO HOMMA AND TATSUO SAKAI Department of Anatomy, School of Medicine, Juntendo University, Hongo 2-1-1, Bunkyo-ku, Tokyo 113, Japan Received December 24, 1993 •ôGH•ô Abstract•ôGS•ô Anatomy of the intrinsic hand muscles in the Japanese monkeys was studied with an improved method to dissect the muscles and nerves in water after removal of the skeletal framework. The thenar eminence contained four muscles, namely m. abductor pollicis brevis, m. opponens pollicis, m, flexor pollicis brevis, and m. adductor pollicis. The hypothenar eminence contained four muscles, namely m. palmaris brevis, m. abductor digiti minimi, m. flexor digiti minimi brevis, and m. opponens digiti minimi. Majority of the thenar muscles are fused more or less with each other, so that clear separation of these muscles was difficult. The lumbrical muscles arose from the palmar parts of four main tendons of the deep flexor muscle to the second, third, fourth, and fifth digits. The mm, contrahentes arose mainly from a medial tendinous septum attached on the palmar surface to the third metacarpus, and included three muscles destined to the second, fourth and fifth digits. The interossei were found on the radial side of the second, third, fourth and fifth finger as well as on the ulnar side of the second, third and fourth finger. The intrinsic hand muscles in the Japanese monkey received innervation either from the median or the ulnar nerve. Branching pattern of these nerves to the individual muscles was fundamentally similar to those in man except for the fact that the median and the ulnar nerve in the Japanese monkey do not communi cateto make a loop in the thenar muscles. -

Musculoskeletal Ultrasound Technical Guidelines II. Elbow
European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound Technical Guidelines II. Elbow Ian Beggs, UK Stefano Bianchi, Switzerland Angel Bueno, Spain Michel Cohen, France Michel Court-Payen, Denmark Andrew Grainger, UK Franz Kainberger, Austria Andrea Klauser, Austria Carlo Martinoli, Italy Eugene McNally, UK Philip J. O’Connor, UK Philippe Peetrons, Belgium Monique Reijnierse, The Netherlands Philipp Remplik, Germany Enzo Silvestri, Italy Elbow Note The systematic scanning technique described below is only theoretical, considering the fact that the examination of the elbow is, for the most, focused to one quadrant only of the joint based on clinical findings. 1 ANTERIOR ELBOW For examination of the anterior elbow, the patient is seated facing the examiner with the elbow in an extension position over the table. The patient is asked to extend the elbow and supinate the fore- arm. A slight bending of the patient’s body toward the examined side makes full supination and as- sessment of the anterior compartment easier. Full elbow extension can be obtained by placing a pillow under the joint. Transverse US images are first obtained by sweeping the probe from approximately 5cm above to 5cm below the trochlea-ulna joint, a Pr perpendicular to the humeral shaft. Cranial US images of the supracondylar region reveal the superficial biceps and the deep brachialis mu- Br scles. Alongside and medial to these muscles, follow the brachial artery and the median nerve: * the nerve lies medially to the artery. * Legend: a, brachial artery; arrow, median nerve; arrowheads, distal biceps tendon; asterisks, articular cartilage of the Humerus humeral trochlea; Br, brachialis muscle; Pr, pronator muscle 2 distal biceps tendon: technique The distal biceps tendon is examined while keeping the patient’s forearm in maximal supination to bring the tendon insertion on the radial tuberosity into view. -

Structure of the Flexor Digitorum Superficialis
Okajimas Folia Anat. Jpn., 56(5) : 277-288, December 1979 Structure of the Flexor Digitorum Superficialis By OSAMU OHTANI Department of Anatomy, Okayama University Medical School, Okayama 700, Japan (Director : Prof. Dr. H. Outi) —Received for Publication, March 9, 1979— Key Words: Flexor digitorum superficialis, Striated muscle, Forearm musculature. Summary. Fifty-two forearms of 26 Japanese adult cadavers were examined. The flexor digitorum superficialis can be separated into two layers: a superficial layer and a deep layer. The superficial layer is composed of the radial head and the superficial part of the humeroulnar head. It forms two muscle bellies which give rise to the tendons for the third and fourth digits, respectively. The deep layer is composed of the deep part of the humeroulnar head. After forming an inter- mediate tendon, the deep layer also divides into two fleshy bellies which give rise to the tendons for the second and fifth digits, respectively. Based on the mode of occurrence of the communicating muscle fasciculi between the superficial layer and the deep layer, the flexor digitorum superficialis can be classified into four types. Type I muscle has no communicating fasciculus (4/52, 7.7%). Type II muscle has a communicating muscle fasciculus between the intermediate tendon and the muscle belly for the fourth digit (muscle fasciculus A) (29/52, 55.8%). Type III muscle has the muscle fasciculus A as well as another communicating muscle fasciculus between the intermediate tendon and the belly for the third digit (muscle fasciculus B) (18/52, 34.6%). Type IV muscle has the muscle fasciculus B only (1/52, 1.9%). -

Disclosures Flexor Pronator Strain
11/19/2018 Flexor Pronator Strain, Epicondylitis, Avulsions Lee Kaplan, MD Director, UHealth Sports Medicine Institute Professor, Department of Orthopaedics, Kinesiology & Sports Science, Biomedical Engineering Medical Director and Head Team Physician, University of Miami Athletics Medical Director and Head Team Physician, Miami Marlins Josue Acevedo, MD Orthopaedics Sports Medicine fellow Disclosures • I have no conflicts of interest in relation to this presentation 2 Flexor Pronator Strain • Anatomy • Function • Forces • Clinical Presentation • Imaging Studies • Treatment 3 1 11/19/2018 Anatomy • Common Flexor Tendon origin - Medial Epicondyle Pronator Teres FCR Palmaris Longus FDS FCU 4 Function • Provides dynamic support to valgus stress during throwing motion • Contraction during early arm acceleration resists valgus and flexes wrist during ball release 5 Elbow Forces • Elbow valgus torque peaks at late cocking phase - during maximal shoulder external rotation (MER) • Can approach torque up to 120 N.m • Significantly higher torque in pitchers who enduring an injury Sawbick et al. JSES, 2004 Adam WA. AJSM, 2010. 6 2 11/19/2018 • Fastballs caused the greatest torque • Curveballs produced the greatest arm speed . • Predictors of increased elbow torque • Increased ball velocity • Higher BMI • Decreased arm slot • Protectors against elbow torque. • Increasing age • longer arm length • greater elbow circumference were independent 7 • VAS fatigue scores increased 0.72 points per inning • Medial elbow torque increased beyond inning 3, increase of 0.84 N·m each inning. • Pitch velocity decreased (0.28 mph per inning) • There were no differences in arm rotation or arm speed as the game progressed. • Arm slot decreased with each successive inning (0.73° on average per inning) ***These findings signify a possible relationship between fatigue and injury risk. -

Nerve Transfer Techniques in Injuries from the Upper Limb
THIEME Update Article | Artículo de Actualización 57 Nerve Transfer Techniques in Injuries from the Upper Limb Técnicas de transferencia nerviosa en lesiones del miembro superior Francisco Martínez Martínez1 B. Ñíguez Sevilla2 J. García García2 A. García López3 1 FEA (field medcial expert), Orthopaedics and Traumatology Surgery, Address for correspondence Francisco Martínez Martínez, C/ Canovas Hospital Clínico Universitario Virgen de la Arrixaca. Murcia, Spain del Castillo n°7- 4°a. 30003-Murcia, Spain 2 Resident, Orthopaedics and Traumatology Surgery, Hospital Clínico (e-mail: [email protected]). Universitario Virgen de la Arrixaca, Murcia, Spain 3 FEA (field medcial expert), Orthopaedics and Traumatology Surgery, Hospital General de Alicante, Alicante, Spain Rev Iberam Cir Mano 2017;45:57–67. Abstract Proximal nerve injuries from the upper limb or the braquial plexus are associated with a poor prognosis, even with prompt repair. In the last few decades an increase in nerve transfer techniques has occurred, by which a denervated peripheral nerve is reinner- vated by a healthy donor nerve. Nerve transfers are indicated in proximal brachial plexus injuries where grafting is not possible or in proximal injuries of peripheral nerves with long reinnervation distances. Nerve transfers represent a revolution in peripheral nerve surgery and offer the potential for superior functional recovery in severe nerve injuries. In complete brachial plexus injuries, there are being studied the existence of nerve roots (intraplexual transfers). If they do not exist, the transference of nerves out of the plexus are used Keywords (extraplexual transfers) as the spinal accessory nerve, the phrenic nerve, the intercostal ► nerve transfers nerves, etc. ► brachial plexus In this update paper, the different motor intra and extraplexual nerve transfer ► nerve injury techniques are going to be reviewed. -
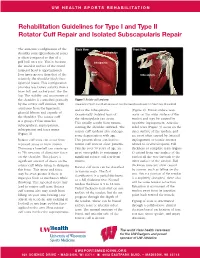
Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair The anatomic configuration of the Back View Front View shoulder joint (glenohumeral joint) Supraspinatus is often compared to that of a golf ball on a tee. This is because Infraspinatus the articular surface of the round humeral head is approximately Teres four times greater than that of the Minor Subscapularis relatively flat shoulder blade face (glenoid fossa). This configuration provides less boney stability than a truer ball and socket joint, like the hip. The stability and movement of the shoulder is controlled primarily Figure 1 Rotator cuff anatomy by the rotator cuff muscles, with Image property of Primal Pictures, Ltd., primalpictures.com. Use of this image without authorization from Primal Pictures, Ltd. is prohibited. assistance from the ligaments, and/or the infraspinatus. (Figure 2). Bursal surface tears glenoid labrum and capsule of Occasionally isolated tears of occur on the outer surface of the the shoulder. The rotator cuff the subscapularis can occur. tendon and may be caused by is a group of four muscles: This usually results from trauma repetitive impingement. Articular subscapularis, supraspinatus, rotating the shoulder outward. The sided tears (Figure 3) occur on the infraspinatus and teres minor rotator cuff tendons also undergo inner surface of the tendon, and (Figure 1). some degeneration with age. are most often caused by internal Rotator cuff tears can occur from This process alone can lead to impingement or tensile stresses repeated stress or from trauma. rotator cuff tears in older patients. related to overhead sports. -

The Muscles That Act on the Upper Limb Fall Into Four Groups
MUSCLES OF THE APPENDICULAR SKELETON UPPER LIMB The muscles that act on the upper limb fall into four groups: those that stabilize the pectoral girdle, those that move the arm, those that move the forearm, and those that move the wrist, hand, and fingers. Muscles Stabilizing Pectoral Girdle (Marieb / Hoehn – Chapter 10; Pgs. 346 – 349; Figure 1) MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: ANTERIOR THORAX: anterior surface coracoid process protracts & depresses Pectoralis minor* pectoral nerves of ribs 3 – 5 of scapula scapula medial border rotates scapula Serratus anterior* ribs 1 – 8 long thoracic nerve of scapula laterally inferior surface stabilizes / depresses Subclavius* rib 1 --------------- of clavicle pectoral girdle POSTERIOR THORAX: occipital bone / acromion / spine of stabilizes / elevates / accessory nerve Trapezius* spinous processes scapula; lateral third retracts / rotates (cranial nerve XI) of C7 – T12 of clavicle scapula transverse processes upper medial border elevates / adducts Levator scapulae* dorsal scapular nerve of C1 – C4 of scapula scapula Rhomboids* spinous processes medial border adducts / rotates dorsal scapular nerve (major / minor) of C7 – T5 of scapula scapula * Need to be familiar with on both ADAM and the human cadaver Figure 1: Muscles stabilizing pectoral girdle, posterior and anterior views 2 BI 334 – Advanced Human Anatomy and Physiology Western Oregon University Muscles Moving Arm (Marieb / Hoehn – Chapter 10; Pgs. 350 – 352; Figure 2) MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: intertubercular -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz. -

Ulnar Nerve Passing Through Triceps Muscle –Rare Variation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861. Volume 12, Issue 6 (Nov.- Dec. 2013), PP 61-62 www.iosrjournals.org Ulnar Nerve Passing Through Triceps Muscle –Rare Variation Chandrika G Teli1, Nilesh N. Kate2, H. S. Kadlimatti 3 1(Department of Anatomy, ESIC Medical College Gulbarga/ Rajiv Gandhi university of health sciences Karnataka, India) 2(Department of Physiology, ESIC Medical College Gulbarga / Rajiv Gandhi university of health sciences Karnataka, India) 3(Department of Anatomy, ESIC Medical College Gulbarga / Rajiv Gandhi university of health sciences Karnataka, India) Abstract : During routine dissection for undergraduate students, right upper limb of 45 year old male showed variation in the course of ulnar nerve. The ulnar nerve arose as a continuation of medial cord, descended down along medial side of axillary and brachial artery. As the nerve travelled upper third of arm, it pierced the medial head belly of triceps muscle, passing through it for 4-5 cm ,emerged out of it to reach near the medial epicondyle. Then the nerve passed behind the medial epicondyle to follow its normal course and distribution. This kind of variation is not been described in the literature. Keywords: lunar nerve, variation in course, entrapment neuropathy. I. Introduction The ulnar nerve (C7, 8, T1) is formed from medial cord of the brachial plexus. It lies medial to axillary and brachial artery as far as middle of humerus, and then pierces the medial inter muscular septum to descend on the anterior face of triceps. It passes behind the medial epicondyle to enter the forearm. -

This Sumarry Is Only for the Muscles of the Hand (Slides: 14-33) Please Refer to the First 13 Slide When Studying
This sumarry is only for the muscles of the hand (slides: 14-33) please refer to the first 13 slide when studying. For The innervation of these muscles its easier to memorize them from the last paragraph in the last page Muscle Origin Insertion Nerve Action Image 1st and 2nd, Flexmetacarpoph (lateral two) alangeal (MP) Extensor Tendons of flexor median nerve; joints & extend Lumbricals expansion of Digitorum 3rd and 4th interphalangeal (4 muscles) medial four profundus medial deep (IP) joints of fingers branch of ulnar fingers except nerve thumb -First arises from Proximal base of 1st phalanges of metacarpal thumb and index, Palmar adduct fingers - remaining three ring, and little Deep branch of Interossei toward center of from anterior fingers and ulnar nerve (4 muscles) third finger surface of shafts dorsal extensor of 2nd, 4th, and expansion of 5th metacarpals each finger . Proximal phalanges of index, middle, and ring fingers Contiguous sides abduct fingers Dorsal Interossei and dorsal Deep branch of of shafts of from center of (4 muscles) extensor ulnar nerve metacarpal bones third finger expansion (1st:index\ 2nd,3rd:middle \ 4th:ring) Both palmar and dorsal: -Flex metacarpophalangeal joints -Extend interphalangeal joints Simultaneous flexion at the metacarpophalangeal joints and extension at the interphalangeal joints of a digit are essential for the fine movements of writing, drawing, threading a needle, etc. The Lumbricals and interossei have long been accepted as not only primary agents in flexing the metacarpophalangeal joints -

Anatomical Considerations of Fascial Release in Ulnar Nerve Transposition: a Concept Revisited
LABORATORY INVESTIGATION J Neurosurg 123:1216–1222, 2015 Anatomical considerations of fascial release in ulnar nerve transposition: a concept revisited Mark A. Mahan, MD,1 Jaime Gasco, MD,2 David B. Mokhtee, MD,3 and Justin M. Brown, MD4 1Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona; 2Division of Neurological Surgery, University of Texas Medical Branch, Galveston, Texas; 3Tulsa Bone and Joint Associates, Tulsa, Oklahoma; and 4Division of Neurosurgery, University of California, San Diego, La Jolla, California OBJECT Surgical transposition of the ulnar nerve to alleviate entrapment may cause otherwise normal structures to become new sources of nerve compression. Recurrent or persistent neuropathy after anterior transposition is commonly attributable to a new distal compression. The authors sought to clarify the anatomical relationship of the ulnar nerve to the common aponeurosis of the humeral head of the flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS) muscles following anterior transposition of the nerve. METHODS The intermuscular septa of the proximal forearm were explored in 26 fresh cadaveric specimens. The fibrous septa and common aponeurotic insertions of the flexor-pronator muscle mass were evaluated in relation to the ulnar nerve, with particular attention to the effect of transposition upon the nerve in this region. RESULTS An intermuscular aponeurosis associated with the FCU and FDS muscles was present in all specimens. Transposition consistently resulted in angulation of the nerve during elbow flexion when this fascial septum was not released. The proximal site at which the nerve began to traverse this fascial structure was found to be an average of 3.9 cm (SD 0.7 cm) from the medial epicondyle. -

Rotator Cuff Tears
OrthoInfo Basics Rotator Cuff Tears What is a rotator cuff? One of the Your rotator cuff helps you lift your arm, rotate it, and reach up over your head. most common middle-age It is made up of muscles and tendons in your shoulder. These struc- tures cover the head of your upper arm bone (humerus). This “cuff” complaints is holds the upper arm bone in the shoulder socket. shoulder pain. Rotator cuff tears come in all shapes and sizes. They typically occur A frequent in the tendon. source of that Partial tears. Many tears do not completely sever the soft tissue. Full thickness tears. A full or "complete" tear will split the soft pain is a torn tissue into two, sometimes detaching the tendon from the bone. rotator cuff. Rotator Cuff Bursa A torn rotator cuff will Tendon Clavicle (Collarbone) Humerus weaken your shoulder. (Upper Arm) This means that many Normal shoulder anatomy. daily activities, like combing your hair or Scapula getting dressed, may (Shoulder Blade) become painful and difficult to do. Rotator Cuff Tendon A complete tear of the rotator cuff tendon. 1 OrthoInfo Basics — Rotator Cuff Tears What causes rotator cuff tears? There are two main causes of rotator cuff repeating the same shoulder motions again and tears: injury and wear. again. Injury. If you fall down on your outstretched This explains why rotator cuff tears are most arm or lift something too heavy with a jerking common in people over 40 who participate in motion, you could tear your rotator cuff. This activities that have repetitive overhead type of tear can occur with other shoulder motions.