Protocol of the Cologne Corona Surveillance (Cocos) Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Interreg I / Ii : Cross-Border Cooperation
INTERREG I / II : CROSS-BORDER COOPERATION Euregio Meuse-Rhine: implementation and management in practice Speech by Mr K.H. Lambertz - Chair of the Monitoring Committee for the Euregio Meuse-Rhine Interreg Programme - Director of Euregio Meuse-Rhine - Minister-President of the German-speaking community of Belgium 1. General background and geographical situation In 1974, the governors of the Dutch and Belgian provinces of Limburg, together with the Chief Executive of the Cologne county administration, acted on the proposal made to them by the future Queen of the Netherlands, Princess Beatrix, during an official visit to Maastricht, to draw up draft arrangements for an association under which even closer cross-border collaboration could develop, along the lines of the Dutch-German Euregio project that had been running since 1957. This initiative was part of the new Community direction in regional policy, which in 1975 was to be provided with an instrument to assist economic development called the European Regional Development Fund (ERDF). In 1976, the principle of cross-border institutions was passed in law. Initially formed as an ad hoc association, the Euregio Meuse-Rhine was designed to promote integration between inhabitants on each side of the national borders. The area covers: • in Holland: the southern part of the Dutch province of Limburg; • in Germany: the city of Aachen, and the districts of Aachen, Heinsberg, Düren and Euskirchen, which make up the Aachen Regio, and • in Belgium: the entire province of Limburg. The province of Liège joined the Euregio Meuse-Rhine in 1978. In 1992, the German-speaking community of Belgium became the fifth partner in the Euregio Meuse- Rhine. -

The Districts of North Rhine-Westphalia
THE DISTRICTS OF NORTH RHINE-WESTPHALIA S D E E N R ’ E S G N IO E N IZ AL IT - G C CO TIN MPETENT - MEE Fair_AZ_210x297_4c_engl_RZ 13.07.2007 17:26 Uhr Seite 1 Sparkassen-Finanzgruppe 50 Million Customers in Germany Can’t Be Wrong. Modern financial services for everyone – everywhere. Reliable, long-term business relations with three quarters of all German businesses, not just fast profits. 200 years together with the people and the economy. Sparkasse Fair. Caring. Close at Hand. Sparkassen. Good for People. Good for Europe. S 3 CONTENTS THE DIstRIct – THE UNKnoWN QUAntITY 4 WHAT DO THE DIstRIcts DO WITH THE MoneY? 6 YoUTH WELFARE, socIAL WELFARE, HEALTH 7 SecURITY AND ORDER 10 BUILDING AND TRAnsPORT 12 ConsUMER PRotectION 14 BUSIness AND EDUCATIon 16 NATURE conseRVAncY AND enVIRonMentAL PRotectIon 18 FULL OF LIFE AND CULTURE 20 THE DRIVING FORce OF THE REGIon 22 THE AssocIATIon OF DIstRIcts 24 DISTRIct POLICY AND CIVIC PARTICIPATIon 26 THE DIRect LIne to YOUR DIstRIct AUTHORITY 28 Imprint: Editor: Dr. Martin Klein Editorial Management: Boris Zaffarana Editorial Staff: Renate Fremerey, Ulrich Hollwitz, Harald Vieten, Kirsten Weßling Translation: Michael Trendall, Intermundos Übersetzungsdienst, Bochum Layout: Martin Gülpen, Minkenberg Medien, Heinsberg Print: Knipping Druckerei und Verlag, Düsseldorf Photographs: Kreis Aachen, Kreis Borken, Kreis Coesfeld, Ennepe-Ruhr-Kreis, Kreis Gütersloh, Kreis Heinsberg, Hochsauerlandkreis, Kreis Höxter, Kreis Kleve, Kreis Lippe, Kreis Minden-Lübbecke, Rhein-Kreis Neuss, Kreis Olpe, Rhein-Erft-Kreis, Rhein-Sieg-Kreis, Kreis Siegen-Wittgenstein, Kreis Steinfurt, Kreis Warendorf, Kreis Wesel, project photos. © 2007, Landkreistag Nordrhein-Westfalen (The Association of Districts of North Rhine-Westphalia), Düsseldorf 4 THE DIstRIct – THE UNKnoWN QUAntITY District identification has very little meaning for many people in North Rhine-Westphalia. -

I Online Supplementary Data – Lötters, S. Et Al.: the Amphibian Pathogen Batrachochytrium Salamandrivorans in the Hotspot Of
Online Supplementary data – Lötters, S. et al.: The amphibian pathogen Batrachochytrium salamandrivorans in the hotspot of its European invasive range: past – present – future. – Salamandra, 56: 173–188 Supplementary document 1. Published site records (populations) of caudate species from Germany in which Bsal was detected until 2018. Data mostly summarized from Spitzen-van der Sluijs et al. (2016), Dalbeck et al. (2018), Lötters et al. (2018), Schulz et al. (2018) and Wagner et al. (2019a). In addition, new findings from the ongoing laboratory testing (especially quality assurance) of samples collected in same time frame were also included, so that some entries differ from those in the mentioned articles. Specimens tested positive for Bd/Bsal and negative for only Bd are indicated under remarks. Legend: † = dead specimen(s); + = ‘low’ infection load (1–10 GE); ++ = ‘medium’ infection load (> 10–100 GE); +++ = ‘high’ infection load (> 100 GE); CI = credible interval per year. Site District Coordinates Species Year N samples N samples Infection Prevalence 95% Remarks (latitude, tested Bsal- loads per year Bayesian longitude) positive CI Northern Eifel North Rhine-Westphalia, StädteRegion 50.578169, Fire salamander, Salamandra salamandra 2015 22 (of which 21 (of which 96% 79–99% mass mortality, 8 of 16 specimens Belgenbach Aachen 6.278448 16 †) 16 †) had Bd/Bsal co-infections Fire salamander, Salamandra salamandra 2017 12 larvae 0 0 0% 0–26% North Rhine-Westphalia, StädteRegion 50.746724, Northern crested newt, Triturus cristatus 2015 2 -

Ansprechpartnerinnen Und Ansprechpartner
Ansprechpartnerinnen und Ansprechpartner 1 Amtshaftung ............................................................................................................... 4 1.1 Sachbearbeitung Amtshaftung ............................................................................. 4 1.2 Teildezernatsleitung ............................................................................................. 4 2 Dienstunfall ................................................................................................................. 4 2.1 Sachbearbeitung Dienstunfall ............................................................................... 4 2.2 Teildezernatsleitung ............................................................................................. 5 3 Einstellung/ Versetzung .............................................................................................. 5 3.1 Berufskolleg / Seiteneinstieg ................................................................................ 5 3.2 Förderschule ........................................................................................................ 6 3.3 Gesamtschule ...................................................................................................... 6 3.4 Grundschule ......................................................................................................... 6 3.5 Hauptschule/Sekundarschule/ Gemeinschaftsschule/PRIMUS-Schule ................ 7 3.6 Gymnasium/Weiterbildungskolleg ....................................................................... -

A Beacon for the COVID-19 Epidemic Control in Brasil: Seroepidemiological Population-Based Surveys Maria Rita Donalisio1*
LETTER TO THE EDITOR https://doi.org/10.1590/1806-9282.67.01.20200512 A beacon for the COVID-19 epidemic control in Brasil: seroepidemiological population-based surveys Maria Rita Donalisio1* The novel severe acute respiratory syndrome coronavirus 2 infection in the population are useful for assessing the impact (SARS-CoV-2), which was firstly identified in late December of public health interventions and can be used in clinical vac- 2019 in China, has spread rapidly worldwide. However, epi- cine trials. demics are expressed from different forms around the world. Population-based surveys have guided public health mea- The epidemic curves do not follow a “natural path” due to dif- sures in several countries. Cross-sectional studies in Spain have ferent social, epidemiological, and cultural contexts, access to shown the most affected regions around Madrid and the dis- health services and to diagnostic tests, vaccine, and preventive ease transmission9. Furthermore, various authors in Iceland measures in different regions1. Oliveira et al.2 investigated dis- have identified populations at risk10. A study conducted in parities in the clinical profile of coronavirus disease (COVID- Gangelt, Heinsberg district, in Germany, where the first case 19) and in the groups that can be more affected by the dis- of COVID-19 was announced in the country, reported that ease in Brasil, China and Italy since the pandemic beginning. 15% of the city population presented antibodies against SARS- In Brasil, the authors reported the highest percentage of cases CoV-2. The first surveys carried out in the United States, in among individuals aged <60, male, and diabetes-affected ones2. -
200 Dpi Resolution
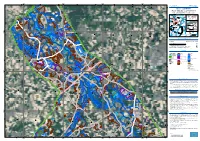
295000 300000 305000 310000 6°4'0"E 6°6'0"E 6°8'0"E 6°10'0"E 6°12'0"E 6°14'0"E 6°16'0"E 6°18'0"E GLIDE number: N/A Activation ID: EMSR517 N " Int. Charter Act. ID: N/A Product N.: 05BONN, v1 0 ' 8 ° 1 5 Bonn - GERMANY Flood - Situation as of 16/07/2021 Delineation MONIT01 - Detail map 04 Sachsen-Anhalt Nordrhein-Westfalen Niedersachsen Zuid-Nederland 06 Vlaams Gewest Detail 04 Detail 02 Detail 03 ThurinBagltice Snea (! Bonn 05 North Sea Region 02 Hessen Wallonne ^ Poland 03 Berlin Rheinland-Pfalz Germany Belgium Czech 01 Republic N France " Saarland 0 Austria ' 0 0 6 0 0 ° 1 Bayern 0 0 Italy 5 Switzerland 5 5 6 6 6 Wassenberg 6 ! 5 5 Est 60 Baden-Wurttemberg km N " 0 ' 6 ° 1 5 Cartographic Information 1:30000 Full color A1, 200 dpi resolution 0 0.5 1 2 km Grid: WGS 1984 UTM Zone 32N map coordinate system Tick marks: WGS 84 geographical coordinate system ± Legend Crisis Information Built-Up Area Hydrography Flooded Area Residential River (16/07/2021 05:41 UTC) General Information Office Stream Area of Interest Wholesale and retail trade Lake Administrative Industrial Land Subject to Inundation boundaries N School, university and research " Reservoir 0 ' International Boundary 4 ° 1 5 River Province Hospital or institutional care Heinsberg Facilities ! Placenames Military ! Dam Placename Cemetery Transportation N Highway Nordrhein-Westfalen " 0 ' 4 ° 1 Primary Road 5 Secondary Road Land Use - Land Cover 0 0 Features available in the vector package 0 0 0 0 0 0 6 6 6 6 5 5 Hückelhoven ! Map Information Heavy rains affected Rhineland-Palatinate area where a severe flood event is expected over E " 0 ' the next few days along the river Moselle. -

COVID-19: Situation Report 8 Mar 2020
Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute 08/03/2020 Confirmed cases Deaths Deaths (%) Coronavirus Disease 2019 Germany 902 0 - (COVID -19) – Changes since the last report have been marked blue in the text – Summary National (as of 08/03/2020, 3 pm) Since 27/01/2020, a total of 902 confirmed cases of SARS-CoV 2 infections (referred to below as COVID-19-cases regardless of their symptoms) were reported in Germany. 15 federal states are affected. Extensive contact tracing by the responsible health authorities is ongoing. The MoH Egypt reported the death due to COVID-19 on 08/03/2020 of a German citizen during his stay in Egypt. 2 COVID-19 Situation Report 08/03/2020 Epidemiological Situation in Germany Case numbers1 A total of 902 (+107) laboratory-confirmed cases of coronavirus disease 2019 (COVID-19) have been detected in Germany since 27/01/2020, of which 447 were electronically reported to and validated at the Robert Koch Institute. Information on laboratory-confirmed cases So far, 902 cases from 179 (+12) rural districts in 15 federal states have been laboratory-confirmed (Table 1). Table 1: Distribution of the laboratory-confirmed COVID-19-cases per federal state in Germany (08/03/2020) Number of Change to Particularly affected areas Federal state cases 07/03/2020 Baden-Württemberg 182 12 Bavaria 172 38 Berlin 40 12 Brandenburg 4 2 Bremen 4 0 Hamburg 13 0 Hesse 19 2 Mecklenburg-Western Pomerania 8 3 Lower Saxony 21 2 North Rhine-Westphalia 398 25 District of Heinsberg Rhineland-Palatinate 19 6 Saarland 9 1 Saxony 4 1 Schleswig-Holstein 7 3 Thuringia 2 0 The cases are between 2 and 91 years old; the median age is 42 years. -

North Rhine-Westphalia for H1 2019
MARKET REPORT ON THE LETTING OF LOGISTICS PROPERTIES AND INDUSTRIAL SPACES North Rhine-Westphalia for H1 2019 Market report on the letting of logistics properties and industrial sites in North Rhine-Westphalia* for first half of 2019 n Take-up in NRW sees impressive year-on-year >> Take-up of logistics properties and industrial spaces in North Rhine-Westphalia H1 2019 growth of 22% to around 517,000 sqm n Ruhr region delivers the highest take-up at +88% year-on-year n Logistics, retail and industrial companies in the Cologne and Düsseldorf sub-markets wait in line n New construction activity stalls n Rents relatively stable n Average rent in Cologne climbs by 10% >> Take-up of logistic property and industrial space by regions in North Rhine-Westphalia H1 2019 n Forecast for full-year 2019: solid take-up of between 850,000 and 930,000 sqm The logistics market in North Rhine-Westphalia (NRW) has enjoyed excellent performance once again. With a letting volume of around 517,000 sqm for industrial and logistics space and business parks, one of Germany’s most im- portant logistics markets recorded impressive year-on-year growth of 22% compared with the prior-year figure of 422,200 sqm and achieved its third-best result in the last five years, coming in at 3% above the five-year average (501,600 sqm). >> Lessors with the highest take-up in H1 2019 in the metropolitan region Düsseldorf The Ruhr region rescued the overall picture for 1. Amazon, Kempen, 3. ABC, Düsseldorf NRW, recording the highest level of demand as 22,370 sqm, new building 13,500 sqm, built-to-suit well as the most leases concluded thanks to quick follow-up letting in functional existing buildings. -

Experiences from Structural Change in the Ruhr Area ISBN 978-3-946211-21-1
JUST TRANSITION FOR REGIONS AND GENERATIONS Experiences from structural change in the Ruhr area ISBN 978-3-946211-21-1 JUST TRANSITION FOR REGIONS AND GENERATIONS Experiences from structural change in the Ruhr area Research study conducted on behalf of WWF Germany by Imprint Published by WWF Germany, Berlin Date January 2019 Authors Elke Dahlbeck, Dr. Stefan Gärtner (Institut für Arbeit und Technik) Coordination Juliette de Grandpré ( WWF Germany) Contact [email protected] Editor Thomas Köberich (WWF Germany) Design Anna Risch ([email protected]) The European Climate Initiative (EUKI) is a project financing instrument by the German Federal Ministry for the Environment, Nature Conserva- tion and Nuclear Safety (BMU). Its implementation is supported by the Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH. It is the overarching goal of the EUKI to foster climate cooperation within the European Union (EU) in order to mitigate greenhouse gas emissions. The opinions put forward in this publication are the sole responsibility of the author and do not necessarily reflect the views of the Federal Ministry for the Environment, Nature Conservation and Nuclear Safety. © 2019 WWF Germany · No reprint of the report or extracts thereof without the publisher’s permission. Worldwide, it has become clear that Foreword global warming is the greatest eco- logical and social challenge of our time. Achieving the climate targets are part of a bigger scheme: a global transition in Germany and Europe towards a society that no longer relies on fossil fuels. This transition is the only possible response to the climate crisis, and in its magnitude and significance comparable to such major historical upheavals as industrialisation or digitalisation. -

Foreign Companies in the Rhineland
As at: September 2013 Foreign companies in the Rhineland ObjEctiVE | SOurcES This survey is designed to show that the Rhineland is truly international due to the large number of foreign companies that are members of the Chambers of Commerce and Industry, which are collaborating in the „Rheinland Initiative“, in this case the Chambers of Aachen, Bonn/Rhein-Sieg, Düsseldorf, Köln, Mittlerer Niederrhein and Wuppertal-Solingen-Remscheid. The foreign companies associated with the Chambers of Commerce and Industry are made up of foreign companies registered in the official commercial register and other small foreign owned businesses. The “Initiative Rheinland” aims to secure and improve the position of the Rhineland as one of the most attractive business destinations in Europe. MARKUS database of Creditreform AG, Neuss, Germany, 2013 Databases of members maintained by Chambers of Commerce and Industry in the Rhineland, Germany, 2013 Ausländische Bevölkerung in Nordrhein-Westfalen am 31. Dezember 2011 Landesbetrieb Information und Technik Nordrhein-Westfalen (IT.NRW), statistics division, Düsseldorf, Germany, 2011 Konjunkturbarometer Rheinland Jahresbeginn 2013 Chambers of Commerce and Industry in the Rhineland, Aachen, Germany, 2013 All the information provided in this brochure has been collated and drafted with the utmost care. The Chamber of Commerce and Industry Mittlerer Niederrhein does not provide any guarantees in respect of the accuracy and completeness of the content nor is it liable for any interim changes. Reprints, including extracts, -

Grzentr Brosch Umschl E.Qxd:Layout 1 06.09.2007 13:04 Uhr Seite 1
GrZentr_Brosch_Umschl_E.qxd:Layout 1 06.09.2007 13:04 Uhr Seite 1 Cultural Industries in Creative Industries: Activities in Aachen – Innovative Support of the Aachen Region – a empirical outlook on The GründerZentrum Cultural Industries – Hotspot of Innovation Europe Kulturwirtschaft e.V. The “New” of in North Rhine-West- the Aachen Model phalia and Europe CREATIVE INDUSTRIES IN AACHEN POTENTIALS OF A TOWN GrZentr_Brosch_Umschl_E.qxd:Layout 1 06.09.2007 13:04 Uhr Seite 2 GrZentr_Brosch_3008_E.qxd:Layout 1 06.09.2007 13:04 Uhr Seite 1 1 FOREWORD The municipality of Aachen was early engaged in the potentials of the Cultural Industries in Aachen, namely not only with respect to the variously quoted “soft location factors”, but rather regarding the Cultural Industries as an autonomous economic factor and innovation driver for other branches. First studies in the recent past have shown that there is a growth potential as to business start-ups in the Aachen area. The economic region of Aachen is in an advantageous situation compared to other locations – innovation potential from university and research institutions as well as the marginality towards neighbouring countries allowed the presumption of development prospects. A consequence of this knowledge was the opening of a centre for founders of a new business deriving from the Cultural Industries in Aachen in June 2004, which – using a trendsetting consultancy programme – within short has established itself facing the persons engaged in the cultural sector in and around Aachen and which in the meantime is attracting supra-regional and international attention as best practice example. 381 primary contacts, 259 initial consultancies and 67 participants in the pilot project “KULTURunternehmen” within the first two years of the existence of the GründerZentrum Kulturwirtschaft e.V. -

Study (Gemeinde Gangelt) Prof. Dr. Hendrik Streeck (Inst
Vorläufiges Ergebnis und Schlussfolgerungen der COVID-19 Case-Cluster- Study (Gemeinde Gangelt) Prof. Dr. Hendrik Streeck (Institut für Virologie) Prof. Dr. Gunther Hartmann (Institut für Klinische Chemie und Klinische Pharmakologie, Sprecher Exzellenzcluster ImmunoSensation2) Prof. Dr. Martin Exner (Institut für Hygiene und öffentliche Gesundheit) Prof. Dr. Matthias Schmid (Institut für Medizinische Biometrie, Informatik und Epidemiologie) Universitätsklinikum Bonn, Bonn, den 9. April 2020 Hintergrund: Die Gemeinde Gangelt ist in Deutschland einer der am stärksten von COVID19 betroffenen Orte Deutschlands. Es wird angenommen, dass das Infektionsgeschehen auf eine Karnevalssitzung am 15. Februar 2020 zurückzuführen ist, da mehrere Personen im Nachgang zu dieser Sitzung SARSCoV2 positiv getestet wurden. Die Karnevalssitzung und das Ausbruchgeschehen der Sitzung wird derzeit noch genauer untersucht. Es wurde eine repräsentative Stichprobe aus der Gemeinde Gangelt (12.529 Einwohner) im Kreis Heinsberg gezogen. Die Weltgesundheitsorganisation (WHO) empfiehlt ein Protokoll, bei dem je nach zu erwartender Prävalenz stichprobenartig 100 bis 300 Haushalte untersucht werden. Diese Stichprobe wurde auf ihre Repräsentativität abgestimmt mit Herrn Prof. Manfred Güllner (Forsa). Ziel: Das Ziel der Studie ist es, den Stand der durchgemachten und noch immer stattfindenden SARS-CoV2 Infektionen (Prozentsatz aller Infizierten) in der Gemeinde Gangelt zu bestimmen. Zusätzlich soll damit der Stand der derzeitigen SARS-CoV2 Immunität ermittelt werden. Vorgehen: Ein Serienbrief wurde an ca. 600 Haushalte verschickt. Insgesamt nahmen ca. 1000 Einwohner aus ca. 400 Haushalten an der Studie teil. Es wurden Fragebögen erhoben, Rachenabstriche genommen und Blut auf das Vorliegen von Antikörper (IgG, IgA) getestet. In diese erste Auswertung gehen die Zwischenergebnisse und Rückschlüsse von ca. 500 Personen ein. Vorläufiges Ergebnis: Es wurde eine bestehende Immunität von ca.