Associations Between the Quality of Life and Nasal Polyp Size In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nasal Polyposis, Eosinophil Dominated Inflammation, and Allergy
Thorax 2000;55 (Suppl 2):S79–S83 S79 Nasal polyposis, eosinophil dominated Thorax: first published as 10.1136/thorax.55.suppl_2.S79 on 1 October 2000. Downloaded from inflammation, and allergy Niels Mygind, Ronald Dahl, Claus Bachert A polyp is an oedematous mucous membrane computed tomographic (CT) scanning). The which forms a pedunculating process with a overall prevalence rate is probably about slim or broad stalk or base. Nasal polyps origi- 2–4%5–7 which increases with age of the study nate in the upper part of the nose around the population. Nasal polyposis occurs with a high openings to the ethmoidal sinuses. The polyps frequency in groups of patients with specified extend into the nasal cavity from the middle airway diseases (table 1). meatus, resulting in nasal blockage and re- Although symptomatic nasal polyposis is stricted airflow to the olfactory region. The rare in the general population, much higher polyp stroma is highly oedematous with a vary- figures for the occurrence of isolated nasal ing density of inflammatory cells. Nasal polyps have been obtained from necropsy polyposis, consisting of recurrent, multiple studies. A thorough endoscopic examination of polyps, is part of an inflammatory reaction removed nasoethmoidal blocks and endoscopic involving the mucous membrane of the nose, examination of unselected necropsy specimens paranasal sinuses, and often the lower airways. have shown polyps in as many as 25–40% of The polyps are easily accessible for immuno- specimens.89 logical and histological studies and an increas- Allergic rhinitis has a high prevalence rate of ing number of publications have appeared in about 15–20%.10 Most cases in the western recent years, including two monographs.12 world are caused by pollen allergy, having a Nasal polyps have long been associated with seasonal occurrence. -

Otorhinolaryngology (Ear, Nose and Throat Surgery, ENT)
Published on Health Careers (https://www.healthcareers.nhs.uk) Home > Explore roles > Doctors > Roles for doctors > Surgery > Otorhinolaryngology (ear, nose and throat surgery, ENT) Otorhinolaryngology (ear, nose and throat surgery, ENT) Otorhinolaryngologists (also known as otolaryngologists or ear, nose and throat or ENT Surgeons) are surgical specialists who diagnose, evaluate and manage a wide range of diseases of the head and neck, including the ear, nose and throat regions. This page provides useful information on the nature of the work, the common procedures/interventions, sub-specialties and other roles that may interest you. Nature of the work ENT surgeons often treat conditions that affect the senses such as hearing and balance disorders or smell and taste problems. They also treat patients with conditions that affect their voice, breathing and swallowing as well as those with head and neck tumours including the skull base and interface with the brain. ENT surgeons may treat people of all ages from newborn babies to elderly people. They see more children than most other surgeons, apart from paediatric surgeons. One of the attractions is that they treat a wide spectrum of ages and diseases. A proportion of an ENT surgeon’s time is spent in outpatient clinics and managing conditions medically without the need for surgery. The use of microscopes & endoscopes in outpatients allows treatment/ diagnosis in the clinic. ENT has possibly the widest range of operations of any speciality from major head & neck procedures with flaps & complex -

Nasal Polyposis: a Review
Global Journal of Otolaryngology ISSN 2474-7556 Review Article Glob J Otolaryngol - Volume 8 Issue 2 May 2017 Copyright © All rights are reserved by Sushna Maharjan DOI: 10.19080/GJO.2017.0 Nasal Polyposis: A Review Sushna Maharjan1*, Puja Neopane2, Mamata Tiwari1 and Ramesh Parajuli3 1Department of Pathology, Chitwan Medical College Teaching Hospital, Nepal 2Department of Oral Medicine and Pathology, Health Sciences University of Hokkaido, Japan 3Department of Department of Otorhinolaryngology, Chitwan Medical College Teaching Hospital, Nepal Submission: May 07, 2017; Published: May 30, 2017 *Corresponding author: Sushna Maharjan, Department of Pathology, Chitwan Medical College Teaching Hospital (CMC-TH), P.O. Box 42, Bharatpur, Chitwan, Nepal, Email: Abstract Nasal polyp is a benign lesion that arises from the mucosa of the nasal sinuses or from the mucosa of the nasal cavity as a macroscopic usuallyedematous present mass. with The nasalexact obstruction,etiology is still rhinorrhea unknown and and postnasalcontroversial, drip. but Magnetic it is assumed resonance that imagingmain causes is suggested, are inflammatory particularly conditions to rule andout allergy. It is more common in allergic patients with asthma. Interleukin-5 has found to be significantly raised in nasal polyps. The patients seriousKeywords: conditions Allergy; such Interleukin-5; as neoplasia. Nasal Histopathological polyp; Neoplasia examination is also suggested to rule out malignancy and for definite diagnosis. Abbreviations: M:F- Male: Female; IgE: Immunoglobulin E; IL: Interleukin; CRS: Chronic Rhinosinusitis; HLA: Human Leucocyte Antigen; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging Introduction the nose and nasal sinuses characterized by stromal edema and Nasal polyps are characterized by benign lesions that arise from the mucosa of the nasal sinuses, most often from the cause may be different. -

Importance of Facial Plastic Surgery Education in Residency: a Resident Survey
Published online: 2019-12-13 THIEME 278 Original Research Importance of Facial Plastic Surgery Education in Residency: A Resident Survey Steven A. Curti1 J. Randall Jordan1 1 Department of Otolaryngology, University of Mississippi Medical Address for correspondence Steven A. Curti, MD, Department of Center, Jackson, Mississippi, United States Otolaryngology, University of Mississippi Medical Center, 2500 North State Street, Jackson, MS 39216, United States Int Arch Otorhinolaryngol 2020;24(3):e278–e281. (e-mail: [email protected]). Abstract Introduction Facial plastic and reconstructive surgery (FPRS) is a key part of the curriculum for otolaryngology residents. It is important to gain an understanding of the breadth of exposure and level of competence residents feel with these concepts during their residency. Objective To determine the level of FPRS exposure and training otolaryngology residents receive during their residency. Methods A survey was emailed to all Accreditation Council for Graduate Medical Education (ACGME) accredited otolaryngology residents. The survey aimed to find the level of exposure to FPRS procedures otolaryngology residents get and how confident they feel with their training in cosmetic FPRS. Results A total of 213 residents responded to the survey for an overall response rate of 13.4%. There was an even mixture of residents from all postgraduate year (PGY) levels, with 58% of respondents being male. Almost all (98%) of the residents felt FPRS was important to otolaryngology residency training. Exposure to procedures varied with 57% performing or assisting with cosmetic minor procedures, 81% performing or assisting with cosmetic major procedures, and 93% performing or assisting with reconstructive procedures. Only 49% of residents felt their programs either very or Keywords somewhat adequately prepared them in cosmetic facial plastic surgery. -

Department of Otorhinolaryngology and Head and Neck Surgery
570 Department of Otorhinolaryngology and Head and Neck Surgery Department of Otorhinolaryngology and Head and Neck Surgery Chairperson: Fakhri, Samer Abouchacra, Kim; Fakhri, Samer (Tenure); Fuleihan, Nabil (Adjunct Clinical); Ghafari, Joseph (Tenure); Hadi, Professors: Usamah (Clinical); Hamdan, Abdul Latif; Younis, Ramzi; Zaytoun, George Bassim, Marc; El-Bitar, Mohammad (Adjunct Faculty); Associate Professors: Geha, Hassem (Adjunct); Macari, Anthony ;Moukarbel, Roger; Saadeh, Maria (Adjunct) Barazi, Randa; Haddad, Ramzi; Natout, Mohammad Ali Assistant Professors: (Clinical) Abou Chebel, Naji (Clinical); Ammoury, Makram Instructors: (Adjunct Clinical), Chalala, Chimene (Adjunct); Korban, Zeina; Zeno, Kinan (Clinical) Abou Jaoude, Nadim; Abou Assi, Samar; Afeiche, Nada; Anhoury, Patrick; Barakat, Nabil; Chedid, Nada; Chidiac, Clinical Associates: Jose; Feghali, Roland; Ghogassian, Saro; Hanna, Antoine; Itani, Mohammad; Kassab, Ammar; Kasty, Maher; Metni, Hoda; Rezk-Lega, Felipe; Sabri, Roy The Department of Otorhinolaryngology—Head and Neck Surgery offers clinical postgraduate resident training to MD graduates. It also offers clinical clerkships to medical students and specialty electives to interns and residents. The residency program consists of five years with a gradual escalation in the clinical and surgical responsibilities of each resident. During the internship year, residents spend 9 months rotating in relevant general surgical specialties, radiology, and emergency medicine and 3 months on the Otorhinolaryngology service. The acquired general surgical skills during this year act as a foundation for their future development as surgeons in Otorhinolaryngology—Head and Neck Surgery. During the next four years of training, residents are exposed to all subspecialties in Otorhinolaryngology—Head and Neck Surgery, namely Otology, Rhinology, Laryngology, Head and Neck Surgery, Pediatric Otorhinolaryngology and Facial Plastic and Reconstructive Surgery. -

New Medical Treatments for Nasal Polyps
New Medical Treatments for Nasal Polyps February 7, 2020 Brian Modena, MD, MSc 1 Disclosures Research support: NHLBI‐Supported Researcher Self Care Catalysts: architect of Health StorylinesTM app Personal Fees: AstraZeneca, GSK, Regeneron, Sanofi 42nd Annual Pulmonary and Allergy Update Objectives 1. Discuss the epidemiology, biology, pathophysiology, and symptoms of CRS with nasal polyposis (CRSwNP). 2. Review treatment guidelines and recommendations for CRSwNP. 3. Review the many scoring systems used to evaluate CRSwNP. 4. Discuss in detail the Phase II and Phase III clinical trials using biologics for treatment of CRSwNP. Nasal Polyposis Epidemiology Prevalence = ~4%1; (CRS = ~11‐12%)2 Costs: Genetic inheritance = ~14% 2 Increases with age; peak ~50 years CRS = ~$8 billion/year Caucasians = Th2‐driven inflammation. Per patient per year: $13,000; Male to female = 2:1 $26,000 if surgery performed. Asians = Th1‐driven inflammation. Association with allergic rhinitis is weak. Surgeries/year = ~500,000 Disease Prevalence estimates 1. Hastan, Fokkens, et al, 2011 Allergic rhinitis Adult: 0.1%; Children 1.5%1 2. Lange, Holst, et al., Clin Otolaryngol 2013. 3. Mygind. JACI. 1990 Dec;86(6 Pt 1):827‐9. Asthma 5‐22% 4. Schleimer RP. Annu Rev Pathol. 2017;12:331‐57. 5. Hunter TD, DeConde AS, Manes RP. J Med Econ. 2018;21(6):610‐5. CRS 20‐25%1‐4 6. Palmer JN, Messina JC, Biletch R, et al. Allergy Asthma Proc. 2018;39:1‐9. NSAID intolerance 36‐72% 7. Pearlman AN, Chandra RK, Chang D, et al. Am J Rhinol Allergy. 2009;23(2):145‐8. NSAID intolerance and asthma 80% 8. -

Surgical Management of Polyps in the Treatment of Nasal Airway
Surgical Management of Polyps in the TreatmentofNasal Airway Obstruction Samuel S. Becker, MD KEYWORDS FESS Nasal polyps Sinonasal polyps Polyp treatment Nasal obstruction In addition to their role in chronic rhinosinusitis and nasal congestion, sinonasal polyps are associated with significant nasal obstruction. Via a purely mechanical effect (ie, obstruction at its simplest level), polyps alter and otherwise block the normal flow of air through the nose. Similarly, by blocking the drainage pathways of the paranasal sinuses, sinus inflammation and its associated symptom of congestion occur. Because the pathway that leads to the formation of sinonasal polyps has not been completely elucidated, effective long-term treatments remain difficult to pinpoint. Management of these polyps, therefore, is a difficult challenge for the contemporary otolaryngologist. Some of the more common medical treatment options include: topical and oral steroids; macrolide antibiotics; diuretic nasal washes; and intrapolyp steroid injection. Surgical options include polypectomy and functional endoscopic sinus surgery (FESS). In addition, novel treatments for polyps are introduced with some frequency. This article presents an overview of management options for sino- nasal polyps, focusing on the indications, efficacy, and complications of the more common interventions. DIAGNOSIS AND PREVALENCE OF SINONASAL POLYPS Diagnosis of sinonasal polyps relies primarily on nasal endoscopy, with computed tomography (CT) to evaluate the extent of disease. Although unilateral -

Prevalence of Benign Vocal Fold Lesions in Ear, Nose, and Throat Outpatient Unit of Dr
37 BIOMOLECULAR AND HEALTH SCIENCE JOURNAL 2020 JUNE, VOL 03 (01) ORIGINAL ARTICLE Prevalence of Benign Vocal Fold Lesions in Ear, Nose, and Throat Outpatient Unit of Dr. Soetomo General Hospital, Surabaya, Indonesia Lucia Miranti Hardianingwati1, Diar Mia Ardani2* 1Department of Otorhinolaryngology - Head and Neck Surgery, Faculty of Medicine, Universitas Airlangga - Dr. Soetomo General Hospital Surabaya, Indonesia 2Division of Pharyngeal Larynx, Department of Otorhinolaryngology - Head and Neck Surgerye, Faculty of Medicine, Universitas Airlangga - Dr. Soetomo General Hospital Surabaya, Indonesia A R T I C L E I N F O A B S T R A C T Article history: Introduction: Benign vocal fold lesions reduce the efficiency of sound production. Reports of Received 12 May 2020 dysphonia cases caused by vocal principles in Indonesia are still very limited. This study aimed to Received in revised form 06 June determine incidence and prevalence of benign vocal fold lesions, namely vocal cord nodules, cysts, 2020 and polyps. Accepted 08 June 2020 Methods: A descriptive retrospective study was conducted using patient’s medical record of Ear, Available online 30 June 2020 Nose, and Throat (ENT) Outpatient Unit. Dysphonia patients with benign vocal cord abnormalities were identified. The data analyzed using descriptive analytic. Keywords: Results: There were 20 patients with benign vocal fold lesions, consisting of 13 patients (65%) Nodule, with nodules, 3 patients (15%) with polyps, and 4 patients (20%) with cysts. The ratio of male Polyp, and female patients was 1: 1. Most patients belonged to age group of 20-59 years (12 patients; Vocal fold, 60%). In term of occupation, most patients belonged to group III, which is a group of workers Dysphonia. -

Statistical Analysis Plan
Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version V1.4 Date 14 July 2017 Decline In lung-function Among Patients with chronic obstructive Lung disease On maintenance therapy (DIAPLO) An observational study evaluating the benefits of early intervention with maintenance therapies to prevent or slow down rapid lung function decline in patients who are at high risk at the time of COPD diagnosis in the combined Optimum Patient Care Research Database and Clinical Practice Research Datalink databases TITLE PAGE Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version 14 July 2017 Date 14 July 2017 TABLE OF CONTENTS PAGE TITLE PAGE ........................................................................................................... 1 TABLE OF CONTENTS ......................................................................................... 2 LIST OF ABBREVIATIONS .................................................................................. 5 RESPONSIBLE PARTIES ...................................................................................... 6 PROTOCOL SYNOPSIS DIAPLO STUDY ........................................................... 7 AMENDMENT HISTORY ................................................................................... 12 MILESTONES ....................................................................................................... 13 1. BACKGROUND AND RATIONALE .................................................................. 14 1.1 Background ........................................................................................................... -
Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer
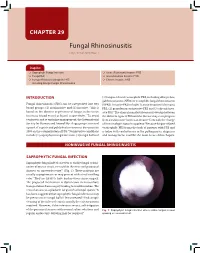
CHAPTER 29 Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer Snapshot Saprophytic Fungal Infection Acute (Fulminant) Invasive FRS Fungal Ball Granulomatous Invasive FRS Fungus-Related Eosinophilic FRS Chronic Invasive FRS Including Allergic Fungal Rhinosinusitis INTRODUCTION (3) fungus-related eosinophilic FRS, including allergic fun- gal rhinosinusitis (AFRS) or eosinphilic fungal rhinosinusitis Fungal rhinosinusitis (FRS) can be categorized into two (EFRS). Invasive FRS include (1) acute invasive (fulminant) 1 broad groups: (1) noninvasive and (2) invasive. This is FRS, (2) granulomatous invasive FRS and (3) chronic inva- based on the absence or presence of fungus in the tissue sive FRS.3 The clinical manifestations may overlap between (mucosa, blood vessel or bone) respectively.2 To avoid the different types of FRS and the disease may even progress confusion and to optimize management, the International from a noninvasive form to an invasive form with the change Society for Human and Animal Mycology group convened of immunologic status in a patient.4 Because fungus-related a panel of experts and published a consensus document in eosinophilic FRS forms the bulk of patients with FRS and 2009 on the categorization of FRS.3 Noninvasive conditions is laden with controversies in the pathogenesis, diagnosis include (1) saprophytic fungal infection, (2) fungal ball and and management, it will be the main focus of this chapter. NONINVASIVE FUNGAL RHINOSINUSITIS SAPROPHYTIC FUNGAL INFECTION Saprophytic fungal infection refers to visible fungal coloni- zation of mucus crusts seen within the nose and paranasal sinuses on nasoendoscopy3,4 (Fig. 1). These patients are usually asymptomatic or may present with a foul smelling odor.2 They are likely to have had previous sinus surgery. -

Vocal Nodules and Polyps: Clinical and Histological Diagnosis
Global Journal of Otolaryngology ISSN 2474-7556 Mini Review Glob J Otolaryngol Volume 8 Issue 5 - July 2017 Copyright © All rights are reserved by Sushna Maharjan DOI: 10.19080/GJO.2017.08.55574 Vocal Nodules and Polyps: Clinical and Histological Diagnosis Sushna Maharjan1*, Ramesh Parajuli2 and Puja Neopane3 1Department of Pathology, Chitwan Medical College Teaching Hospital, Nepal 2Department of Department of Otorhinolaryngology, Chitwan Medical College Teaching Hospital, Nepal 3Department of Oral Medicine and Pathology, School of Dentistry, Health Sciences University of Hokkaido, Japan Submission: June 19, 2017; Published: July 07, 2017 *Corresponding author: Sushna Maharjan, Department of Pathology, Chitwan Medical College Teaching Hospital (CMC-TH), P.O. Box 42, Bharatpur, Chitwan, Nepal, Email: Abstract Vocal nodules and polyps are the most common benign laryngeal lesions. Recent studies have emphasized the importance of the clinico- histological correlation in laryngeal pathologies. The clinico-histological correlation of these lesions is not always easy, but an accurate diagnosis is of the utmost importance. Keywords: Laryngeal; Nodule; Polyp; Vocal Introduction histological changes can often be seen in vocal fold nodules and Vocal nodules and polyps are the most common benign Reinke’s edema [4]. laryngeal lesions which are diagnosed primarily by patient history, clinical complaints and through visual examination such Besides the repetitive trauma, the addition causes that may contribute to polyp formation are airway infections, allergies, and stroboscopy. The etiology of both is commonly related to as indirect laryngoscopy with rigid or flexible fiber optic scope thinning medications [2]. The size and location of the polyps nicotine, gastro-esophageal reflux, aspirin and other blood lesions. -

Approaching Otolaryngology Patients During the COVID-19 Pandemic
Complete ManuscriptClick here to access/download;Complete Manuscript;Otolaryngology Diseases in COVID-19 Patients-V17-final.docx This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery. Approaching Otolaryngology Patients during the COVID-19 Pandemic Chong Cui1,2#, Qi Yao3#, Di Zhang4#, Yu Zhao1,2#, Kun Zhang1,2, Eric Nisenbaum5, Pengyu Cao1,2,6, Keqing Zhao1,2,6, Xiaolong Huang3, Dewen Leng3, Chunhan Liu4, Ning Li7, Yan Luo8, Bing Chen1,2, Roy Casiano5, Donald Weed5, Zoukaa Sargi5, Fred Telischi5, Hongzhou Lu6, James C. Denneny III9, Yilai Shu1,2 Xuezhong Liu 5 1. ENT Institute and Otorhinolaryngology Department of the Affiliated Eye and ENT Hospital, State Key Laboratory of Medical Neurobiology, Institutes of Biomedical Sciences Fudan University, Shanghai, 200031, China. 2. NHC Key Laboratory of Hearing Medicine, Fudan University, Shanghai, 200031, China. 3. Department of Otorhinolaryngology, Chinese and Western Medicine Hospital of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China. 4. Department of Otolaryngology, The Third People’s Hospital of Shenzhen, 29 Bulan Road, Longgang District, Shenzhen, 518112, China. 5. Department of Otolaryngology, University of Miami Miller School of Medicine, Miami, FL 33136, USA. 6. Department of Infectious Diseases, Shanghai Public Health Clinical Center, 2901 Caolang Road, Shanghai 201508, China 7. Department of Infectious Disease, Huashan Hospital, Fudan University, Shanghai, 200040, China. This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery. 8. Department of Hospital-Acquired Infection Control, Eye and ENT Hospital, Fudan University, Shanghai, 200031, China. 9. American Academy of Otolaryngology – Head and Neck Surgery, Alexandria, VA 22314, USA # contributed equally Corresponding Authors: Dr.