Could Semiquantitative Analysis Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Technical Reference Manual for the Standardization of Geographical Names United Nations Group of Experts on Geographical Names
ST/ESA/STAT/SER.M/87 Department of Economic and Social Affairs Statistics Division Technical reference manual for the standardization of geographical names United Nations Group of Experts on Geographical Names United Nations New York, 2007 The Department of Economic and Social Affairs of the United Nations Secretariat is a vital interface between global policies in the economic, social and environmental spheres and national action. The Department works in three main interlinked areas: (i) it compiles, generates and analyses a wide range of economic, social and environmental data and information on which Member States of the United Nations draw to review common problems and to take stock of policy options; (ii) it facilitates the negotiations of Member States in many intergovernmental bodies on joint courses of action to address ongoing or emerging global challenges; and (iii) it advises interested Governments on the ways and means of translating policy frameworks developed in United Nations conferences and summits into programmes at the country level and, through technical assistance, helps build national capacities. NOTE The designations employed and the presentation of material in the present publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The term “country” as used in the text of this publication also refers, as appropriate, to territories or areas. Symbols of United Nations documents are composed of capital letters combined with figures. ST/ESA/STAT/SER.M/87 UNITED NATIONS PUBLICATION Sales No. -

C BINGO HOUSE HALE M6ASSAD0R Itanrlfffittr Leuttititg Mrraui
1; WEDNESDAY, NOVEMBER 27, 1968 . PAGE K)URTEEN • w . iianrh^Bti^r lEtipttttts Iffralb Manchester Stores Open Tonight for Christmas Shopping Memb«m o t John Mather a member of Me financing com Chapter, Orter o f DeMolay, will mittee and olMinman o f the In- About Town have a coffee and doc^hnut Knight Head J u st ssy: utand tomonrowr at Keith's vestment oammiAtM. He ia ohe A memorial Mara lor the late of the original membeta of the Avwrngt Dafly Net PrsM R rii The Weather ParWng area from 9 am . imtil JProaMant, John f . KennedjH .CktiBens Advisory Oouncfl of "Charts It, PUass* For the Week B aM Fcreceet of U. 8. Weather B m e u after the road race. AS pro Of Kiwani& win be celebrated at noon Fri the Manoheeter Coeniminlty Neveraber 16, IMS day at the Cathedral of St. ceeds will be donated to the at Wlfidy tonight. Rein teperlng muscular dyatrophy reaearch N. WiUlem Knight o f 66 OoUege. He le currently eendng Joeeph, Hartford, at the requeet as ita oorreepoodlng secretary, off to .bower*. Low In SO* by haid. White St. was eleoM preailent of Mm Connecticut Federation of treaeurer and chairman of the 13,891 morning. 8etarday rionSy, windy Democratic Women’* Olube. of the KtwanU Club of Man itanrlfffitTr lEuTtititg MrraUi flnanoe committee. end eolder with eeettered enow Mynttc Review, Women’s chester yesterday. He le a vice ^ Mepiber ef the AnSIt Knight ie ateo a treasurer of B un ea eC OtrealettMi Annie*. Opm houM, In honor of the BaneAt Aenodaition, will have president of the Connecticut MdneheUer" A City of Village Charm Wth wedding annlverrary of Mr. -

5892 Cisco Category: Standards Track August 2010 ISSN: 2070-1721
Internet Engineering Task Force (IETF) P. Faltstrom, Ed. Request for Comments: 5892 Cisco Category: Standards Track August 2010 ISSN: 2070-1721 The Unicode Code Points and Internationalized Domain Names for Applications (IDNA) Abstract This document specifies rules for deciding whether a code point, considered in isolation or in context, is a candidate for inclusion in an Internationalized Domain Name (IDN). It is part of the specification of Internationalizing Domain Names in Applications 2008 (IDNA2008). Status of This Memo This is an Internet Standards Track document. This document is a product of the Internet Engineering Task Force (IETF). It represents the consensus of the IETF community. It has received public review and has been approved for publication by the Internet Engineering Steering Group (IESG). Further information on Internet Standards is available in Section 2 of RFC 5741. Information about the current status of this document, any errata, and how to provide feedback on it may be obtained at http://www.rfc-editor.org/info/rfc5892. Copyright Notice Copyright (c) 2010 IETF Trust and the persons identified as the document authors. All rights reserved. This document is subject to BCP 78 and the IETF Trust's Legal Provisions Relating to IETF Documents (http://trustee.ietf.org/license-info) in effect on the date of publication of this document. Please review these documents carefully, as they describe your rights and restrictions with respect to this document. Code Components extracted from this document must include Simplified BSD License text as described in Section 4.e of the Trust Legal Provisions and are provided without warranty as described in the Simplified BSD License. -

Kyrillische Schrift Für Den Computer
Hanna-Chris Gast Kyrillische Schrift für den Computer Benennung der Buchstaben, Vergleich der Transkriptionen in Bibliotheken und Standesämtern, Auflistung der Unicodes sowie Tastaturbelegung für Windows XP Inhalt Seite Vorwort ................................................................................................................................................ 2 1 Kyrillische Schriftzeichen mit Benennung................................................................................... 3 1.1 Die Buchstaben im Russischen mit Schreibschrift und Aussprache.................................. 3 1.2 Kyrillische Schriftzeichen anderer slawischer Sprachen.................................................... 9 1.3 Veraltete kyrillische Schriftzeichen .................................................................................... 10 1.4 Die gebräuchlichen Sonderzeichen ..................................................................................... 11 2 Transliterationen und Transkriptionen (Umschriften) .......................................................... 13 2.1 Begriffe zum Thema Transkription/Transliteration/Umschrift ...................................... 13 2.2 Normen und Vorschriften für Bibliotheken und Standesämter....................................... 15 2.3 Tabellarische Übersicht der Umschriften aus dem Russischen ....................................... 21 2.4 Transliterationen veralteter kyrillischer Buchstaben ....................................................... 25 2.5 Transliterationen bei anderen slawischen -

The Unicode Standard 5.1 Code Charts
Cyrillic Supplement Range: 0500–052F The Unicode Standard, Version 5.1 This file contains an excerpt from the character code tables and list of character names for The Unicode Standard, Version 5.1. Characters in this chart that are new for The Unicode Standard, Version 5.1 are shown in conjunction with any existing characters. For ease of reference, the new characters have been highlighted in the chart grid and in the names list. This file will not be updated with errata, or when additional characters are assigned to the Unicode Standard. See http://www.unicode.org/errata/ for an up-to-date list of errata. See http://www.unicode.org/charts/ for access to a complete list of the latest character code charts. See http://www.unicode.org/charts/PDF/Unicode-5.1/ for charts showing only the characters added in Unicode 5.1. See http://www.unicode.org/Public/5.1.0/charts/ for a complete archived file of character code charts for Unicode 5.1. Disclaimer These charts are provided as the online reference to the character contents of the Unicode Standard, Version 5.1 but do not provide all the information needed to fully support individual scripts using the Unicode Standard. For a complete understanding of the use of the characters contained in this file, please consult the appropriate sections of The Unicode Standard, Version 5.0 (ISBN 0-321-48091-0), online at http://www.unicode.org/versions/Unicode5.0.0/, as well as Unicode Standard Annexes #9, #11, #14, #15, #24, #29, #31, #34, #38, #41, #42, and #44, the other Unicode Technical Reports and Standards, and the Unicode Character Database, which are available online. -

General Glossary
GENERAL GLOSSARY Where the gender of nouns is not marked, it should be assumed that those ending in -ta are feminine and those with any other ending are masculine. The gender is marked when it is not predictable in this way. The plural of a noun is indicated when it is known. The annexation form is given only where it differs from the normal pattem with final -itl-id. The absolute state is indicated for the small number of nouns that have preserved this. For other principles followed in the general glossary, see the introduction to the glossary of verbs. 2 ?ana coin I xa ?ana la-paltet 1 You ?adi then, and so shall not take out a single coin (S:48) ?afandi gentleman (Kurd.) ?afillu even (Heb.) ?anne these/those (L, S) ?agar if (Kurd.) (§19.4.1) ?ara f., pl. ?aräne ground ?aglinja friendly gathering (Kurd.) ?arba four I ?aglinja matwlwa 1 They ?arba-sar fourteen held a friendly gathering ?arbamin fourth (Y:81) ?arbelna, ?arbenna, ?arbinna, f. ?ajal end (of life) (Kurd. < Arab.) ?arbelta, ?arbelnela, pl. ?alpa thousand I tre ?a/pa two ?arbinne inhabitant of Arbel thousand, t!!Jha ?a/pa three ?arbi forty thousand, etc. ?arbusab Wednesday ?amalyat f. operation (medical) ?arlf, pl. ?arife large loaf of bread (Kurd. < Arab.) I dabl (L:567) (Arab.) ?ama/yat ?o/ 1 He must have ?armalta, pl. ?arma/ye widow an operation (L:60) ?arota Friday ?amir order, command (Kurd. < ?arzäq supplies (treated Arab.) grammatically as singular) ?amln trustworthy (Arab.) (Arab.) ?amman but (Arab.) ?asin hammer (Kurd.) ?amona, pl. -

Electronic Supplementary Information (ESI)
Electronic Supplementary Material (ESI) for Nanoscale. This journal is © The Royal Society of Chemistry 2020 Electronic Supplementary Information (ESI) A versatile UCST-type composite microsphere for image-guided chemoembolization and photothermal therapy against liver cancer Dan Huanga#, Haitao Daib, c#, Keyu Tangb, c#, Bin Chenb, c, Hongzhang Zhub, Dubo Chend, Nan Lib, Yingzhao Wange, Chuwei Liue, Yonghui Huangb, Jianyong Yangb, c, Chao Zhanga, c*, Run Linb, c*, Weiling Hec, e* aSchool of Biomedical Engineering, Sun Yat-Sen University, Shenzhen, Guangdong, 518107, China bDepartment of Radiology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510080, China cCenter for Precision Medicine, Sun Yat-Sen University, Guangzhou, Guangdong, 510080, China dDepartment of Laboratory Medicine, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510080, China eDepartment of Gastrointestinal Surgery, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510080, China *Corresponding Authors: Chao Zhang, Ph.D. School of Biomedical Engineering, and Center for Precision Medicine, Sun Yat-Sen University, Shenzhen 518107, Guangdong, China. E-mail: [email protected] Run Lin, M.D. Center for Precision Medicine, and Department of Radiology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510080, China. E-mail: [email protected] Weiling He, M.D. Center for Precision Medicine, and Department of Gastrointestinal Surgery, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510080, China. E-mail: [email protected] #These authors contributed equally to this work. Preparation of polydopamine coated SPION To prepare polydopamine coated SPION (SPION@PDA), 30 mg of dopamine was mixed with 25 mg of SPION in 250 mL of 10 mM PBS (pH 8.5). -

Navy LPD-17 Flight II and LHA Amphibious Ship Programs: Background and Issues for Congress
Navy LPD-17 Flight II and LHA Amphibious Ship Programs: Background and Issues for Congress Updated August 26, 2019 Congressional Research Service https://crsreports.congress.gov R43543 Navy LPD-17 Flight II and LHA Amphibious Ship Programs Summary The Navy wants to procure a total of 13 LPD-17 Flight II amphibious ships. LPD-17 Flight II ships cost roughly $1.8 billion each to procure. The first LPD-17 Flight II ship, LPD-30, was procured in FY2018. As part of its action on the Navy’s proposed FY2019 budget, Congress provided $350 million in unrequested advance procurement (AP) funding for a second LPD-17 Flight II ship, LPD-31, to be procured in FY2020. This was consistent with the Navy’s FY2019 budget submission, under which LPD-31 was planned for procurement in FY2020 and the remainder of its procurement cost was to be requested in FY2020. The Navy’s FY2020 budget submission, however, proposes deferring the procurement of LPD-31 by one year, to FY2021, and the Navy’s proposed FY2020 budget, rather than requesting the remainder of LPD-31’s procurement cost, instead requests $247.1 million in AP funding for the ship. Navy officials state that if no LPD-17 Flight II ship is procured in FY2020, the $350 million in FY2019 AP funding that Congress provided for the LPD-17 program would become unexecutable, because that funding was provided specifically for use in building an LPD-17 Flight II ship procured in FY2020, not an LPD-17 Flight II ship procured in FY2021. The $350 million in FY2019 AP funding can be made executable by procuring LPD-31 in FY2020 or by passing legislation permitting the FY2019 AP funding to be used for an LPD-17 Flight II ship procured in FY2021. -

Cyrillic # Version Number
############################################################### # # TLD: xn--j1aef # Script: Cyrillic # Version Number: 1.0 # Effective Date: July 1st, 2011 # Registry: Verisign, Inc. # Address: 12061 Bluemont Way, Reston VA 20190, USA # Telephone: +1 (703) 925-6999 # Email: [email protected] # URL: http://www.verisigninc.com # ############################################################### ############################################################### # # Codepoints allowed from the Cyrillic script. # ############################################################### U+0430 # CYRILLIC SMALL LETTER A U+0431 # CYRILLIC SMALL LETTER BE U+0432 # CYRILLIC SMALL LETTER VE U+0433 # CYRILLIC SMALL LETTER GE U+0434 # CYRILLIC SMALL LETTER DE U+0435 # CYRILLIC SMALL LETTER IE U+0436 # CYRILLIC SMALL LETTER ZHE U+0437 # CYRILLIC SMALL LETTER ZE U+0438 # CYRILLIC SMALL LETTER II U+0439 # CYRILLIC SMALL LETTER SHORT II U+043A # CYRILLIC SMALL LETTER KA U+043B # CYRILLIC SMALL LETTER EL U+043C # CYRILLIC SMALL LETTER EM U+043D # CYRILLIC SMALL LETTER EN U+043E # CYRILLIC SMALL LETTER O U+043F # CYRILLIC SMALL LETTER PE U+0440 # CYRILLIC SMALL LETTER ER U+0441 # CYRILLIC SMALL LETTER ES U+0442 # CYRILLIC SMALL LETTER TE U+0443 # CYRILLIC SMALL LETTER U U+0444 # CYRILLIC SMALL LETTER EF U+0445 # CYRILLIC SMALL LETTER KHA U+0446 # CYRILLIC SMALL LETTER TSE U+0447 # CYRILLIC SMALL LETTER CHE U+0448 # CYRILLIC SMALL LETTER SHA U+0449 # CYRILLIC SMALL LETTER SHCHA U+044A # CYRILLIC SMALL LETTER HARD SIGN U+044B # CYRILLIC SMALL LETTER YERI U+044C # CYRILLIC -
Prayers to Pacify the Dangers of Earthquake
Prayers to Pacify the Dangers of Earthquake As advised by Kyabje Zopa Rinpoche Ksitigarbha Practice I prostrate, go for refuge, and make offerings to the bodhisattva Ksitigarbha who has unbearable compassion for me and all sentient beings who are suffering and whose minds are obscured, who has qualities like the sky and liberates sentient beings from all suffering and gives every happiness. Please grant blessings! (3x) With hands folded in prostration, you can visualize doing the prostration to all the buddhas and bodhisattvas – that becomes prostration when you say the word “prostration.” When you say “refuge,” think that you are asking to be free from the two obscurations (to be able to achieve enlightenment). When you say the word “offering,” think all the offerings that you have are then offered. Then, when you ask for “blessings,” think in the mind the whole path to enlightenment – this is the blessing to be received. So the extensive benefits of this mantra will be translated. This is the mantra that Kshitigarbha heard from buddhas equaling the number of sand grains of the river Ganga (in India). He made offerings to them and then received this mantra. This is the story of the mantra – how to receive all of the benefits. This mantra is to be used for any difficulties of problems. It is the best one to do for any problems in any situation. Even reciting it only four or five times – just a few times – is very powerful. It speaks so much of power, showing how important the bodhisattva is. Even to recite or just to think of the name of the bodhisattva is very, very powerful. -

MSR-4: Annotated Repertoire Tables, Non-CJK
Maximal Starting Repertoire - MSR-4 Annotated Repertoire Tables, Non-CJK Integration Panel Date: 2019-01-25 How to read this file: This file shows all non-CJK characters that are included in the MSR-4 with a yellow background. The set of these code points matches the repertoire specified in the XML format of the MSR. Where present, annotations on individual code points indicate some or all of the languages a code point is used for. This file lists only those Unicode blocks containing non-CJK code points included in the MSR. Code points listed in this document, which are PVALID in IDNA2008 but excluded from the MSR for various reasons are shown with pinkish annotations indicating the primary rationale for excluding the code points, together with other information about usage background, where present. Code points shown with a white background are not PVALID in IDNA2008. Repertoire corresponding to the CJK Unified Ideographs: Main (4E00-9FFF), Extension-A (3400-4DBF), Extension B (20000- 2A6DF), and Hangul Syllables (AC00-D7A3) are included in separate files. For links to these files see "Maximal Starting Repertoire - MSR-4: Overview and Rationale". How the repertoire was chosen: This file only provides a brief categorization of code points that are PVALID in IDNA2008 but excluded from the MSR. For a complete discussion of the principles and guidelines followed by the Integration Panel in creating the MSR, as well as links to the other files, please see “Maximal Starting Repertoire - MSR-4: Overview and Rationale”. Brief description of exclusion -
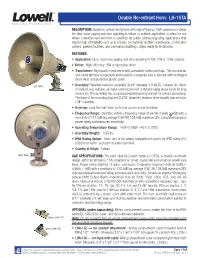
Double Re-Entrant Horn: LH-15TA
Double Re-entrant Horn: LH-15TA DESCRIPTION: Double re-entrant metal horn with high efficiency 15W compression driver for clear voice paging and tone signaling in indoor or outdoor applications is ideal for use where a weather-resistant horn is specified for public address/signaling applications that require high intelligibility such as in schools, recreational facilities, warehouses, distribution centers, parking facilities, and commercial buildings. Ships ready for installation. FEATURES: • Application: Clear, loud voice paging and tone signaling in 25V, 70V or 100V systems. • Driver: High efficiency 15W compression driver • Transformer: High quality transformer with screwdriver-selectable taps. The tap selector and screw terminal connections are located in a recessed area in the rear with an integral strain relief and protective plastic cover. LH-15TA • Assembly: Weather-resistant assembly (8.94" diameter x 9.38"D), suitable for indoor or outdoor use, features all-metal construction with a durable beige epoxy finish for long service life. The assembly has a universal swivel mounting bracket for precise positioning. The base of the mounting bracket (2.875" diameter) features three equally spaced holes (.28" diameter). • Hook-up: Easy two-wire hook-up to rear access screw terminals. • Frequency Range: Operates within a frequency range of 537Hz-4.5kHz (+6dB) with a sensitivity of 112.2dB log average (1W/1M) 124.0dB maximum SPL (calculated based on power rating and measured sensitivity). • Operating Temperature Range: -40˚F to 158˚F (-40˚C to 70˚C) • Assembly Weight: 3.55 lbs. • IP66 Rating Option: Order one of the wiring compartment covers for IP66 rating (IEC 60529) for water- and dust-resistant operation.