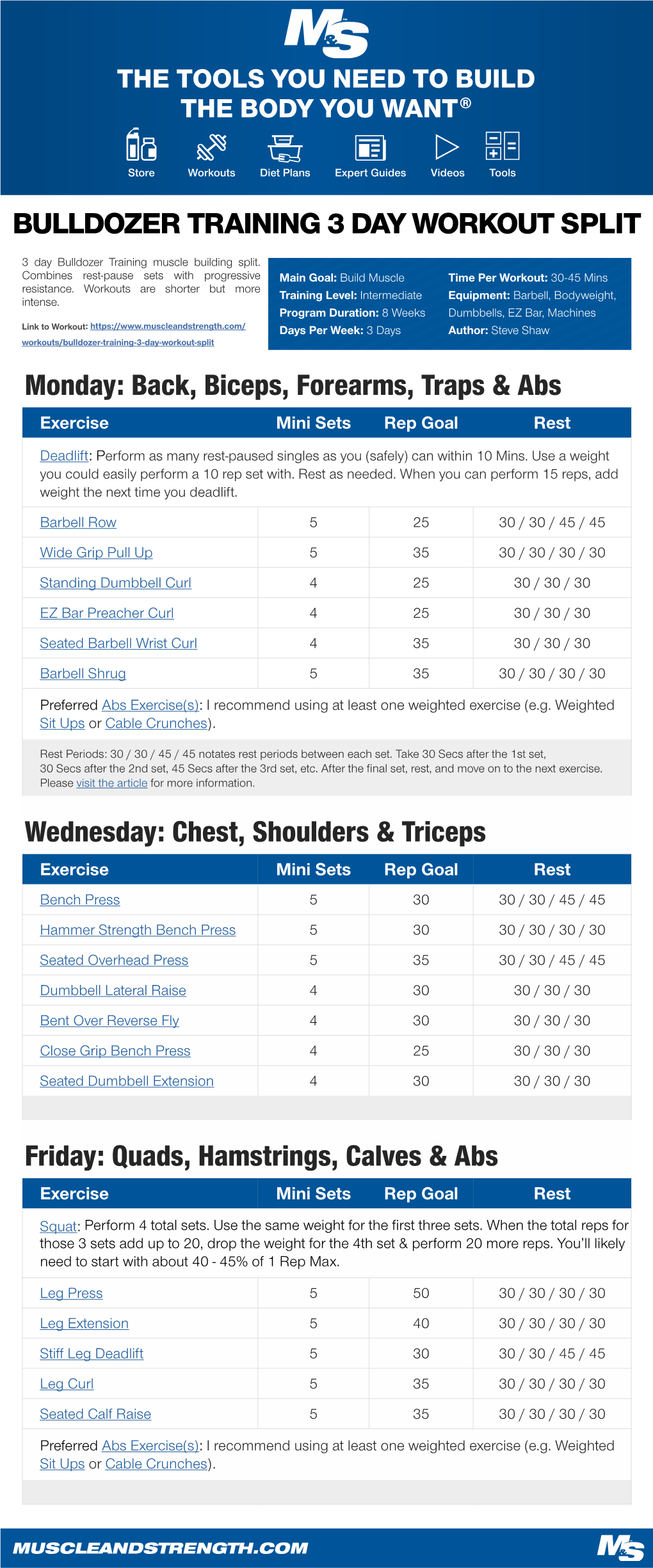
Monday: Back, Biceps, Forearms, Traps & Abs Wednesday
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Extended Insertion of Teres Minor Muscle: a Rare Case Report
Eur J Anat, 16 (3): 224-225 (2012) CASE REPORT Extended insertion of teres minor muscle: a rare case report Monica Jain, Lovesh Shukla, Dalbir Kaur Maharaja Agrasen Medical College, Agroha-125047, Hisar, Haryana, India SUMMARY upwards and laterally, and gets inserted on the lowest of the three impressions on the greater Teres minor is one of the muscles of the shoul- tubercle of the humerus and fuses with the der joint along with subscapularis, supraspina- capsule of the shoulder joint along with other tus and infraspinatus forming rotator cuff. muscles forming the rotator cuff. It is inner- Variations of teres minor are relatively uncom- vated by the posterior branch of the axillary mon. A unique and extended insertion of this nerve. It stabilizes the humerus by holding muscle is being reported in the present case. the humeral head in the glenoid cavity of the Knowledge of the anatomy of this muscle is scapula, a and causes lateral rotation of the important to avoid injury to the axillary nerve arm (Johnson, 2008). Variations of teres and posterior circumflex humeral vessels while minor are relatively uncommon and have been surgically approaching the shoulder joint and occasionally reported by various authors inserting portals of the arthroscope in a poste- (Bergman et al., 2006). rior approach to the shoulder joint. Key words: Teres minor – Rotator cuff – CASE REPORT Shoulder joint – Capsule of shoulder joint – Humerus – Surgical neck of humerus During routine dissection of the shoulder region of upper limb of an approximately 50 year-old male cadaver for undergraduate teach- INTRODUCTION ing and training, a unique and extended inser- tion of the teres minor muscle was found on the Teres minor is a one of the short scapular right side. -

Tricepsterrific
ACE-SPONSORED RESEARCH TricepsTerrific omen from all walks of life struggle to avoid the dreaded flabby, jiggly arms—and they often turn to personal trainers and fitness pros for help. “Guys always want to get rid of their bellies, while women always By Brittany Boehler,W B.S., seem to want to tone their triceps,” says John P. Porcari, Ph.D., John Porcari, Ph.D., an exercise physiologist Dennis Kline, M.S., with the University of Wisconsin and former C. Russell Hendrix, Ph.D., and personal trainer. Carl Foster, Ph.D., with Mark Anders But as with most clients, their time is constantly being gobbled up by work and family obligations, leaving little extra time for regular exercise. They want results—and fast! With that in mind, the This study was funded solely by the American Council on Exercise, the nation’s Work- American Council on Exercise (ACE). out Watchdog, sponsored comprehensive research to determine which exercises are most effec- tive—and efficient—for targeting the triceps. Armed with this new research, you’ll be able to better guide your clients in their efforts to tone and strengthen their triceps. TheTo determine Study the efficacy of the eight most common triceps exercises, ACE enlisted a team of exercise scientists from the University of Wiscon- sin/La Crosse Exercise and Health Program. Led www.acefitness.org pg. 1 ACE-SPONSORED RESEARCH by John Porcari, Ph.D., and Brittany Boehler, B.S., the exercise to ensure proper muscle recovery. Subjects lifted research team recruited 15 healthy female subjects, ages 70 percent of their previously determined 1 RM for the 20 to 24, from the local La Crosse community. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -

M1 – Muscled Arm
M1 – Muscled Arm See diagram on next page 1. tendinous junction 38. brachial artery 2. dorsal interosseous muscles of hand 39. humerus 3. radial nerve 40. lateral epicondyle of humerus 4. radial artery 41. tendon of flexor carpi radialis muscle 5. extensor retinaculum 42. median nerve 6. abductor pollicis brevis muscle 43. flexor retinaculum 7. extensor carpi radialis brevis muscle 44. tendon of palmaris longus muscle 8. extensor carpi radialis longus muscle 45. common palmar digital nerves of 9. brachioradialis muscle median nerve 10. brachialis muscle 46. flexor pollicis brevis muscle 11. deltoid muscle 47. adductor pollicis muscle 12. supraspinatus muscle 48. lumbrical muscles of hand 13. scapular spine 49. tendon of flexor digitorium 14. trapezius muscle superficialis muscle 15. infraspinatus muscle 50. superficial transverse metacarpal 16. latissimus dorsi muscle ligament 17. teres major muscle 51. common palmar digital arteries 18. teres minor muscle 52. digital synovial sheath 19. triangular space 53. tendon of flexor digitorum profundus 20. long head of triceps brachii muscle muscle 21. lateral head of triceps brachii muscle 54. annular part of fibrous tendon 22. tendon of triceps brachii muscle sheaths 23. ulnar nerve 55. proper palmar digital nerves of ulnar 24. anconeus muscle nerve 25. medial epicondyle of humerus 56. cruciform part of fibrous tendon 26. olecranon process of ulna sheaths 27. flexor carpi ulnaris muscle 57. superficial palmar arch 28. extensor digitorum muscle of hand 58. abductor digiti minimi muscle of hand 29. extensor carpi ulnaris muscle 59. opponens digiti minimi muscle of 30. tendon of extensor digitorium muscle hand of hand 60. superficial branch of ulnar nerve 31. -

Triceps Exercises.Pdf
Ultimate Personal Training Triceps Exercise Guide Major Muscles That Act On the Elbow and Forearm MUSCLE ORIGIN INSERTION PRIMARY FUNCTIONS Brachialis Anterior humerous Ulnar tuberosity and Flexion at elbow coronoid process of ulna Triceps Long head from lower edge of glenoid cavity of Olecranon process of Extension at elbow brachii scapula; lateral head from posterior humerus; ulna short head from distal two-thirds of posterior humerus Pronator Distal end of medial humerus and medial aspect Middle third of lateral Flexion at elbow; teres of ulna radius pronation at forearm Triceps exercises.doc Page 1 of 21 Bench Tricep Dips Exercise Data Main Muscle Worked: Triceps Other Muscles Worked: Chest Equipment: BodyOnly Mechanics Type: Compound Tips: Place two flat benches parallel to each other, about three to four feet apart. Sit on one bench facing the other, with your hands grasping the side of the bench. Using your hands to support your weight, lift your feet to the top of the other bench so that the rest of your body is suspended between the two benches. Cross one foot over the other. Slowly lower your body toward the floor by bending your elbows until your upper arms and forearms form a right angle. Do not go below a 90-degree angle, as this can stress your shoulders. Slowly raise back up to the start position by straightening your arms. You can also place a weight plate on your upper legs for added resistance! Lying Cable Triceps Extension Exercise Data Main Muscle Worked: Triceps Other Muscles Worked: None Equipment: Cable Mechanics Type: Isolation Tips: Lie on a bench and grasp a short bar with a narrow overhand grip. -

Rotator Cuff 101 Every Year, More Than Two Million American Adults Seek Medical Care for Rotator Cuff Disease
BONE & JOINT BRIEFINGS Rotator Cuff 101 Every year, more than two million American adults seek medical care for rotator cuff disease. he rotator cuff is a series of 4 muscles It’s important to recognize that most people who surrounding the ball and socket joint of have shoulder pain don’t have a rotator cuff tear; the shoulder and plays a crucial role in there are many other causes. Pain from a rotator cuff optimizing shoulder function. The shoulder tear is usually experienced on the lateral aspect of the joint is inherently unstable, as the major arm, almost midway between the shoulder and the Tmuscles that move the shoulder around—the deltoid, elbow. It’s usually worse with overhead activity and the pectoralis, the back muscles—have a tendency worse at night. If this sort of pain is accompanied by to move the ball out of the center of the socket. The weakness, it probably should be checked right away. rotator cuff, almost as a counterforce against the If there’s no weakness involved, just aches and major muscles, helps to provide a stable fulcrum and pain, then ice, anti-inflammatory medication and a to optimize shoulder mechanics. couple of weeks of lighter activity could be all one As you might imagine, the muscles of the rotator needs. However, if the pain continues for more than a Christopher Gorczynski, MD cuff are subjected to quite a bit of stress. Friction couple of weeks, it deserves to be evaluated. Because and heavy usage (through sports or other repetitive the rotator cuff is under tension, tears generally get activity) can cause the tendons of the rotator cuff bigger over time and partial tears can become full- Those of us who are 30, to thicken or become inflamed and get “pinched” thickness tears. -

Pronator Teres Tear at the Myotendinous Junction in the Recreational Golfer: a Case Report
International Journal of Orthopaedics Online Submissions: http: //www.ghrnet.org/index.php/ijo Int. J. of Orth. 2021 April 28; 8(2): 1457-1462 doi: 10.17554/j.issn.2311-5106.2021.08.405 ISSN 2311-5106 (Print), ISSN 2313-1462 (Online) CASE REPORT Pronator Teres Tear at the Myotendinous Junction in the Recreational Golfer: A Case Report Alvarho J. Guzman1, BA; Stewart A. Bryant1, MD; Shane M. Rayos Del Sol1, BS, MS; Brandon Gardner1, MD, PhD; Moyukh O. Chakrabarti1, MBBS; Patrick J. McGahan1, MD; James L. Chen1, MD 1 Department of Orthopedic Surgery, Advanced Orthopedics & was expected to make a complete return to pre-injury level athletic Sports Medicine, San Francisco, CA, the United States. activity with conservative management. With this article, we consider biceps rupture on the differential diagnoses associated with pronator Conflict-of-interest statement: The author(s) declare(s) that there teres musculotendinous injuries, emphasize the significance of club is no conflict of interest regarding the publication of this paper. type in relation to golfing injuries, and propose a potential pronator teres rupture non-operative rehabilitation protocol. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external Key words: Pronator teres; Golf; Biceps; Ecchymosis; Rehabilitation reviewers. It is distributed in accordance with the Creative Com- protocol mons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- © 2021 The Author(s). Published by ACT Publishing Group Ltd. All commercially, and license their derivative works on different terms, rights reserved. -

Guidelines for Returning to Weightlifting Following Shoulder Surgery
Guidelines for Returning to Weightlifting Following Shoulder Surgery Before initiating any type of weight training, you must have full range of motion of the shoulder and normal strength of the rotator cuff and scapular muscle groups. Your motion and strength should be tested by COLUMBIA UNIVERSITY your surgeon before beginning any weightlifting regimen. CENTER FOR SHOULDER, ELBOW AND SPORTS The following illustrates the approximate time table for beginning MEDICINE weight training following your particular surgery: Rotator Cuff Repair: 6 months Christopher S. Ahmad, MD Bankart Repair: 3 months Office (212) 305-5561 Labrum Repair: 4-6 months Fax (212) 305-4040 Arthroscopic Subacromial Decompression: 4-6 months Louis U. Bigliani, MD When beginning a weight training program, you should start with low Office (212) 305-5564 weights and with 3 sets of 15-20 repetitions. The high repetition sets Fax (212) 305-0999 will ensure that the weights you are using are not too heavy. NEVER perform any weightlifting exercise to the point of muscle failure. Edwin Cadet, MD Muscle failure occurs when the muscle is no longer able to provide the Office (212) 305-4626 energy necessary to contract and move the joints involved in the Fax (212) 305-4040 particular exercise. When muscle failure occurs, the risk for joint, muscle and tendon injuries is greatly increased. William N. Levine, MD Office (212) 305-0762 Exercises to AVOID: Fax (212) 305-4040 1. Triceps Dips 2. Chest Flies Appointment Scheduling 3. Pull-downs behind the neck (212) 305-4565 4. Wide grip bench press 5. Triceps press overhead Mailing Address: th 6. -

Ulnar Nerve Contribution in the Innervation of the Triceps Brachii Muscle Ulnar Nerve to the Triceps Brachii
ORIGINAL COMMUNICATION Anatomy Journal of Africa. 2017. Vol 6 (1): 834 – 839. ULNAR NERVE CONTRIBUTION IN THE INNERVATION OF THE TRICEPS BRACHII MUSCLE ULNAR NERVE TO THE TRICEPS BRACHII Silva DLR, Barros MP, Freire TGS, Firmino Júnior L, Almeida Filho WRB, Correia Cadeira JSL, Silva NO CorresPondence to Diêgo Lucas Ramos e Silva Rua Prof. Virgilio Guedes, 1391 Ponta Grossa, 57014-220 Maceió, AL. Email: [email protected] ABSTRACT The ulnar nerve is considered the thickest terminal branch of the medial cord in the brachial Plexus and most authors does not mention the possibility of this nerve emitting branches to the arm. However, some studies rePorted that the ulnar nerve could suPPly the medial head of triceps brachii muscle. The main objective in this study was identifying the Presence of ulnar nerve branches in tricePs brachii muscle. Sixty uPPer limbs of adult Brazilian corpses of both sexes were used. The estimated age was between 25 and 80 years old. Every studied piece had the nerves and their branches quantified and measured with a manual mechanic caliper. The branches were photographed and had the data registered in individual files. Were found ulnar nerve branches for all the heads of tricePs brachii muscle: 1 branch (9,1%) to lateral head, 2 branches (18,1%) to long head and 8 branches (72,7%) to medial head. Thus, we can conclude that the contribution of ulnar nerve to tricePs brachii muscle constitutes an imPortant anatomical variation. Key words: Ulnar nerve; Triceps brachii muscle; Innervation. INTRODUCTION The ulnar nerve is the terminal branch of the communication with the radial nerve (Bekler et medial cord of the brachial Plexus, receiving C8 al, 2009). -

Workout Plan Pdf
WORKOUT PLAN PDF 17 INCHES – ARMS TRAINING PROGRAM 17 INCHES is a 10 weeks Arm training program to build size of Biceps & Triceps. This will help to gain 1-2 inches arms size and 8-10 pounds of muscle mass in 10 weeks. Follow the exact workout & nutrition plan for the proper results. GURU MANN – Nutritionist & Advanced Fitness Professional United States Guru Mann Fitness Inc. WORKOUT SPLIT OPTION 1 OPTION 2 MONDAY STRENGTH – BICEPS/TRICEPS ------ TUESDAY ------ STRENGTH – BICEPS/TRICEPS WEDNESDAY ------ ------ THURSDAY ENDURANCE – BICEPS/TRICEPS ------ FRIDAY ------ ENDURANCE – BICEPS/TRICEPS SATURDAY ------ ------ SUNDAY REST REST Combine it with other workout plan STRENGTH EXERCISES SETS REPS ALTERNATE EXERCISES 0 WARM UP DB CURL OR EMPLY BARBELL 2-3 15-20 --------- TRICEPS PUSHDOWN 1 SUPER SET 1A. EZ BARBELL CURL 3 8-7-6 STRAIGHT BAR CURL 1B. HAMMER CURL 2 SUPER SET 2A. BARBELL PREACHER CURL 3 8-7-6 DB PREACHER CURL 2B. DB CON. CURL 3 SUPER SET 3A. ROPE CURL 3 8-7-6 CLOSE GRIP BAR 3B. ROPE OVERHEAD EXT. CURL 4 SUPER SET 4A. SKULL CRUSHER 3 8-7-6 ---------- 4B. DB KICKBACK 5 SUPER SET 5A. DB OVERHEAD EXT. 3 8-7-6 5B. WEIGHTED CLOSE GRIP ---------- INCLINE PUSHUP 6 SUPER SET 6A. WRIST CURL (PALM UP) 3 8-7-6 WRIST CURL (PALM 6B. STANDING WRIST CURL FACING DOWN) REST IS 2-3 MIN IN BETWEEN THE SET. THERE IS NO REST IN-BETWEEN THE SUPER SET. ENDURANCE EXERCISES SETS REPS ALTERNATE EXERCISES 0 WARM UP DB CURL OR EMPLY BARBELL 3 15-20 --------- TRICEPS PUSHDOWN 1 SUPER SET 1A. -

Anatomy, Biomechanics, Physiology, Diagnosis and Treatment of Teres
ANATOMY, BIOMECHANICS, PHYSIOLOGY, DIAGNOSIS AND TREATMENT OF TERES MAJOR STRAINS IN THE CANINE Laurie Edge-Hughes, BScPT, CAFCI, CCRT Four Leg Rehabilitation Therapy & The Canine Fitness Centre Ltd, Calgary, AB, Canada The Canadian Horse and Animal Physical Rehabilitation Assn. The Animal Rehab Institute, Loxahatchee, Florida, USA BACKGROUND The canine shoulder apparatus is unique as compared to other canine joints and also when compared to the human shoulder. When compared to the hind limb it is interesting to note that the front limb has no boney attachment to the axial skeleton in that there is no clavicle in the canine. This factor alone means that muscular strength and co-ordination is of utmost importance to full functioning of the front limb. When compared to the human shoulder, one obvious difference is that the shoulder joint is a weight bearing joint. The orientation of the canine scapula and humerus is vertical and the weight distribution is 60 to 65 % on the front legs and 40 – 35% on the hind legs. Essentially dogs are like ‘front wheel drive vehicles’, designed to propel themselves forward by primarily ‘pulling’ from the front end. This is why identification and treatment of front limb muscle injuries is critically important for athletic or just high energy dogs who are most prone to injuring shoulder muscles. The teres major muscle is one that is commonly strained, often unidentified and hence not as effectively treated as it could be in the active canine patient. ANATOMY The teres major muscle originates from the caudal angle and caudal edge of the scapula and inserts into the eminence on the proximal 1/3 of the medial surface of the humerus. -

Neurotization to Innervate the Deltoid and Biceps: 3 Cases
SCIENTIFIC ARTICLE Neurotization to Innervate the Deltoid and Biceps: 3 Cases Christopher J. Dy, MD, MSPH, Alison Kitay, MD, Rohit Garg, MBBS, Lana Kang, MD, Joseph H. Feinberg, MD, Scott W. Wolfe, MD Purpose To describe our experience using direct muscle neurotization as a treatment adjunct during delayed surgical reconstruction for traumatic denervation injuries. Methods Three patients who had direct muscle neurotization were chosen from a consecutive series of patients undergoing reconstruction for brachial plexus injuries. The cases are presented in detail, including long-term clinical follow-up at 2, 5, and 10 years with accompanying postoperative electrodiagnostic studies. Postoperative motor strength using British Medical Research Council grading and active range of motion were retrospectively extracted from the clinical charts. Results Direct muscle neurotization was performed into the deltoid in 2 cases and into the biceps in 1 case after delays of up to 10 months from injury. Two patients had recovery of M4 strength, and the other patient had recovery of M3 strength. All 3 patients had evidence on electrodiagnostic studies of at least partial muscle reinnervation after neurotization. Conclusions Direct muscle neurotization has shown promising results in numerous basic science investigations and a limited number of clinical cases. The current series provides additional clinical and electrodiagnostic evidence that direct muscle neurotization can successfully provide reinnervation, even after lengthy delays from injury to surgical treatment. Clinical relevance Microsurgeons should consider direct muscle neurotization as a viable adjunct treatment and part of a comprehensive reconstructive plan, especially for injuries associated with avulsion of the distal nerve stump from its insertion into the muscle.