Steroid Therapy for Nasal Polyp: Compliance Due to Cost and Phobia in Developing Countries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nasal Polyposis, Eosinophil Dominated Inflammation, and Allergy
Thorax 2000;55 (Suppl 2):S79–S83 S79 Nasal polyposis, eosinophil dominated Thorax: first published as 10.1136/thorax.55.suppl_2.S79 on 1 October 2000. Downloaded from inflammation, and allergy Niels Mygind, Ronald Dahl, Claus Bachert A polyp is an oedematous mucous membrane computed tomographic (CT) scanning). The which forms a pedunculating process with a overall prevalence rate is probably about slim or broad stalk or base. Nasal polyps origi- 2–4%5–7 which increases with age of the study nate in the upper part of the nose around the population. Nasal polyposis occurs with a high openings to the ethmoidal sinuses. The polyps frequency in groups of patients with specified extend into the nasal cavity from the middle airway diseases (table 1). meatus, resulting in nasal blockage and re- Although symptomatic nasal polyposis is stricted airflow to the olfactory region. The rare in the general population, much higher polyp stroma is highly oedematous with a vary- figures for the occurrence of isolated nasal ing density of inflammatory cells. Nasal polyps have been obtained from necropsy polyposis, consisting of recurrent, multiple studies. A thorough endoscopic examination of polyps, is part of an inflammatory reaction removed nasoethmoidal blocks and endoscopic involving the mucous membrane of the nose, examination of unselected necropsy specimens paranasal sinuses, and often the lower airways. have shown polyps in as many as 25–40% of The polyps are easily accessible for immuno- specimens.89 logical and histological studies and an increas- Allergic rhinitis has a high prevalence rate of ing number of publications have appeared in about 15–20%.10 Most cases in the western recent years, including two monographs.12 world are caused by pollen allergy, having a Nasal polyps have long been associated with seasonal occurrence. -

Nasal Polyposis: a Review
Global Journal of Otolaryngology ISSN 2474-7556 Review Article Glob J Otolaryngol - Volume 8 Issue 2 May 2017 Copyright © All rights are reserved by Sushna Maharjan DOI: 10.19080/GJO.2017.0 Nasal Polyposis: A Review Sushna Maharjan1*, Puja Neopane2, Mamata Tiwari1 and Ramesh Parajuli3 1Department of Pathology, Chitwan Medical College Teaching Hospital, Nepal 2Department of Oral Medicine and Pathology, Health Sciences University of Hokkaido, Japan 3Department of Department of Otorhinolaryngology, Chitwan Medical College Teaching Hospital, Nepal Submission: May 07, 2017; Published: May 30, 2017 *Corresponding author: Sushna Maharjan, Department of Pathology, Chitwan Medical College Teaching Hospital (CMC-TH), P.O. Box 42, Bharatpur, Chitwan, Nepal, Email: Abstract Nasal polyp is a benign lesion that arises from the mucosa of the nasal sinuses or from the mucosa of the nasal cavity as a macroscopic usuallyedematous present mass. with The nasalexact obstruction,etiology is still rhinorrhea unknown and and postnasalcontroversial, drip. but Magnetic it is assumed resonance that imagingmain causes is suggested, are inflammatory particularly conditions to rule andout allergy. It is more common in allergic patients with asthma. Interleukin-5 has found to be significantly raised in nasal polyps. The patients seriousKeywords: conditions Allergy; such Interleukin-5; as neoplasia. Nasal Histopathological polyp; Neoplasia examination is also suggested to rule out malignancy and for definite diagnosis. Abbreviations: M:F- Male: Female; IgE: Immunoglobulin E; IL: Interleukin; CRS: Chronic Rhinosinusitis; HLA: Human Leucocyte Antigen; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging Introduction the nose and nasal sinuses characterized by stromal edema and Nasal polyps are characterized by benign lesions that arise from the mucosa of the nasal sinuses, most often from the cause may be different. -

New Medical Treatments for Nasal Polyps
New Medical Treatments for Nasal Polyps February 7, 2020 Brian Modena, MD, MSc 1 Disclosures Research support: NHLBI‐Supported Researcher Self Care Catalysts: architect of Health StorylinesTM app Personal Fees: AstraZeneca, GSK, Regeneron, Sanofi 42nd Annual Pulmonary and Allergy Update Objectives 1. Discuss the epidemiology, biology, pathophysiology, and symptoms of CRS with nasal polyposis (CRSwNP). 2. Review treatment guidelines and recommendations for CRSwNP. 3. Review the many scoring systems used to evaluate CRSwNP. 4. Discuss in detail the Phase II and Phase III clinical trials using biologics for treatment of CRSwNP. Nasal Polyposis Epidemiology Prevalence = ~4%1; (CRS = ~11‐12%)2 Costs: Genetic inheritance = ~14% 2 Increases with age; peak ~50 years CRS = ~$8 billion/year Caucasians = Th2‐driven inflammation. Per patient per year: $13,000; Male to female = 2:1 $26,000 if surgery performed. Asians = Th1‐driven inflammation. Association with allergic rhinitis is weak. Surgeries/year = ~500,000 Disease Prevalence estimates 1. Hastan, Fokkens, et al, 2011 Allergic rhinitis Adult: 0.1%; Children 1.5%1 2. Lange, Holst, et al., Clin Otolaryngol 2013. 3. Mygind. JACI. 1990 Dec;86(6 Pt 1):827‐9. Asthma 5‐22% 4. Schleimer RP. Annu Rev Pathol. 2017;12:331‐57. 5. Hunter TD, DeConde AS, Manes RP. J Med Econ. 2018;21(6):610‐5. CRS 20‐25%1‐4 6. Palmer JN, Messina JC, Biletch R, et al. Allergy Asthma Proc. 2018;39:1‐9. NSAID intolerance 36‐72% 7. Pearlman AN, Chandra RK, Chang D, et al. Am J Rhinol Allergy. 2009;23(2):145‐8. NSAID intolerance and asthma 80% 8. -

Highlights of Prescribing Information
HIGHLIGHTS OF PRESCRIBING INFORMATION • Gastrointestinal Perforation: Increased risk in patients with certain GI These highlights do not include all the information needed to use disorders; Signs and symptoms may be masked (5.4) ® EMFLAZA safely and effectively. See full prescribing information for • Behavioral and Mood Disturbances: May include euphoria, insomnia, EMFLAZA. mood swings, personality changes, severe depression, and psychosis (5.5) • Effects on Bones: Monitor for decreases in bone mineral density with EMFLAZA® (deflazacort) tablets, for oral use EMFLAZA® (deflazacort) oral suspension chronic use of EMFLAZA (5.6) Initial U.S. Approval: 2017 • Ophthalmic Effects: May include cataracts, infections, and glaucoma; Monitor intraocular pressure if EMFLAZA is continued for more than 6 ---------------------------INDICATIONS AND USAGE--------------------------- weeks (5.7) EMFLAZA is a corticosteroid indicated for the treatment of Duchenne muscular dystrophy (DMD) in patients 2 years of age and older (1) • Vaccination: Do not administer live or live attenuated vaccines to patients receiving immunosuppressive doses of corticosteroids. Administer live- ----------------------DOSAGE AND ADMINISTRATION---------------------- attenuated or live vaccines at least 4 to 6 weeks prior to starting • The recommended once-daily dosage is approximately 0.9 mg/kg/day EMFLAZA (5.8) administered orally (2.2) • Serious Skin Rashes: Discontinue at the first sign of rash, unless the rash is • Discontinue gradually when administered for more than a few -

Comparative Effects of Anti-Inflammatory Corticosteroids in Human Bone-Derived Osteoblast-Like Cells
Copyright ©ERS Journals Ltd 1998 Eur Respir J 1998; 12: 1327–1333 European Respiratory Journal DOI: 10.1183/09031936.98.12061327 ISSN 0903 - 1936 Printed in UK - all rights reserved Comparative effects of anti-inflammatory corticosteroids in human bone-derived osteoblast-like cells H. Namkung-Matthäi*, J.P. Seale**, K. Brown***, R.S. Mason* aa Comparative effects of anti-inflammatory corticosteroids in human bone-derived osteo- Depts of *Physiology and Institute for blast- like cells. H. Namkung-Matthäi, J.P. Seale, K. Brown, R.S. Mason. ©ERS Journals Ltd Biomedical Research, **Pharmacology and 1998. ***Pharmacy, University of Sydney, Aus- ABSTRACT: While effects of inhaled corticosteroids on serum markers of bone tralia. metabolism in normal and asthmatic subjects have been reported, there are little data Correspondence: R.S. Mason on the direct effects of these corticosteroids on end-organs such as bone. The results Dept of Physiology and Institute for Bio- presented here compare the effects of budesonide and its epimers (22S- and 22R- medical Research budesonide), fluticasone and dexamethasone on growth and differentiation of cul- University of Sydney tured human bone cells. NSW 2006 Osteoblast-like cells were cultured from human foetal bone chips grown to conflu- Australia ence and used at first subculture. Fax: 61 293512058 At concentrations of 10-11–10-7 M each corticosteroid (CS) caused a dose-dependent Keywords: Alkaline phosphatase decrease in [3H]thymidine incorporation into deoxyribonucleic acid (DNA), median bioactivity effective concentration (EC50): fluticasone (0.06 nM) >22R (0.26 nM) >22S (0.4 nM) bone-derived cells >budesonide (0.47 nM) >dexamethasone (1.5 nM). -

MSM Chapter 1200 3/1/21
MEDICAID SERVICES MANUAL TRANSMITTAL LETTER February 23, 2021 TO: CUSTODIANS OF MEDICAID SERVICES MANUAL FROM: JESSICA KEMMERER, HIPAA PRIVACY AND CIVIL RIGHTS OFFICER /Jessica Kemmerer/ BACKGROUND AND EXPLANATION The DHCFP is proposing revisions to Medicaid Services Manual (MSM), Chapter 1200 – Prescribed Drugs, Appendix A, to reflect recommendations approved on October 22, 2020, by the Drug Use Review (DUR) Board. The proposed changes include the addition of new prior authorization criteria for Doxepine Topical, the addition of new prior authorization criteria for Zeposia® (ozanimod), addition of new prior authorization for Evenity® (romosozumab-aqqg), Prolia® (denosumab), Forteo® (teriparatide) and Tymlos® (abaloparatide) within a new combined osteoporosis agents section, and addition of new prior authorization criteria for Orilissa® (elagolix) and Oriahnn® (elagolix, estradiol, and norethindrone) within a new Gonadorpin Hormone Receptor (GnRH) Antagonist and Combinations section. Additionally, the DHCFP is proposing revisions to the existing prior authorization criteria for psychotropic medications for children and adolescents, and revision to the existing clinical criteria for Epidiolex® (cannabidiol). Throughout the chapter, grammar, punctuation and capitalization changes were made, duplications removed, acronyms used and standardized, and language reworded for clarity. Renumbering and re- arranging of sections was necessary. These changes are effective March 1, 2021. MATERIAL TRANSMITTED MATERIAL SUPERSEDED MTL N/A MTL N/A MSM Ch 1200 – Prescribed Drugs MSM Ch 1200 – Prescribed Drugs Background and Explanation of Policy Changes, Manual Section Section Title Clarifications and Updates Appendix A Psychotropic Added new policy language criteria on which specific Section N Medications for drug classes may bypass polypharmacy clinical criteria. Children and Adolescents Appendix A Reserved for Future Created a new section titled “Doxepin Topical.” Added Section W Use new prior authorization criteria for doxepin topical. -

Surgical Management of Polyps in the Treatment of Nasal Airway
Surgical Management of Polyps in the TreatmentofNasal Airway Obstruction Samuel S. Becker, MD KEYWORDS FESS Nasal polyps Sinonasal polyps Polyp treatment Nasal obstruction In addition to their role in chronic rhinosinusitis and nasal congestion, sinonasal polyps are associated with significant nasal obstruction. Via a purely mechanical effect (ie, obstruction at its simplest level), polyps alter and otherwise block the normal flow of air through the nose. Similarly, by blocking the drainage pathways of the paranasal sinuses, sinus inflammation and its associated symptom of congestion occur. Because the pathway that leads to the formation of sinonasal polyps has not been completely elucidated, effective long-term treatments remain difficult to pinpoint. Management of these polyps, therefore, is a difficult challenge for the contemporary otolaryngologist. Some of the more common medical treatment options include: topical and oral steroids; macrolide antibiotics; diuretic nasal washes; and intrapolyp steroid injection. Surgical options include polypectomy and functional endoscopic sinus surgery (FESS). In addition, novel treatments for polyps are introduced with some frequency. This article presents an overview of management options for sino- nasal polyps, focusing on the indications, efficacy, and complications of the more common interventions. DIAGNOSIS AND PREVALENCE OF SINONASAL POLYPS Diagnosis of sinonasal polyps relies primarily on nasal endoscopy, with computed tomography (CT) to evaluate the extent of disease. Although unilateral -

Statistical Analysis Plan
Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version V1.4 Date 14 July 2017 Decline In lung-function Among Patients with chronic obstructive Lung disease On maintenance therapy (DIAPLO) An observational study evaluating the benefits of early intervention with maintenance therapies to prevent or slow down rapid lung function decline in patients who are at high risk at the time of COPD diagnosis in the combined Optimum Patient Care Research Database and Clinical Practice Research Datalink databases TITLE PAGE Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version 14 July 2017 Date 14 July 2017 TABLE OF CONTENTS PAGE TITLE PAGE ........................................................................................................... 1 TABLE OF CONTENTS ......................................................................................... 2 LIST OF ABBREVIATIONS .................................................................................. 5 RESPONSIBLE PARTIES ...................................................................................... 6 PROTOCOL SYNOPSIS DIAPLO STUDY ........................................................... 7 AMENDMENT HISTORY ................................................................................... 12 MILESTONES ....................................................................................................... 13 1. BACKGROUND AND RATIONALE .................................................................. 14 1.1 Background ........................................................................................................... -
Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer
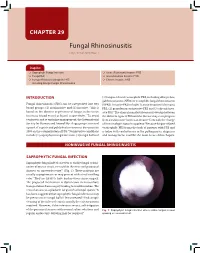
CHAPTER 29 Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer Snapshot Saprophytic Fungal Infection Acute (Fulminant) Invasive FRS Fungal Ball Granulomatous Invasive FRS Fungus-Related Eosinophilic FRS Chronic Invasive FRS Including Allergic Fungal Rhinosinusitis INTRODUCTION (3) fungus-related eosinophilic FRS, including allergic fun- gal rhinosinusitis (AFRS) or eosinphilic fungal rhinosinusitis Fungal rhinosinusitis (FRS) can be categorized into two (EFRS). Invasive FRS include (1) acute invasive (fulminant) 1 broad groups: (1) noninvasive and (2) invasive. This is FRS, (2) granulomatous invasive FRS and (3) chronic inva- based on the absence or presence of fungus in the tissue sive FRS.3 The clinical manifestations may overlap between (mucosa, blood vessel or bone) respectively.2 To avoid the different types of FRS and the disease may even progress confusion and to optimize management, the International from a noninvasive form to an invasive form with the change Society for Human and Animal Mycology group convened of immunologic status in a patient.4 Because fungus-related a panel of experts and published a consensus document in eosinophilic FRS forms the bulk of patients with FRS and 2009 on the categorization of FRS.3 Noninvasive conditions is laden with controversies in the pathogenesis, diagnosis include (1) saprophytic fungal infection, (2) fungal ball and and management, it will be the main focus of this chapter. NONINVASIVE FUNGAL RHINOSINUSITIS SAPROPHYTIC FUNGAL INFECTION Saprophytic fungal infection refers to visible fungal coloni- zation of mucus crusts seen within the nose and paranasal sinuses on nasoendoscopy3,4 (Fig. 1). These patients are usually asymptomatic or may present with a foul smelling odor.2 They are likely to have had previous sinus surgery. -

With Deflazacort
Annals of the Rheumatic Diseases 1994; 53: 331-333 331 Long term treatment of polymyalgia rheumatica Ann Rheum Dis: first published as 10.1136/ard.53.5.331 on 1 May 1994. Downloaded from with deflazacort Marco A Cimmino, Gianluigi Moggiana, Carlomaurizio Montecucco, Roberto Caporali, Silvano Accardo Abstract most common starting doses were 15 mg/day Objectives-To evaluate the long term (15 patients, 37 5%), 30 mg/day (14 patients, efficacy and tolerability of deflazacort, a 35%), and 6 mg/day (four patients, 10%). The corticosteroid reputed to have only minor highest dose (60 mg) was used in two patients side effects, in the treatment of poly- with concomitant giant cell arteritis. Patients myalgia rheumatica (PMR). were evaluated monthly for one year and every Methods-In a prospective open study, six months thereafter. Deflazacort was tapered deflazacort was administered at an by about 20% if the patient was asymptomatic average initial dose of 21-8 mg/day for a and ESR was reduced. Side effects were mean period of 19 months in 40 patients searched with a questionnaire and by physical with PMR. examination. Results-A highly significant improve- In PMR recurrences (defined as signs or ment of clinical and laboratory param- symptoms of PMR and/or giant cell arteritis eters occurred one month after therapy requiring higher doses of steroids), deflazacort onset. This improvement persisted for the was increased to the latest level that had whole study period. Laboratory param- kept the patient asymptomatic. A relapse eters of tolerability did not change during was defined as signs or symptoms of PMR the study. -
Multiple Corticosteroids Allergy in a Patient with Asthma: a Case Report
Mahadi et al. The Egyptian Journal of Internal Medicine (2020) 32:4 The Egyptian Journal of https://doi.org/10.1186/s43162-020-00008-x Internal Medicine CASE REPORT Open Access Multiple corticosteroids allergy in a patient with asthma: a case report Mahrunissa Mahadi1, Wan Syazween Lyana Wan Ahmad Kammal2* , Norazirah Md Nor1 and Adawiyah Jamil1 Abstract Background: Allergy towards systemic corticosteroid is rare. This case report discusses the investigations to confirm diagnosis and alternative treatments. Case presentation: A 51-year-old asthmatic woman developed severe anaphylactic reaction following administration of systemic hydrocortisone. Skin prick, intradermal, and intravenous provocation tests confirmed allergy to triamcinolone, hydrocortisone, and dexamethasone. Skin prick tests (SPTs) were negative to all the aforementioned drugs. Intradermal test (IDT) with triamcinolone 1:10 concentration resulted in a 2-mm wheal associated with rhonchi. IDT with hydrocortisone 1:10 concentration showed an 8-mm wheal with rhonchi. IDTs to dexamethasone and carboxymethylcellulose were negative. Generalized rhonchi were observed with intravenous dexamethasone full concentration challenge. Conclusions: Corticosteroid allergy should be suspected in asthma patients with worsening bronchospasm after its administration. Due to its rarity, such diagnosis can easily be missed, resulting in increased morbidity and mortality in patients. Keywords: Glucocorticoid, Drug hypersensitivity, Skin tests, Asthma Key messages Corticosteroid allergy occurs with various administration Corticosteroid allergy is rare. It should be suspected in routes including intravenous, oral, inhaled, intramuscular, asthmatic patients with worsening bronchospasm after intra-articular, ocular, intralesional, and topical applications steroid administration. Allergic skin tests are useful to [4]. Type IV hypersensitivity reaction in the form of allergic identify the allergen and suitable alternatives. -

Upper Airway Findings and Markers of Lung Disease Progression in Patients with Cystic Fibrosis
Published online: 2020-03-11 THIEME 434 Original Research Upper Airway Findings and Markers of Lung Disease Progression in Patients with Cystic Fibrosis Luciane Mazzini Steffen1 Luise Sgarabotto Pezzin1 Natassia Sulis2 Nedio Steffen1 Leonardo Araujo Pinto3 1 Department of Otorhinolaringology, Pontifícia Universidade Address for correspondence Luise Sgarabotto Pezzin, MD, CatólicadoRioGrandedoSul,PortoAlegre,RS,Brazil Department of Otorhinolaringology, Pontifícia Universidade Católica 2 Department of Pediatrics, Pontifícia Universidade Católica do Rio do Rio Grande do Sul, Porto Alegre, RS, 90619900, Brazil Grande do Sul, Porto Alegre, RS, Brazil (e-mail: [email protected]). 3 Department of Pediatric Pneumology, Pontifícia Universidade CatólicadoRioGrandedoSul,PortoAlegre,RS,Brazil Int Arch Otorhinolaryngol 2020;24(4):e434–e437. Abstract Introduction Cystic fibrosis (CF) is a genetic disease that limits the quality of life mainly due to respiratory symptoms. The relationship between findings of the upper airways and CF lung disease is not yet completely understood. Objective The aim of the present study is to describe the most frequent nasal findings and pathogens in patients with CF and investigate the association between the findings of the upper respiratory tract and markers of lung disease progression. Methods Retrospective study in patients with CF from the Pediatric Pulmonology Department who underwent otorhinolaryngological evaluation between 2015 and 2017. Nasal endoscopy and nasal swab collection were part of the evaluation. The severity markers used were: percentage of predicted forced expiratory volume in the first second (FEV1%), body mass index (BMI) and the Shwachman-Kulczycki (SK) clinical score. Results A total of 48 patients with CF were included. The mean of the predicted percentage of FEV1% was 83.36 Æ 30.04.