Guidelines for Returning to Weightlifting Following Shoulder Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
GET SWOLE Diet + Training Series DIET + TRAINING GUIDE GET SWOLE FOOD LIST + TRAINING GUIDE
Laron LandrY Pro FOOTBall suPERSTAR PHASE 1 GET SWOLE DIET + TRAINING SERIES DIET + TRAINING GUIDE GET SWOLE FOOD LIST + TRAINING GUIDE MEATS: VEGETABLES: • Chicken • Asparagus • Kale • Mackerel • Bamboo Shoots • Kohlrabi • Salmon • Bean Sprouts • Lettuces • Tuna • Beet Greens • Mushrooms • Lean Beef • Bok Choy Greens • Mustard Greens • Jerky • Broccoli • Parsley • Turkey • Cabbage • Radishes • Lunch Meat Ham • Cauliflower • Salad Greens • Lunch Meat Roast Beef • Celery • Sauerkraut • Eggs • Chards • Spinach String Beans • Chicory • Summer Squashes • Collard Greens • Turnip Greens • Cucumber • Watercress • Endive • Yellow Squash • Escarole • Zucchini Squash • Garlic CARBOHYDRATES: FATS: • Brown Rice • Avocado • Sweet Potato • Almonds • Quinoa • Cashews • Oatmeal • Olive Oil • Whole Wheat Bread • Whole Organic Butter • Ezekiel Bread • Walnuts • Whole Wheat Spaghetti • Kidney Beans • Yams • Black Beans • Barley • Brazil Nuts • Rye Bread • Pumpernickel Bread FRUITS: CONDIMENTS + SEASONINGS: • Apples • Spicy Mustard • Strawberries • Hot Sauce • Papaya • Crushed Red Pepper • Pears • Mrs. Dash Original Blend • Fresh Prunes • Mrs. Dash Fiesta Lime • Orange • Mrs. Dash Extra Spicy • Grapefruit • Mrs. Dash Tomato Basil Garlic • Kiwi • Mrs. Dash Lemon Pepper • Peaches TO SEE “PROPER FORM” EXERCISE VIDEOS,www.bodybuilding VISIT: MUSCLEPHARM.COM.com/getswole GET SWOLE PHASE 1: WEEKS 1–4 + TRAINING GUIDE EX. TIME: 7:00AM SUPPLEMENT: FOOD: Wake Up RE-CON®: 1/2 scoop • 3 whole eggs * Take with 8-12 oz. of water. • 1/4 cup oatmeal • 1 cup of fruit ARMOR-V™: 6 capsules * Take with 8-12 oz. of water. EX. TIME: 10:00AM SUPPLEMENT: FOOD: Mid-Morning COMBAT POWDER®: 2 scoops No Food * Take with 8-12 oz. of water & 2 oz. of heavy whipping cream. EX. TIME: 1:00PM SUPPLEMENT: FOOD: Lunch No Supplement Choose From Food List: Meat: 8 oz. -

Extended Insertion of Teres Minor Muscle: a Rare Case Report
Eur J Anat, 16 (3): 224-225 (2012) CASE REPORT Extended insertion of teres minor muscle: a rare case report Monica Jain, Lovesh Shukla, Dalbir Kaur Maharaja Agrasen Medical College, Agroha-125047, Hisar, Haryana, India SUMMARY upwards and laterally, and gets inserted on the lowest of the three impressions on the greater Teres minor is one of the muscles of the shoul- tubercle of the humerus and fuses with the der joint along with subscapularis, supraspina- capsule of the shoulder joint along with other tus and infraspinatus forming rotator cuff. muscles forming the rotator cuff. It is inner- Variations of teres minor are relatively uncom- vated by the posterior branch of the axillary mon. A unique and extended insertion of this nerve. It stabilizes the humerus by holding muscle is being reported in the present case. the humeral head in the glenoid cavity of the Knowledge of the anatomy of this muscle is scapula, a and causes lateral rotation of the important to avoid injury to the axillary nerve arm (Johnson, 2008). Variations of teres and posterior circumflex humeral vessels while minor are relatively uncommon and have been surgically approaching the shoulder joint and occasionally reported by various authors inserting portals of the arthroscope in a poste- (Bergman et al., 2006). rior approach to the shoulder joint. Key words: Teres minor – Rotator cuff – CASE REPORT Shoulder joint – Capsule of shoulder joint – Humerus – Surgical neck of humerus During routine dissection of the shoulder region of upper limb of an approximately 50 year-old male cadaver for undergraduate teach- INTRODUCTION ing and training, a unique and extended inser- tion of the teres minor muscle was found on the Teres minor is a one of the short scapular right side. -

Tricepsterrific
ACE-SPONSORED RESEARCH TricepsTerrific omen from all walks of life struggle to avoid the dreaded flabby, jiggly arms—and they often turn to personal trainers and fitness pros for help. “Guys always want to get rid of their bellies, while women always By Brittany Boehler,W B.S., seem to want to tone their triceps,” says John P. Porcari, Ph.D., John Porcari, Ph.D., an exercise physiologist Dennis Kline, M.S., with the University of Wisconsin and former C. Russell Hendrix, Ph.D., and personal trainer. Carl Foster, Ph.D., with Mark Anders But as with most clients, their time is constantly being gobbled up by work and family obligations, leaving little extra time for regular exercise. They want results—and fast! With that in mind, the This study was funded solely by the American Council on Exercise, the nation’s Work- American Council on Exercise (ACE). out Watchdog, sponsored comprehensive research to determine which exercises are most effec- tive—and efficient—for targeting the triceps. Armed with this new research, you’ll be able to better guide your clients in their efforts to tone and strengthen their triceps. TheTo determine Study the efficacy of the eight most common triceps exercises, ACE enlisted a team of exercise scientists from the University of Wiscon- sin/La Crosse Exercise and Health Program. Led www.acefitness.org pg. 1 ACE-SPONSORED RESEARCH by John Porcari, Ph.D., and Brittany Boehler, B.S., the exercise to ensure proper muscle recovery. Subjects lifted research team recruited 15 healthy female subjects, ages 70 percent of their previously determined 1 RM for the 20 to 24, from the local La Crosse community. -

Home Workout
HOME WORKOUT 13 MIN AMRAP 12 MIN AMRAP 10 MIN AMRAP 60 sec cardio (run, jumping 60 sec cardio (run, jumping jacks, squat jumps, burpees, jacks, squat jumps, burpees, 20 Seconds Wall Sit mountain climbers, stairs) mountain climbers, stairs) 10 to 1 Pushups 16 Walking Lunges 20 Jumping Jacks 10 to 1 Y Raises 8 Squat Jumps 20 Air Squats 16 Chair Step Ups (8 each) 8 Air Deadlifts 20 Calf Raises (pause at top) *** Y Raise Cans/Water Bottles 8 Knee Tucks 16 sec side plank each side Y RAISE SQUAT JUMP WALL SIT STEP UPS KNEE TUCKS AIR SQUAT HOME WORKOUT 13 MIN AMRAP 10 MIN AMRAP TABATA (20/10)x4 2 min Cardio (run, jumping jacks, squat jumps, burpees, 30 High Knees AB Bicycles Slow mountain climbers, stairs) 8 Squat Jumps 30 Butt Kicks Low Plank (Elbows) 8 Deadlift Jumps 4 Each Way Staggered Pushup AB Bicycles Fast 8 ea Single Leg Glute Bridge 16 Book Front Raise High Plank 16 Air Squat 8 Each Single Arm Row ***20 sec on/10 sec off 16 Air Deadlift ***Home Item for Row Do 4 times through of 20/10 SQUAT JUMP STAGGERED PUSHUP AB BICYCLES SINGLE LEG GLUTE FRONT RAISE HIGH PLANK HOME WORKOUT 12 MIN AMRAP 12 MIN AMRAP TABATA (30/10)x4 45 Seconds Cardio (run, jumping jacks, squat jumps, burpees, 5 Inchworms to Low Plank Quick Jumps (Jump Rope) mountain climbers, stairs) 10 each way home item 8’s 5 Each Leg Lunge Jump or Lunge Air Squat 10 each arm single arm arnold 10 Each Leg Donkey Kick Quick Jumps (Jump Rope) 30 steam engines slow 10 Dead Bugs Step Ups 10 pushups 10 Can Hammer Curls ***30 sec on/10 sec off 10 lying toe touches (legs up) ***Neutral -

The Bench Press Fly's
www.dfwsportsmed.com AC Joint Injuries: Weight-Lifting Exercises to Avoid Adapted from Ollie Odebunmi, Demand Media The acromioclavicular joint, also known as the AC joint, is at the top most point of your shoulder where the collar bone attaches to the shoulder. AC joint injuries are caused by repetitive trauma, falls on the shoulder joint or certain weightlifting exercises. But you don't have to abandon your weightlifting program. Simply modify your technique and avoid the exercises that cause discomfort. The Bench Press Avoid full range of motion barbell or dumbbell bench presses. Excessive stress on the AC joint occurs when your elbows drop below your body on the downward motion. Using heavy weights compounds the problem. The bench press is often seen as a test of strength by weightlifters, and many do the exercise too frequently with near- maximal weights. Limit the stress on your AC joint by not bench pressing every week. Use a towel roll or do the bench press on the floor to prevent the elbows from dropping past the body. Fly’s Flat bench or incline bench dumbbell fly’s with dumbbells lowered in a wide arc out to the sides overextends the shoulder joints. The stress and risk of injury to the AC joint increases if your elbows drop below your body to get a full stretch of the pectorals. Machine fly’s gripping a bar or handles or with forearms against a pad also overextend your shoulder joints on the negative phase of the movement as your elbows travel beyond your shoulder joints. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -
Monday: Back, Biceps, Forearms, Traps & Abs Wednesday
THE TOOLS YOU NEED TO BUILD THE BODY YOU WANT® Store Workouts Diet Plans Expert Guides Videos Tools BULLDOZER TRAINING 3 DAY WORKOUT SPLIT 3 day Bulldozer Training muscle building split. Combines rest-pause sets with progressive Main Goal: Build Muscle Time Per Workout: 30-45 Mins resistance. Workouts are shorter but more Training Level: Intermediate Equipment: Barbell, Bodyweight, intense. Program Duration: 8 Weeks Dumbbells, EZ Bar, Machines Link to Workout: https://www.muscleandstrength.com/ Days Per Week: 3 Days Author: Steve Shaw workouts/bulldozer-training-3-day-workout-split Monday: Back, Biceps, Forearms, Traps & Abs Exercise Mini Sets Rep Goal Rest Deadlift: Perform as many rest-paused singles as you (safely) can within 10 Mins. Use a weight you could easily perform a 10 rep set with. Rest as needed. When you can perform 15 reps, add weight the next time you deadlift. Barbell Row 5 25 30 / 30 / 45 / 45 Wide Grip Pull Up 5 35 30 / 30 / 30 / 30 Standing Dumbbell Curl 4 25 30 / 30 / 30 EZ Bar Preacher Curl 4 25 30 / 30 / 30 Seated Barbell Wrist Curl 4 35 30 / 30 / 30 Barbell Shrug 5 35 30 / 30 / 30 / 30 Preferred Abs Exercise(s): I recommend using at least one weighted exercise (e.g. Weighted Sit Ups or Cable Crunches). Rest Periods: 30 / 30 / 45 / 45 notates rest periods between each set. Take 30 Secs after the 1st set, 30 Secs after the 2nd set, 45 Secs after the 3rd set, etc. After the final set, rest, and move on to the next exercise. -

M1 – Muscled Arm
M1 – Muscled Arm See diagram on next page 1. tendinous junction 38. brachial artery 2. dorsal interosseous muscles of hand 39. humerus 3. radial nerve 40. lateral epicondyle of humerus 4. radial artery 41. tendon of flexor carpi radialis muscle 5. extensor retinaculum 42. median nerve 6. abductor pollicis brevis muscle 43. flexor retinaculum 7. extensor carpi radialis brevis muscle 44. tendon of palmaris longus muscle 8. extensor carpi radialis longus muscle 45. common palmar digital nerves of 9. brachioradialis muscle median nerve 10. brachialis muscle 46. flexor pollicis brevis muscle 11. deltoid muscle 47. adductor pollicis muscle 12. supraspinatus muscle 48. lumbrical muscles of hand 13. scapular spine 49. tendon of flexor digitorium 14. trapezius muscle superficialis muscle 15. infraspinatus muscle 50. superficial transverse metacarpal 16. latissimus dorsi muscle ligament 17. teres major muscle 51. common palmar digital arteries 18. teres minor muscle 52. digital synovial sheath 19. triangular space 53. tendon of flexor digitorum profundus 20. long head of triceps brachii muscle muscle 21. lateral head of triceps brachii muscle 54. annular part of fibrous tendon 22. tendon of triceps brachii muscle sheaths 23. ulnar nerve 55. proper palmar digital nerves of ulnar 24. anconeus muscle nerve 25. medial epicondyle of humerus 56. cruciform part of fibrous tendon 26. olecranon process of ulna sheaths 27. flexor carpi ulnaris muscle 57. superficial palmar arch 28. extensor digitorum muscle of hand 58. abductor digiti minimi muscle of hand 29. extensor carpi ulnaris muscle 59. opponens digiti minimi muscle of 30. tendon of extensor digitorium muscle hand of hand 60. superficial branch of ulnar nerve 31. -

Girls Level 3 Gymnastics Prerequisites
Girls Level 2 Gymnastics Girls Level 3 Gymnastics Girls Level 1 Gymnastics Prerequisites: Tumbling Skills: Prerequisites Prerequisites: Forward Rolls: tuck/ straddle Tumbling Skills: Backward Rolls: tuck/ straddle Handstand Straight arm forward roll Pike Backward roll Interest in gymnastics Cartwheels: Side: Left & Right One arm cartwheels Front: Left & Right Far Arm: Left & Right Run, Hurdle Cartwheel Near Arm: Left & Right Headstand/ with forward roll Round-off Single leg lift/ Handstand/ Hand stand Handstand (3 sec hold): Straight/ with forward roll Straddle/ Split Bridges/ from hand stand Back-bend kick-over Backbend Front Limber Scales Split leap/ full turn/ Fouette /Tour Jete 1/2 turns in coupe Uneven Bars: Jumps: straight/ tuck/straddle/ pike/ 45° casts/Jump glide full turns Straight arm jump to support Uneven Bars: Single leg shoot through Pullover & Cast Single leg up-rise Glide/ Pike to toe touch Forward stride circle Long hang swing/ w/ ½ turn Pull over from hang Back hip circle Cast, long hand swing / w/ ½ turn Single leg cut/ Jump on squat Balance Beam: Jump to sole circle dismount Floor/low beam: cartwheel/split leap/ Balance Beam: full turns Mounts/ Dismounts-jumps High Beam: Small jumps/leaps Walks on toes: forwards/ backwards/ Walks (coupe /passe ) on releve sideways on both sides Kick turns Dip Step kick walk ¾ handstand Pivot turns/ ½ turn coupe Round off dismount Straight jumps Forward roll/Backward roll Sissone Vaulting Skills: Scales From board to mats: Assemble Forward -
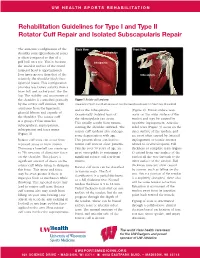
Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Type I and Type II Rotator Cuff Repair and Isolated Subscapularis Repair The anatomic configuration of the Back View Front View shoulder joint (glenohumeral joint) Supraspinatus is often compared to that of a golf ball on a tee. This is because Infraspinatus the articular surface of the round humeral head is approximately Teres four times greater than that of the Minor Subscapularis relatively flat shoulder blade face (glenoid fossa). This configuration provides less boney stability than a truer ball and socket joint, like the hip. The stability and movement of the shoulder is controlled primarily Figure 1 Rotator cuff anatomy by the rotator cuff muscles, with Image property of Primal Pictures, Ltd., primalpictures.com. Use of this image without authorization from Primal Pictures, Ltd. is prohibited. assistance from the ligaments, and/or the infraspinatus. (Figure 2). Bursal surface tears glenoid labrum and capsule of Occasionally isolated tears of occur on the outer surface of the the shoulder. The rotator cuff the subscapularis can occur. tendon and may be caused by is a group of four muscles: This usually results from trauma repetitive impingement. Articular subscapularis, supraspinatus, rotating the shoulder outward. The sided tears (Figure 3) occur on the infraspinatus and teres minor rotator cuff tendons also undergo inner surface of the tendon, and (Figure 1). some degeneration with age. are most often caused by internal Rotator cuff tears can occur from This process alone can lead to impingement or tensile stresses repeated stress or from trauma. rotator cuff tears in older patients. related to overhead sports. -

Exercise of the Month: Reverse Dumbbell
Exercise of the Month Reverse Dumbbell Fly Purpose: To increase overall size and strength to the upper posterior body. Mainly targets the upper back muscles which also act as very powerful spinal stabilizers for posture. Target Muscles: Rhomboids, Rear Deltoids, Middle trapezius Equipment Needed: Dumbbells, or equally weighted soup cans/water bottles Start/Movement: Front view: Side view: • Grab a pair of dumbbells that is appropriate to perform the exercise. Stand shoulder width apart with a slight bend in your knees. • Bend forward at your hips until your torso is at a 45-degree angle, chest up and core fully engaged. Try to remain in this position throughout the entire set. • Bring the dumbbells straight down parallel to the floor, your palms facing each other, with your arms slightly bent. • Raise both arms out to the sides keeping the slight bend in your arms as you squeeze your shoulder blades together. Don’t go past shoulder height when you lift the dumbbells. • Perform the exercise for 3 sets of 8-12 reps. Tips: • When you’re lifting the dumbbells, you should be focused on squeezing your shoulder blades together. • Keep your core fully engaged so that you don't apply too much pressure on your lower back or neck. • Keep your chest open to the ground which will ensure you use your upper back and deltoids to lift the dumbbells. Click here for a video demonstration of this exercise! From Corporate Fitness Works Team Leader: Kameron Arey. -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz.