Role of C. Pneumoniae in Nasal Polyp Formation: PCR in Tissue And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nasal Polyposis, Eosinophil Dominated Inflammation, and Allergy
Thorax 2000;55 (Suppl 2):S79–S83 S79 Nasal polyposis, eosinophil dominated Thorax: first published as 10.1136/thorax.55.suppl_2.S79 on 1 October 2000. Downloaded from inflammation, and allergy Niels Mygind, Ronald Dahl, Claus Bachert A polyp is an oedematous mucous membrane computed tomographic (CT) scanning). The which forms a pedunculating process with a overall prevalence rate is probably about slim or broad stalk or base. Nasal polyps origi- 2–4%5–7 which increases with age of the study nate in the upper part of the nose around the population. Nasal polyposis occurs with a high openings to the ethmoidal sinuses. The polyps frequency in groups of patients with specified extend into the nasal cavity from the middle airway diseases (table 1). meatus, resulting in nasal blockage and re- Although symptomatic nasal polyposis is stricted airflow to the olfactory region. The rare in the general population, much higher polyp stroma is highly oedematous with a vary- figures for the occurrence of isolated nasal ing density of inflammatory cells. Nasal polyps have been obtained from necropsy polyposis, consisting of recurrent, multiple studies. A thorough endoscopic examination of polyps, is part of an inflammatory reaction removed nasoethmoidal blocks and endoscopic involving the mucous membrane of the nose, examination of unselected necropsy specimens paranasal sinuses, and often the lower airways. have shown polyps in as many as 25–40% of The polyps are easily accessible for immuno- specimens.89 logical and histological studies and an increas- Allergic rhinitis has a high prevalence rate of ing number of publications have appeared in about 15–20%.10 Most cases in the western recent years, including two monographs.12 world are caused by pollen allergy, having a Nasal polyps have long been associated with seasonal occurrence. -

Nasal Polyposis: a Review
Global Journal of Otolaryngology ISSN 2474-7556 Review Article Glob J Otolaryngol - Volume 8 Issue 2 May 2017 Copyright © All rights are reserved by Sushna Maharjan DOI: 10.19080/GJO.2017.0 Nasal Polyposis: A Review Sushna Maharjan1*, Puja Neopane2, Mamata Tiwari1 and Ramesh Parajuli3 1Department of Pathology, Chitwan Medical College Teaching Hospital, Nepal 2Department of Oral Medicine and Pathology, Health Sciences University of Hokkaido, Japan 3Department of Department of Otorhinolaryngology, Chitwan Medical College Teaching Hospital, Nepal Submission: May 07, 2017; Published: May 30, 2017 *Corresponding author: Sushna Maharjan, Department of Pathology, Chitwan Medical College Teaching Hospital (CMC-TH), P.O. Box 42, Bharatpur, Chitwan, Nepal, Email: Abstract Nasal polyp is a benign lesion that arises from the mucosa of the nasal sinuses or from the mucosa of the nasal cavity as a macroscopic usuallyedematous present mass. with The nasalexact obstruction,etiology is still rhinorrhea unknown and and postnasalcontroversial, drip. but Magnetic it is assumed resonance that imagingmain causes is suggested, are inflammatory particularly conditions to rule andout allergy. It is more common in allergic patients with asthma. Interleukin-5 has found to be significantly raised in nasal polyps. The patients seriousKeywords: conditions Allergy; such Interleukin-5; as neoplasia. Nasal Histopathological polyp; Neoplasia examination is also suggested to rule out malignancy and for definite diagnosis. Abbreviations: M:F- Male: Female; IgE: Immunoglobulin E; IL: Interleukin; CRS: Chronic Rhinosinusitis; HLA: Human Leucocyte Antigen; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging Introduction the nose and nasal sinuses characterized by stromal edema and Nasal polyps are characterized by benign lesions that arise from the mucosa of the nasal sinuses, most often from the cause may be different. -

New Medical Treatments for Nasal Polyps
New Medical Treatments for Nasal Polyps February 7, 2020 Brian Modena, MD, MSc 1 Disclosures Research support: NHLBI‐Supported Researcher Self Care Catalysts: architect of Health StorylinesTM app Personal Fees: AstraZeneca, GSK, Regeneron, Sanofi 42nd Annual Pulmonary and Allergy Update Objectives 1. Discuss the epidemiology, biology, pathophysiology, and symptoms of CRS with nasal polyposis (CRSwNP). 2. Review treatment guidelines and recommendations for CRSwNP. 3. Review the many scoring systems used to evaluate CRSwNP. 4. Discuss in detail the Phase II and Phase III clinical trials using biologics for treatment of CRSwNP. Nasal Polyposis Epidemiology Prevalence = ~4%1; (CRS = ~11‐12%)2 Costs: Genetic inheritance = ~14% 2 Increases with age; peak ~50 years CRS = ~$8 billion/year Caucasians = Th2‐driven inflammation. Per patient per year: $13,000; Male to female = 2:1 $26,000 if surgery performed. Asians = Th1‐driven inflammation. Association with allergic rhinitis is weak. Surgeries/year = ~500,000 Disease Prevalence estimates 1. Hastan, Fokkens, et al, 2011 Allergic rhinitis Adult: 0.1%; Children 1.5%1 2. Lange, Holst, et al., Clin Otolaryngol 2013. 3. Mygind. JACI. 1990 Dec;86(6 Pt 1):827‐9. Asthma 5‐22% 4. Schleimer RP. Annu Rev Pathol. 2017;12:331‐57. 5. Hunter TD, DeConde AS, Manes RP. J Med Econ. 2018;21(6):610‐5. CRS 20‐25%1‐4 6. Palmer JN, Messina JC, Biletch R, et al. Allergy Asthma Proc. 2018;39:1‐9. NSAID intolerance 36‐72% 7. Pearlman AN, Chandra RK, Chang D, et al. Am J Rhinol Allergy. 2009;23(2):145‐8. NSAID intolerance and asthma 80% 8. -

Surgical Management of Polyps in the Treatment of Nasal Airway
Surgical Management of Polyps in the TreatmentofNasal Airway Obstruction Samuel S. Becker, MD KEYWORDS FESS Nasal polyps Sinonasal polyps Polyp treatment Nasal obstruction In addition to their role in chronic rhinosinusitis and nasal congestion, sinonasal polyps are associated with significant nasal obstruction. Via a purely mechanical effect (ie, obstruction at its simplest level), polyps alter and otherwise block the normal flow of air through the nose. Similarly, by blocking the drainage pathways of the paranasal sinuses, sinus inflammation and its associated symptom of congestion occur. Because the pathway that leads to the formation of sinonasal polyps has not been completely elucidated, effective long-term treatments remain difficult to pinpoint. Management of these polyps, therefore, is a difficult challenge for the contemporary otolaryngologist. Some of the more common medical treatment options include: topical and oral steroids; macrolide antibiotics; diuretic nasal washes; and intrapolyp steroid injection. Surgical options include polypectomy and functional endoscopic sinus surgery (FESS). In addition, novel treatments for polyps are introduced with some frequency. This article presents an overview of management options for sino- nasal polyps, focusing on the indications, efficacy, and complications of the more common interventions. DIAGNOSIS AND PREVALENCE OF SINONASAL POLYPS Diagnosis of sinonasal polyps relies primarily on nasal endoscopy, with computed tomography (CT) to evaluate the extent of disease. Although unilateral -

Statistical Analysis Plan
Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version V1.4 Date 14 July 2017 Decline In lung-function Among Patients with chronic obstructive Lung disease On maintenance therapy (DIAPLO) An observational study evaluating the benefits of early intervention with maintenance therapies to prevent or slow down rapid lung function decline in patients who are at high risk at the time of COPD diagnosis in the combined Optimum Patient Care Research Database and Clinical Practice Research Datalink databases TITLE PAGE Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version 14 July 2017 Date 14 July 2017 TABLE OF CONTENTS PAGE TITLE PAGE ........................................................................................................... 1 TABLE OF CONTENTS ......................................................................................... 2 LIST OF ABBREVIATIONS .................................................................................. 5 RESPONSIBLE PARTIES ...................................................................................... 6 PROTOCOL SYNOPSIS DIAPLO STUDY ........................................................... 7 AMENDMENT HISTORY ................................................................................... 12 MILESTONES ....................................................................................................... 13 1. BACKGROUND AND RATIONALE .................................................................. 14 1.1 Background ........................................................................................................... -
Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer
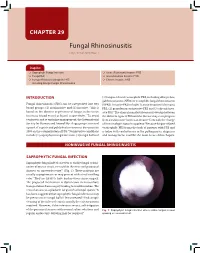
CHAPTER 29 Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer Snapshot Saprophytic Fungal Infection Acute (Fulminant) Invasive FRS Fungal Ball Granulomatous Invasive FRS Fungus-Related Eosinophilic FRS Chronic Invasive FRS Including Allergic Fungal Rhinosinusitis INTRODUCTION (3) fungus-related eosinophilic FRS, including allergic fun- gal rhinosinusitis (AFRS) or eosinphilic fungal rhinosinusitis Fungal rhinosinusitis (FRS) can be categorized into two (EFRS). Invasive FRS include (1) acute invasive (fulminant) 1 broad groups: (1) noninvasive and (2) invasive. This is FRS, (2) granulomatous invasive FRS and (3) chronic inva- based on the absence or presence of fungus in the tissue sive FRS.3 The clinical manifestations may overlap between (mucosa, blood vessel or bone) respectively.2 To avoid the different types of FRS and the disease may even progress confusion and to optimize management, the International from a noninvasive form to an invasive form with the change Society for Human and Animal Mycology group convened of immunologic status in a patient.4 Because fungus-related a panel of experts and published a consensus document in eosinophilic FRS forms the bulk of patients with FRS and 2009 on the categorization of FRS.3 Noninvasive conditions is laden with controversies in the pathogenesis, diagnosis include (1) saprophytic fungal infection, (2) fungal ball and and management, it will be the main focus of this chapter. NONINVASIVE FUNGAL RHINOSINUSITIS SAPROPHYTIC FUNGAL INFECTION Saprophytic fungal infection refers to visible fungal coloni- zation of mucus crusts seen within the nose and paranasal sinuses on nasoendoscopy3,4 (Fig. 1). These patients are usually asymptomatic or may present with a foul smelling odor.2 They are likely to have had previous sinus surgery. -

Upper Airway Findings and Markers of Lung Disease Progression in Patients with Cystic Fibrosis
Published online: 2020-03-11 THIEME 434 Original Research Upper Airway Findings and Markers of Lung Disease Progression in Patients with Cystic Fibrosis Luciane Mazzini Steffen1 Luise Sgarabotto Pezzin1 Natassia Sulis2 Nedio Steffen1 Leonardo Araujo Pinto3 1 Department of Otorhinolaringology, Pontifícia Universidade Address for correspondence Luise Sgarabotto Pezzin, MD, CatólicadoRioGrandedoSul,PortoAlegre,RS,Brazil Department of Otorhinolaringology, Pontifícia Universidade Católica 2 Department of Pediatrics, Pontifícia Universidade Católica do Rio do Rio Grande do Sul, Porto Alegre, RS, 90619900, Brazil Grande do Sul, Porto Alegre, RS, Brazil (e-mail: [email protected]). 3 Department of Pediatric Pneumology, Pontifícia Universidade CatólicadoRioGrandedoSul,PortoAlegre,RS,Brazil Int Arch Otorhinolaryngol 2020;24(4):e434–e437. Abstract Introduction Cystic fibrosis (CF) is a genetic disease that limits the quality of life mainly due to respiratory symptoms. The relationship between findings of the upper airways and CF lung disease is not yet completely understood. Objective The aim of the present study is to describe the most frequent nasal findings and pathogens in patients with CF and investigate the association between the findings of the upper respiratory tract and markers of lung disease progression. Methods Retrospective study in patients with CF from the Pediatric Pulmonology Department who underwent otorhinolaryngological evaluation between 2015 and 2017. Nasal endoscopy and nasal swab collection were part of the evaluation. The severity markers used were: percentage of predicted forced expiratory volume in the first second (FEV1%), body mass index (BMI) and the Shwachman-Kulczycki (SK) clinical score. Results A total of 48 patients with CF were included. The mean of the predicted percentage of FEV1% was 83.36 Æ 30.04. -

Associations Between the Quality of Life and Nasal Polyp Size In
Journal of Clinical Medicine Article Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease Sven Schneider 1 , Nicholas J. Campion 1, Sergio Villazala-Merino 1, David Tianxiang Liu 1 , Tina Bartosik 1, Lukas D. Landegger 1 , Navid Ahmadi 1 , Christian A. Mueller 1, Erich Vyskocil 1, Victoria Stanek 1, Tamara Quint 2, Christine Bangert 2 and Julia Eckl-Dorna 1,* 1 Department of Otorhinolaryngology, Medical University of Vienna, 1090 Vienna, Austria; [email protected] (S.S.); [email protected] (N.J.C.); [email protected] (S.V.-M.); [email protected] (D.T.L.); [email protected] (T.B.); [email protected] (L.D.L.); [email protected] (N.A.); [email protected] (C.A.M.); [email protected] (E.V.); [email protected] (V.S.) 2 Department of Dermatology, Medical University of Vienna, 1090 Vienna, Austria; [email protected] (T.Q.); [email protected] (C.B.) * Correspondence: [email protected]; Tel.: +43-1-40400-34380 Received: 21 February 2020; Accepted: 23 March 2020; Published: 28 March 2020 Abstract: Chronic rhinosinusitis (CRS) is a common disease that substantially impairs the quality of life (QoL). Here, we aimed to assess patients’ QoL in different subtypes of CRS and correlated this with nasal polyp size to improve the clinical understanding of the burden of disease. In this retrospective single-center study, 107 patients with the following diagnoses were analyzed: CRS without nasal polyps (CRSsNP), CRS with nasal polyps (CRSwNP), or aspirin-exacerbated respiratory disease (AERD). -

Eosinophilic Lung Diseases
Eosinophilic Lung Diseases Vincent Cottin, MD, PhDa,b,* KEYWORDS Eosinophil Eosinophilic pneumonia Interstitial lung disease Eosinophilic granulomatosis with polyangiitis Aspergillus KEY POINTS Eosinophilic lung diseases may present as eosinophilic pneumonia with chronic or acute onset, or as the more transient Lo¨ ffler syndrome. The diagnosis of eosinophilic pneumonia is based on both characteristic clinical-imaging features and the demonstration of alveolar eosinophilia of at least 25% eosinophils at bronchoalveolar lavage. Peripheral blood eosinophilia is present in most eosinophilic lung disorders, but can be absent at presentation in idiopathic acute eosinophilic pneumonia and in patients receiving corticosteroid treatment. In Europe and North America, chronic eosinophilic pneumonia is most frequently idiopathic, whereas acute eosinophilic pneumonia is often related to drug or tobacco smoke exposure. All possible causes of eosinophilia (especially fungus or parasitic infection, drug or toxic exposure) must be thoroughly investigated. DEFINITION AND CLASSIFICATION count of greater than 1.5 Â 109 on 2 examinations Definition over at least a 1-month interval.3–5 Alveolar eosin- ophilia is defined by differential cell count of at Eosinophilic lung diseases are a group of diffuse least 25% eosinophils at bronchoalveolar lavage parenchymal lung diseases1,2 characterized by (BAL), and typically greater than 40%.4 the prominent infiltration of the lung interstitium and the alveolar spaces by polymorphonuclear Classification eosinophils, with conservation of the lung archi- tecture. As a corollary, a common denominator Eosinophilic lung disorders can present as acute of eosinophilic lung diseases is represented by a or chronic pneumonia or as the transient Lo¨ ffler dramatic response to systemic corticosteroid ther- syndrome, which is most commonly of parasitic apy and healing without any sequelae in most origin (Box 1). -

Steroid Therapy for Nasal Polyp: Compliance Due to Cost and Phobia in Developing Countries
Journal of Otolaryngology-ENT Research Review Article Open Access Steroid therapy for nasal polyp: compliance due to cost and phobia in developing countries Abstract Volume 10 Issue 6 - 2018 Nasal polyps are among the common conditions encountered by an otolaryngologist in Vadisha Srinivas Bhat routine clinical practice. It is a benign lesion, but can be troublesome due to variety of Department of Otorhinolaryngology, Deemed to be University clinical symptoms. A condition, which can be diagnosed easily by clinical examination K S Hegde Medical Academy, India supported by CT scan of the paranasal sinuses, poses a challenge in the treatment. While surgical clearance with the aid of endoscopic sinus surgery can provide quick Correspondence: Vadisha Srinivas Bhat, Professor, relief from nasal obstruction, it is frequently followed by recurrence. Medical treatment Otorhinolaryngology, K S Hegde Medical Academy, NITTE, with systemic and intranasal steroid is increasingly used with success as reported by Deemed to be University, Mangalore 575018, Karnataka, India, many authors around the world. Steroid has been used as a single modality of therapy Tel +919480174828, Email or as an adjuvant to surgical therapy before and after the surgery. Considering the long duration of treatment required with intranasal steroids, a large proportion of patients Received: July 06, 2018 | Published: November 16, 2018 discontinue the treatment after certain period of usage, due to number factors which include the cost of therapy and phobia of steroids. This is a review about the steroid usage in nasal polyp, with emphasis on the compliance. Keywords: nasal polyp, steroid; phobia, cost, compliance Introduction sinusitis, whereas allergic fungal sinusitis causes multiple bilateral nasal polyps. -

Evaluation of Allergic Fungal Sinusitis Occurrence in Patients with Nasal Polyps
ORIGINAL ARTICLE Evaluation of Allergic Fungal Sinusitis Occurrence in Patients with Nasal Polyps ABDUR REHMAN, FAISAL RAFIQ, ATHAR ADNAN UPPAL* ABSTRACT Aim: To evaluate allergic fungal sinusitis occurrence in patients with nasal polyps. Methods: This was a prospective descriptive study, conducted at ENT Department of Nawaz Sharif Social Security Hospital Multan Road Lahore , from January 2013 to June 2015. A total of 125 patients with nasal polyps were examined and surgery performed followed by histopathology and culture examination of surgical specimens. Results: Allergic fungal sinusitis (AFS) was found in 28/125 (22.4%) nasal polyp patients. In 28 cases of allergic fungal sinusitis, mean age was 30 years. Majority of patients (67.8%) were in the age range 20 – 40 years. Male to female ratio was 1.4:1. Most (53.5%) of AFS patients belonged to lower social class. Concomitant asthma was noted in 06 (21.4%) patients. Conclusion: Allergic fungal sinusitis is common aetiology seen among nasal polyp patients. Slightly more than one fifth of cases with nasal polyp (22.4%) had AFS in this study, While treating chronic rhinosinusitis patients, this disease entity must be kept in mind. AFS was seen to effect mainly young adults and middle aged poor people living in hot humid conditions. Aspergillus was the commonest organism responsible for AFS. Results are good if it is diagnosed early and treated properly. Keywords: Allergic fungal sinusitis (AFS), Nasal polyp, Allergic mucin. INTRODUCTION elevated total and fungus specific IgE Allergic fungal sinusitis is an allergic reaction of the concentration5,10. The involved sinuses contain brown sinonasal mucosa to aerosolized environmental 1 or greenish black material,which has been called fungal allergens in an immunocompetent person . -

Influence of Chronic Sinusitis and Nasal Polyp on the Lower Airway of Subjects Without Lower Airway Diseases
Original Article Allergy Asthma Immunol Res. 2014 July;6(4):310-315. http://dx.doi.org/10.4168/aair.2014.6.4.310 pISSN 2092-7355 • eISSN 2092-7363 Influence of Chronic Sinusitis and Nasal Polyp on the Lower Airway of Subjects Without Lower Airway Diseases Suh-Young Lee,1,2,3 Soon Ho Yoon,4 Woo-Jung Song,1,2 So-Hee Lee,1,2,5 Hye-Ryun Kang,1,2 Sun-Sin Kim,1,2,5 Sang-Heon Cho1,2,5* 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea 2Institute of Allergy and Clinical Immunology, Seoul National University Medical Research Center, Seoul, Korea 3Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea 4Department of Radiology, Seoul National University College of Medicine, Seoul, Korea 5Seoul National University Hospital Healthcare System Gangnam Center, Seoul, Korea This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. Purpose: Upper and lower respiratory tract pathologies are believed to be interrelated; however, the impact of upper airway inflammation on lung function in subjects without lung disease has not been evaluated. This study investigated the association of CT finding suggesting chronic sinusitis and lung function in healthy subjects without lung disease. Methods: This was a retrospective study of prospectively collected data from 284 sub- jects who underwent a pulmonary function test, bronchial provocation test, rhinoscopy, and osteomeatal unit computed tomography offered as a pri- vate health check-up option.