Rotator Cuff Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Physio Med Self Help for Achilles Tendinopathy
Physio Med Self Help 0113 229 1300 for Achilles Tendinopathy Achilles tendon injuries are common, often evident in middle aged runners to non-sporting individuals. They are often characterised by pain in the tendon, usually at the beginning and end of exercise, pain and stiffness first thing in the morning or after sitting for long periods. There is much that can be done to both speed up the healing and prevent re-occurrence. Anatomy of the Area The muscles of your calf (the gastrocnemius and soleus) are the muscles which create the force needed to push your foot off the floor when walking, running and jumping, or stand up on your toes. The Achilles tendon is the fibrous band that connects these muscles to your heel. You may recognise the term ‘Achilles Tendonitis’ which was the previous name used for Achilles Tendinopathy. However the name has changed as it is no longer thought to be a totally inflammatory condition, but rather an overuse injury causing pain, some localised inflammation and degeneration of the thick Achilles tendon at the back of the ankle. Potential causes of Achilles Tendinopathy and advice on how to prevent it • Poor footwear or sudden change in training surface e.g. sand makes the calf work harder » Wear suitable shoes for the activity (type, fit and condition of footwear). » Take account of the surface you are exercising on and if soft and unstructured like sand or loose soil reduce the intensity / duration or take a short break or reduce any load you are carrying into smaller loads until you become conditioned to it. -

An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them
An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them Patrick S. Buckley, MD University Orthopaedic Associates June 1, 2019 Disclosures • None www.UOANJ.com Anatomy of the Meniscus • Act as functional extensions of the tibial plateaus to increase depth of tibial articular surface • The meniscotibial attachment contributes to knee stability • Triangular in cross-section Gross Anatomy of the Meniscus • Ultrastructural Anatomy – Primarily Type I collagen (90%) – 70% water – Fiber orientation is circumferential (hoop stressing) Meniscal Vascularity • Relatively avascular • Vascular penetration – 10 - 30% medial – 10 - 25% lateral • Non-vascularized portions gain nutrients from mechanical loading and joint motion Medial Meniscus • Semilunar shape • Thin anterior horn • Broader posterior horn • More stable & less motion than the lateral = tears more often Lateral Meniscus • Almost circular in shape • Intimately associated with the ACL tibial insertion • Posterior horn attachments – Ligament of Humphrey – Ligament of Wrisberg • Lateral meniscus is a more dynamic structure with more motion Main Importance of Menisci • Load transmission • Joint stability Load Bearing / Shock Absorption • MM 50% and 70% LM of load transmitted through mensicus in extension • 85 % at 90° of flexion • Meniscectomy – 50 % decrease in contact area – 20 % less shock absorption www.UOANJ.com Meniscal effect on joint stability • Secondary restraints to anterior tibial translation in normal knees • In an ACL-deficient knee: the posterior horn of the medial meniscus is more important than the lateral meniscus Interaction of ACL and PHMM • Lack of MM in ACLD knees significantly ↑ anterior tibial translation at all knee flexion angles • Think about with high grade pivot! (Levy, JBJS,1982) (Allen, JOR,2000) C9ristiani, AJSM, 2017) Meniscus Function -Now known to be important structure for load distribution and secondary stabilizer to the knee. -

Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment
Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment The glenohumeral joint is the most mobile joint in the human body, but this same characteristic also makes it the least stable joint.1-3 The rotator cuff is a group of muscles that are important in supporting the glenohumeral joint, essential in almost every type of shoulder movement.4 These muscles maintain dynamic joint stability which not only avoids mechanical obstruction but also increases the functional range of motion at the joint.1,2 However, dysfunction of these stabilizers often leads to a complex pattern of degeneration, rotator cuff tear arthropathy that often involves subacromial impingement.2,22 Rotator cuff tear arthropathy is strikingly prevalent and is the most common cause of shoulder pain and dysfunction.3,4 It appears to be age-dependent, affecting 9.7% of patients aged 20 years and younger and increasing to 62% of patients of 80 years and older ( P < .001); odds ratio, 15; 95% CI, 9.6-24; P < .001.4 Etiology for rotator cuff pathology varies but rotator cuff tears and tendinopathy are most common in athletes and the elderly.12 It can be the result of a traumatic event or activity-based deterioration such as from excessive use of arms overhead, but some argue that deterioration of these stabilizers is part of the natural aging process given the trend of increased deterioration even in individuals who do not regularly perform overhead activities.2,4 The factors affecting the rotator cuff and subsequent treatment are wide-ranging. The major objectives of this exposition are to describe rotator cuff anatomy, biomechanics, and subacromial impingement; expound upon diagnosis and assessment; and discuss surgical and conservative interventions. -

Musculoskeletal Diagnostic Imaging
Musculoskeletal Diagnostic Imaging Vivek Kalia, MD MPH October 02, 2019 Course: Sports Medicine for the Primary Care Physician Department of Radiology University of Michigan @VivekKaliaMD [email protected] Objectives • To review anatomy of joints which commonly present for evaluation in the primary care setting • To review basic clinical features of particular musculoskeletal conditions affecting these joints • To review key imaging features of particular musculoskeletal conditions affecting these joints Outline • Joints – Shoulder – Hip • Rotator Cuff Tendinosis / • Osteoarthritis Tendinitis • (Greater) Trochanteric bursitis • Rotator Cuff Tears • Hip Abductor (Gluteal Tendon) • Adhesive Capsulitis (Frozen Tears Shoulder) • Hamstrings Tendinosis / Tears – Elbow – Knee • Lateral Epicondylitis • Osteoarthritis • Medical Epicondylitis • Popliteal / Baker’s cyst – Hand/Wrist • Meniscus Tear • Rheumatoid Arthritis • Ligament Tear • Osteoarthritis • Cartilage Wear Outline • Joints – Ankle/Foot • Osteoarthritis • Plantar Fasciitis • Spine – Degenerative Disc Disease – Wedge Compression Deformity / Fracture Shoulder Shoulder Rotator Cuff Tendinosis / Tendinitis • Rotator cuff comprised of 4 muscles/tendons: – Supraspinatus – Infraspinatus – Teres minor – Subscapularis • Theory of rotator cuff degeneration / tearing with time: – Degenerative partial-thickness tears allow superior migration of the humeral head in turn causes abrasion of the rotator cuff tendons against the undersurface of the acromion full-thickness tears may progress to -
Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair
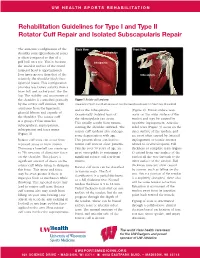
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair The anatomic configuration of the Back View Front View shoulder joint (glenohumeral joint) Supraspinatus is often compared to that of a golf ball on a tee. This is because Infraspinatus the articular surface of the round humeral head is approximately Teres four times greater than that of the Minor Subscapularis relatively flat shoulder blade face (glenoid fossa). This configuration provides less boney stability than a truer ball and socket joint, like the hip. The stability and movement of the shoulder is controlled primarily Figure 1 Rotator cuff anatomy by the rotator cuff muscles, with Image property of Primal Pictures, Ltd., primalpictures.com. Use of this image without authorization from Primal Pictures, Ltd. is prohibited. assistance from the ligaments, and/or the infraspinatus. (Figure 2). Bursal surface tears glenoid labrum and capsule of Occasionally isolated tears of occur on the outer surface of the the shoulder. The rotator cuff the subscapularis can occur. tendon and may be caused by is a group of four muscles: This usually results from trauma repetitive impingement. Articular subscapularis, supraspinatus, rotating the shoulder outward. The sided tears (Figure 3) occur on the infraspinatus and teres minor rotator cuff tendons also undergo inner surface of the tendon, and (Figure 1). some degeneration with age. are most often caused by internal Rotator cuff tears can occur from This process alone can lead to impingement or tensile stresses repeated stress or from trauma. rotator cuff tears in older patients. related to overhead sports. -

Ministry of Health of Ukraine Ukrainian Medical Dental Academy
Ministry of Health of Ukraine Ukrainian Medical Dental Academy Methodical instructions for independent work for students during training to practical (seminar) classes and in class Academic discipline Surgical dentistry Module № 5 Lesson topic № 1 Anatomy of the temporomandibular joint (TMJ). Modern methods of diagnosing TMJ diseases. Arthroscopy, its possibilities in the diagnosis and treatment of TMJ diseases. Dislocations of the mandible: etiology, clinic, diagnosis, treatment. Curation of the patient in the clinic of maxillofacial surgery. Writing an academic medical history. Course V Faculty Stomatological Poltava 2020 1. Relevance of the topic. Knowledge of the anatomical structure of the temporomandibular joint (TMJ) and the characteristics of modern diagnostic methods for assessing their pathologies. The etiology, clinical diagnosis and treatment of mandibular dislocations allows you to choose a timely and effective way to treat this pathology, avoid mistakes and complications, allows the dentist to diagnose TMJ and prescribe optimal treatment. Academic history in which the student is able to use knowledge , obtained in the study of basic and applied sciences, obtained demonstrate practical skills. 2. Specific target: 2 .1.Analyze to know statistics, diseases TMJ.; 2.2. Explain the methods of diagnosing diseases TMJ; 2.3. To offer to examine patients with diseases of TMJ; 2.4. Classify diseases TMJ; 2.5. Interpret theoretical and clinical studies of diseases TMJ; 2.6. Draw diagrams, graphs 2.7. Analyze the treatment plan for patients with diseases TMJ; 2.8. Make a plan for the treatment of patients with diseases TMJ; 3. Basic knowledge, skills, abilities necessary for studying the topic (interdisciplinary integration). Names of previous Acquired skills disciplines Anatomy To study the anatomical and topographic structure of the temporomandibular joint. -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz. -

Primary and Secondary Consequences of Rotator Cuff
Hafizur Rahman Department of Mechanical Science and Engineering, University of Illinois at Urbana-Champaign, Urbana, IL 61801 Primary and Secondary e-mail: [email protected] Consequences of Rotator Cuff Eric Currier Department of Mechanical Science and Engineering, Injury on Joint Stabilizing University of Illinois at Urbana-Champaign, Urbana, IL 61801 Tissues in the Shoulder e-mail: [email protected] Rotator cuff tears (RCTs) are one of the primary causes of shoulder pain and dysfunction Marshall Johnson in the upper extremity accounting over 4.5 million physician visits per year with 250,000 Department of Mechanical Engineering, rotator cuff repairs being performed annually in the U.S. While the tear is often consid- Georgia Institute of Technology, ered an injury to a specific tendon/tendons and consequently treated as such, there are Atlanta, GA 30332 secondary effects of RCTs that may have significant consequences for shoulder function. e-mail: [email protected] Specifically, RCTs have been shown to affect the joint cartilage, bone, the ligaments, as well as the remaining intact tendons of the shoulder joint. Injuries associated with the Rick Goding upper extremities account for the largest percent of workplace injuries. Unfortunately, Department of Orthopaedic, the variable success rate related to RCTs motivates the need for a better understanding Joint Preservation Institute of Iowa, of the biomechanical consequences associated with the shoulder injuries. Understanding West Des Moines, IA 50266 the timing of the injury and the secondary anatomic consequences that are likely to have e-mail: [email protected] occurred are also of great importance in treatment planning because the approach to the treatment algorithm is influenced by the functional and anatomic state of the rotator cuff Amy Wagoner Johnson and the shoulder complex in general. -

ANKLE LIGAMENT STRAIN DURING SUPINATION SPRAIN INJURY – a Alt, W., Lohrer, H., & Gollhofer, A
Vilas-Boas, Machado, Kim, Veloso (eds.) Portuguese Journal of Sport Sciences Biomechanics in Sports 29 11 (Suppl. 2), 2011 REFERENCES: ANKLE LIGAMENT STRAIN DURING SUPINATION SPRAIN INJURY – A Alt, W., Lohrer, H., & Gollhofer, A. (1999). FunctionalProperties of Adhesive Ankle Taping: COMPUTATIONAL BIOMECHANICS STUDY Neuromuscular and Mechanical Effects Before and After Exercise. Foot & Ankle International , 20(4), 238-45. Daniel Tik-Pui Fong1,2, Feng Wei3, Youlian Hong4,5, Tron Krosshaug6, Benesch, S., Putz, W., Rosenbaum, D., & Becker, H.-P. (2000). Reliability of Peroneal Reaction Time Roger C. Haut3 and Kai-Ming Chan1,2 Measurements. Clin Biomech , 15. Cordova, M. L., Bernard, L. W., Au, K. K., Demchak, T. J., Stone, M. B., & Sefton, J. M. (2010). Department of Orthopaedics and Traumatology, Prince of Wales Hospital, Cryotherapy and ankle bracing effects on peroneus longus response during sudden inversion. J 1 Electromyogr Kinesiol , 20, 248-53. Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China The Hong Kong Jockey Club Sports Medicine and Health Sciences Centre, Delahunt, E. (2007). Peroneal reflex contribution to the development of functional instability of the 2 ankle joint. Phys Ther Sport , 8, 98-104. Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China 3 Docherty, C. L., & Arnold, B. L. (2008). Force sence deficits in functionally unstable ankles. J Orthop Orthopaedic Biomechanics Laboratories, Michigan State University, USA Res , 26(11), 1489-93. Department of Sports Science and Physical Education, Faculty of Education, 4 Eechaute, C., Vaes, P., Duquet, W., & Gheluwe, B. v. (2009). Reliability ans discriminative validity of The Chinese University of Hong Kong, Hong Kong, China sudden ankle inversion measurements in patients with chronic ankle instability. -

Impingement Syndrome and Tears of the Rotator Cuff
Impingement Syndrome and Tears of the Rotator Cuff Dr Keith Holt Impingement is a very common problem in which the tendons of the rotator cuff (predominantly supraspinatus) rub on the underside of the acromion (the bone at the point of the shoulder). This causes pain due to the repeated rubbing of those tendons and it is especially bad with certain positions of the arm. In particular it is difficult to put the arm behind the back and to use it in the elevated position. This makes it difficult to drive, change gears, hang clothes, comb one’s hair, and even to lie on the affected shoulder. The cause of this problem can be: How does the shoulder work? The shoulder, like the hip, is a ball and socket joint (like a tow 1) A muscle imbalance problem due to poor functioning bar). Unlike the hip however, the socket is very small and is of the rotator cuff tendons themselves; thus allowing the not big enough to hold the head of the humerus (the ball) arm to ride up and rub on the acromion, squashing the in place. This gives the joint a large range of motion but, as rotator cuff tendons in the process: or a consequence, it also means that it is potentially unstable. 2) A mechanical problem where the space for the tendon To function normally, muscles on both sides of the joint must is inadequate. One way this can occur is with an injury work together to hold the joint in place during movement. to the tendon itself which causes swelling of that tendon This means that when the deltoid muscle (see diagrams) lifts such that it becomes too large for the space at hand the arm out from the side of the body, the supraspinatus and [primary tendonitis (inflammation of the tendon) with other muscles of the rotator cuff must pull down on the top secondary impingement [rubbing of the tendon on the of the humerus. -

Rotator Cuff Tears
OrthoInfo Basics Rotator Cuff Tears What is a rotator cuff? One of the Your rotator cuff helps you lift your arm, rotate it, and reach up over your head. most common middle-age It is made up of muscles and tendons in your shoulder. These struc- tures cover the head of your upper arm bone (humerus). This “cuff” complaints is holds the upper arm bone in the shoulder socket. shoulder pain. Rotator cuff tears come in all shapes and sizes. They typically occur A frequent in the tendon. source of that Partial tears. Many tears do not completely sever the soft tissue. Full thickness tears. A full or "complete" tear will split the soft pain is a torn tissue into two, sometimes detaching the tendon from the bone. rotator cuff. Rotator Cuff Bursa A torn rotator cuff will Tendon Clavicle (Collarbone) Humerus weaken your shoulder. (Upper Arm) This means that many Normal shoulder anatomy. daily activities, like combing your hair or Scapula getting dressed, may (Shoulder Blade) become painful and difficult to do. Rotator Cuff Tendon A complete tear of the rotator cuff tendon. 1 OrthoInfo Basics — Rotator Cuff Tears What causes rotator cuff tears? There are two main causes of rotator cuff repeating the same shoulder motions again and tears: injury and wear. again. Injury. If you fall down on your outstretched This explains why rotator cuff tears are most arm or lift something too heavy with a jerking common in people over 40 who participate in motion, you could tear your rotator cuff. This activities that have repetitive overhead type of tear can occur with other shoulder motions. -

Rotator Cuff 101 Every Year, More Than Two Million American Adults Seek Medical Care for Rotator Cuff Disease
BONE & JOINT BRIEFINGS Rotator Cuff 101 Every year, more than two million American adults seek medical care for rotator cuff disease. he rotator cuff is a series of 4 muscles It’s important to recognize that most people who surrounding the ball and socket joint of have shoulder pain don’t have a rotator cuff tear; the shoulder and plays a crucial role in there are many other causes. Pain from a rotator cuff optimizing shoulder function. The shoulder tear is usually experienced on the lateral aspect of the joint is inherently unstable, as the major arm, almost midway between the shoulder and the Tmuscles that move the shoulder around—the deltoid, elbow. It’s usually worse with overhead activity and the pectoralis, the back muscles—have a tendency worse at night. If this sort of pain is accompanied by to move the ball out of the center of the socket. The weakness, it probably should be checked right away. rotator cuff, almost as a counterforce against the If there’s no weakness involved, just aches and major muscles, helps to provide a stable fulcrum and pain, then ice, anti-inflammatory medication and a to optimize shoulder mechanics. couple of weeks of lighter activity could be all one As you might imagine, the muscles of the rotator needs. However, if the pain continues for more than a Christopher Gorczynski, MD cuff are subjected to quite a bit of stress. Friction couple of weeks, it deserves to be evaluated. Because and heavy usage (through sports or other repetitive the rotator cuff is under tension, tears generally get activity) can cause the tendons of the rotator cuff bigger over time and partial tears can become full- Those of us who are 30, to thicken or become inflamed and get “pinched” thickness tears.