Type 2 Diabetes Report for 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Making the Right Move
MAKING THE RIGHT MOVE Investing and Creating Jobs in the Pittsburgh Region REAL PITTSBURGH REAL PEOPLE Looking Ahead: 2014 and Beyond Imagining a Bright Future for Our Region – and Making it Happen By Charles E. Bunch In many ways, the Pittsburgh region has com- Boomers. We’re seeing this on our job search engine within Imag- pleted the economic, environmental and qual- inePittsburgh.com, where the number of open jobs across the 10- ity-of-life transformation begun 30 years ago. county Pittsburgh region numbered around 25,000 at last count. We bottomed out in 1983, with an unemploy- ment rate over 18 percent. Throughout 2013, The Conference is addressing this opportunity in a variety of ways, in- WHEN YOU INVEST IN THE cluding through our robust talent attraction and retention initiative, COMMUNITY, THE RETURNS our jobless rate outperformed the state and the nation as a whole. We’re closing the year with the largest workforce which includes ImaginePittsburgh.com. We’re also working with ARE GUARANTEED. in regional history – about 100,000 more people employed than at our partners in workforce development to increase the supply of trained At Huntington, we know how important it is to give back to workers in the region. One such program, ShaleNET, has been such the community. After all, we do more than just work here – we industrial peak in 1979. live and raise our families here too. And after everything this a success that the federal government has increased its investment to community has done for us, we’re just happy to be able to We are enjoying the fruits of three decades of hard work by countless expand it to other states. -

Palumbo-Donahue School of Business 2015-2016 Graduate Outcomes
Palumbo-Donahue School of Business 2015-2016 Graduate Outcomes NUMBER OF RESPONDENTS RESPONDENTS ATTENDING AVERAGE MAJOR RESPONDENTS EMPLOYED GRADUATE SCHOOL SALARY TOP EMPLOYERS Bachelor’s Degree Accounting 61 59% 26% $49,283 BNY Mellon, Deloitte, EY, KPMG, PNC, PwC, Schneider Downs, ThermoFisher Scientific Economics 6 67% 33% $50,000 Craneware, Henderson Brothers, PNC Entrepreneurship 3 33% 33% Dick’s Sporting Goods Finance 31 64% 16% $51,038 Deloitte, Federated Investors, Hudson Companies, PNC, Rockwell Automation Information Systems 23 96% 4% $55,450 Duquesne Light, Federated Investors, Management Giant Eagle, Pittsburgh Pirates, PNC, UPMC International Business 7 71% $51,500 Amazon, Hertz, Westinghouse Electric Legal Studies 3 100% Management 13 69% 15% $45,450 American Eagle, Brookstone Inc., Embassy Suites, Macy’s, PNC Marketing 24 67% 16% $46,409 ADP, Diamond Kinetics, MARC USA, PNC Sports Marketing 6 67% $39,333 Ferguson, Fragasso Financial Advisors, Tesla Motors Supply Chain Management 41 78% 7% $56,930 Amazon, Bechtel Plant Machinery, Cisco Systems, Lockheed Martin, PPG, Wabtec, Wesco Distribution Master’s Degree Accountancy 5 100% $49,333 Deloitte, EY, KPMG Business Administration 31 74% 6% $76,881 Bayer, BNY Mellon, Cigna, Federated Investors, FedEx PNC, United States Steel Information Systems 5 60% 20% $65,333 Apple, PNC Sustainability 5 60% AECOM, BNY Mellon, Idea Foundry Palumbo-Donahue School of Business 2015-2016 Graduate Outcomes AUGUST 2015, DECEMBER 2015 AND MAY 2016 GRADUATES Profile information is based on student -

Top 50 Employers
Top 50 Employers Adams County 4th Quarter, 2015 Combined Government Ownerships Rank Employer Rank Employer 1 Knouse Foods Cooperative Inc 26 Upper Adams School District 2 Gettysburg College 27 Dal-Tile Services Inc 3 The Gettysburg Hospital 28 International Paper Company 4 Federal Government 29 Passage Healthcare LLC 5 The Brethren Home Community 30 Hoffman Homes Inc 6 Hain Pure Protein Corporation 31 State Government 7 Tim-Bar Corporation 32 Wal-Mart Associates Inc 8 Conewago Valley School District 33 Giant Food Stores LLC 9 Adams County 34 Utz Quality Foods Inc 10 Gettysburg Area School District 35 Rice Fruit Company 11 C&J Clark America Inc 36 Lutheran Social Services 12 Aerotek Inc 37 Jacoby Transportation Inc 13 WellSpan Medical Group 38 Transitions Healthcare Gettysburg 14 Pella Corporation 39 Fairfield Area School District 15 Hillandale Gettysburg LP 40 Genlyte Thomas Group LLC 16 World Color Printing (USA) II Corp 41 Pennwood Products Inc 17 Littlestown Area School District 42 Specialty Granules Inc 18 Motts LLP 43 Haverfield International Inc 19 Ski Liberty Operating Corp 44 Truenorth Wellness Services 20 Kennies Markets Inc 45 YWCA of Gettysburg & Adams County 21 Conewago Enterprises Inc 46 United Parcel Service Inc 22 Bermudian Springs School District 47 Focus Behavioral Health Inc 23 ACNB Bank 48 JDCS Enterprise 24 Lincoln Intermediate Unit No. 12 49 Hanover Prest-Paving Company 25 Diocese of Harrisburg 50 Winter Gardens Quality Foods Inc Source: Quarterly Census of Employment and Wages Center for Workforce Information & Analysis -
Interaction-Spring 08:Interaction-Spring 08
A QUARTERLY PUBLICATION OF THE EPILEPSY FOUNDATION WESTERN/CENTRAL PENNSYLVANIA Spring 2008 www.efwp.org 20th20th AAnniversary!nniversary! Pittsburgh Fun Run/Walk Going 20 Years Strong EPILEPSY FOUNDATION WESTERN/CENTRAL PENNSYLVANIA Western PA Office: Central PA Office: 1501 Reedsdale Street 900 South Arlington Avenue Suite 3002 Suite 126 Pittsburgh, PA 15233 Harrisburg, PA 17109 TOLL FREE: 1-800-361-5885 TOLL FREE: 1-800-336-0301 PHONE: 412-322-5880 PHONE: 717-541-0301 FAX: 412-322-7885 FAX: 717-541-1202 WEBSITE: www.efwp.org EMAIL: [email protected] South Central PA Office: TDD EOP/AUX AID: 1-800-855- 2880 1450 Scalp Avenue Suite 1150 Northwest PA Office: Johnstown, PA 15904 915 State Street PHONE:814-262-7494 Suite 101 Erie, PA 16501 A copy of our official registration and financial information may be obtained from the PHONE: 814-451-1135 Pennsylvania Department of State by calling toll free, within Pennsylvania, 1-800-732-0999. FAX: 814-451-1150 Registration does not imply endorsement. Policy Board Tom Trimm, Esq. Denis McCarthy James Valeriano, M.D. President Karin A.Vanek Team Aiden came out in full force for the 19th annual Pittsburgh Pirates Fun Run/Walk last year. Justin Yakovac Claudio F. Abreu, Ph.D. Sharon Aulicino Board of Governors Dick Barton Douglas Dick Joyce Bender Steve Morris Louis Catalano, M.D. Rich Ryan Fun Run/Walks All Tom Chakurda Advisory Board James D. Chiafullo Barbara Johanson Patricia Crumrine, M.D. Bobbie Martha Eugene DeFrank C. James Parks Kristin Lesker Eisel Across the State! Ronald Rohm Julie Faneca James Valeriano, M.D. -

Download the Report Here
20 20 MANAGED CARE ® 1987 SINCE DIGEST SERIES Pittsburgh Business Group on Health Type 2 Diabetes Report™ Featuring Demographic, Utilization, Charge, and Pharmacotherapy Data With a Focus on Patients With Commercial Insurance Coverage 13th Edition www.pbghpa.org PBGH TYPE 2 DIABETES REPORT™ INTRODUCTION Sanofi U.S. (Sanofi) and the Pittsburgh Business Group on Health (PBGH) Most of the data in this report (current as of calendar year 2019) were are pleased to present the 13th edition of the Type 2 Diabetes Report™, gathered by IQVIA, Durham, NC, a leading provider of innovative health an overview of key demographic, utilization, charge, pharmacotherapy, care data products and analytic services. A review process takes place, and health outcome measures for Type 2 diabetes patients in Pittsburgh before and during production of this report, between IQVIA and Forte and western Pennsylvania (Erie and Johnstown), as well as parts of Ohio Information Resources LLC. (Youngstown) and West Virginia (Wheeling). The report also provides Sanofi, as sponsor of this report, maintains an arm’s-length relationship supplemental data on patients with respiratory conditions as well as IQVIA’s with the organizations that prepare the report and carry out the research state and national benchmarks, which help providers and employers better for its contents. The desire of Sanofi is that the information in this report be identify opportunities to serve the needs of their patients. All data are drawn completely independent and objective. from the Sanofi Managed Care Digest Series®. PBGH EMPLOYER MEMBERS 84 Lumber Company Civil & Environmental Ellwood Group, Inc. Mitsubishi Electric Power Specialty Tires of America Allegheny County Consultants, Inc. -

The Pittsburgh Promise 2020 Report to the Community the Pittsburgh Promise 2020 Report to the Community
THE PITTSBURGH PROMISE 2020 REPORT TO THE COMMUNITY THE PITTSBURGH PROMISE 2020 REPORT TO THE COMMUNITY From the beginning, The Pittsburgh Promise was a big idea. This one-two punch only served to strengthen our resolve and inflame our Today, that big idea is creating economic mobility for urban youth and determination “to advance a region that is good and just for all,” as we proclaim a more diverse workforce for our region. This report demonstrates that in our vision statement. The Pittsburgh Promise is working. We sprang into action with emergency outreach to identify and serve more than In January 2020, we launched a new initiative that deploys Promise Coaches 700 students who severely experienced COVID’s impacts. We raised $1.3 million The Promise into our urban high schools to reach our most vulnerable students. Their mission through which we addressed food insecurity by providing grocery gift cards; is to equip students with the tools they need to identify their skills and interests, restored well-being by paying for mental health services; and kept students on their post-secondary pathway by giving extra tuition scholarships for spring, build on the supports available to them, understand the educational options in Franco Harris summer, and fall semesters to make up for the lack of summer jobs available is Working front of them, develop the soft skills employers demand of them, and prepare for CHAIR the jobs and opportunities that exist in the region’s marketplace. We hired and to students or to fill gaps created by their parents’ unemployment. dedicated nine highly skilled and mission-driven emerging leaders to find and We continued to do our core work of helping kids pursue their dreams through empower the students who might not, on their own, find their way to their future hard work and post-secondary education without interruption. -
Survey Class of 2012 Post-Graduation Status (Summer
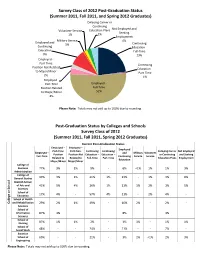
Survey Class of 2012 Post-Graduation Status (Summer 2011, Fall 2011, and Spring 2012 Graduates) Delaying Career or Continuing Not Employed and Volunteer Service Education Plans Seeking 1% 2% Employment Military Service 4% Employed and 1% Continuing Continuing Education - Education Full-Time 9% 23% Employed - Part-Time Continuing Position Not Related Education - to Major/Minor Part-Time 2% 1% Employed - Part-Time Employed - Position Related Full-Time to Major/Minor 52% 4% Please Note: Totals may not add up to 100% due to rounding. Post-Graduation Status by Colleges and Schools Survey Class of 2012 (Summer 2011, Fall 2011, Spring 2012 Graduates) Current Post-Graduation Status Employed – Employed – Employed Part-Time Part-Time Continuing Continuing Delaying Career Not Employed Employed – and Military Volunteer Position Position Not Education – Education – or Continuing and Seeking Full-Time Continuing Service Service Related to Related to Full-Time Part-Time Education Plans Employment Education Major/Minor Major/Minor College of Business 77% 3% 1% 9% - 6% <1% 1% 1% 3% Administration College of General Studies 49% 3% 1% 21% 1% 13% - 1% 3% 8% Dietrich School of Arts and 41% 5% 4% 26% 1% 11% 1% 2% 3% 5% Sciences School of Education 17% 4% - 57% 4% 11% - 2% 4% - School of Health College orSchool College and Rehabilitation 29% 2% 1% 49% - 16% 2% - 2% - Sciences School of Information 87% 3% - - - 8% - - 3% - Sciences School of Nursing 87% 1% 1% 2% - 3% 3% - 1% 1% School of Social Work 48% - - 24% - 21% - - 7% - Swanson School of 69% - - 21% - 3% 2% <1% 2% 3% Engineering Please Note: Totals may not add up to 100% due to rounding. -

Pittsburgh Area Organizations That Hire Chemists, Chemical Engineers, and Chemical Technicians
Pittsburgh Area Organizations that Hire Chemists, Chemical Engineers, and Chemical Technicians Initial Release Date: March 11, 2013 Compiled by Joseph Jolson with input from: The Joint Employment Committee of the ACS – Pittsburgh Section, AIChE – Pittsburgh Chapter, SACP and SSP* Analytical, Material, Medical and Testing Laboratories Clark Testing www.clarktestinggroup.com Delta Analytical Instruments, Inc. www.deltalab.com Industrial Testing Laboratory Services, LLC www.itls.com KTA Associates, Inc. http://ktainc.net Matco Services, Inc. www.matcoinc.com Microbac Laboratories, Inc. www.microbac.com Microseeps, Inc. www.microseeps.com Pace Analytical Services, Inc. www.pacelabs.com Professional Analytical and Consulting Services www.pacslabs.com Professional Services Industries, Inc. www.psiusa.com Quest Diagnostics www.questdiagnostics.com RJ Lee Group www.rjlg.com TestAmerica www.testamericainc.com West Penn Testing Group www.westpenntesting.com Ceramic and Glass Manufacturers ANH Refractories Company www.hwr.com Ardex Group www.ardex.com Dielectric Solutions www.dielectricsolutions.com Dlubak Corporation www.dlubakglass.com PPG Industries, Inc. www.ppg.com Sauereisen www.sauereisen.com Food Companies Del Monte Foods www.delmonte.com H.J. Heinz Company www.heinz.com Gas Detection and Safety Equipment Manufacturers Ametek, Inc. www.ametek.com Bacharach Inc. www.bacharach-inc.com Breen Energy Solutions www.breenes.com ChemDAQ Incorporated www.chemdaq.com Conspec Controls www.conspec-controls.com CSE Corporation www.csecorporation.com Draeger Safety, Inc. www.draeger.us FLIR Systems, Inc. http://gs.flir.com Industrial Scientific Corporation www.indsci.com Mine Safety Appliances Company, Inc. www.msanet.com NanoLambda www.nanolambda4u.net Rel-Tek Corporation www.rel-tek.com Ferrous and Non-Ferrous Metals AK Steel www.aksteel.com ALCOA www.alcoa.com Allegheny Technologies Inc. -
Course Catalog
APRIL–JUNE 2007 COURSE CATALOG NONPROFITS BUILD STRONG COMMUNITIES... WE BUILD STRONG NONPROFITS. THE BAYER CENTER FOR NONPROFIT MANAGEMENT AT ROBERT MORRIS UNIVERSITY A MESSAGE FROM THE EXECUTIVE DIRECTOR The newspaper headline read, “Nonprofits Less Effective … Spending More on Overhead, Less on Mission.” And you could hear a collective shudder go through the populace and checkbooks snapping shut! Charity Navigator had spoken – Pittsburgh’s nonprofit organizations are less effective than those in 25 other cities. In using the 990 form for its analysis, Charity Navigator is passing judgment on the nation’s nonprofits – and urging donors to make giving decisions based on their formula. But is the 990 a true record of expenses in nonprofits? When the Bayer Center released its Wage and Benefit Survey in January, we hosted a session with Kennard Wing, a consultant who worked on a national project examining overhead costs of nonprofits. Ken’s groups looked at 228,000 990 forms to see how various groups in all stages of development, with all budget sizes and all types of causes, reported their use of dollars from all revenue sources. This well-respected study showed that in many cases, nonprofits showed little to no management and general or fundraising expenses at all. Those agencies must have looked particularly appealing to Charity Navigator! There is currently no standard for reporting nonprofit management and fundraising expenses. Individual groups and their auditors have to make their own decisions about how best to allocate their expenses. And for agencies that lack detailed time sheets, the true picture of overhead versus program/mission-related activities remains quite elusive. -

Leadership That Lifts Us All Recognizing Outstanding Philanthropy 2017 - 2018
Leadership That Lifts Us All Recognizing Outstanding Philanthropy 2017 - 2018 uwswpa.org Thank you to our 2017 sponsors: Premier Gold Dear Friends, As philanthropic leaders who, through their generous gifts of time and treasure, demonstrate their commitment to tackling our community’s most pressing problems, we should be proud of the impact we make on the lives of people who need our help. Through our gifts – Tocqueville Society members contributed nearly $10 million to the United Way 2017 Campaign – the most vulnerable members of our community are getting much-needed support: Dan Onorato • local children like Alijah (page 18) are matched with caring mentors who are helping them plan to continue their education after high school; • seniors like Jean (page 4) are receiving support that helps them remain in the homes they love; • people with disabilities like Kenny (page 9) are getting the opportunity to find 1 meaningful work; and • women like Sarah (page 43) are able to overcome challenges in order to gain greater financial stability. On behalf of our community, thank you for your support. Your gift helps United Way put solutions into action, making a difference and encouraging hope for a better David Schlosser tomorrow for everyone. With warmest regards Dan Onorato David Schlosser 2017 Tocqueville Society Co-Chair 2017 Tocqueville Society Co-Chair 2017 Top Tocqueville Corporations The Tocqueville Society Tocqueville Society Membership Growth United Way recognizes these United Way’s Tocqueville Society is corporations that had the largest comprised of philanthropic leaders 2011 430 number of Tocqueville Society and volunteer champions who donors for the 2017 campaign, give $10,000 or more annually to regardless of company size or United Way, creating a profound 2012 458 overall campaign total. -

Pittsburgh, PA Previous GTCA City 2013
Pittsburgh, PA Previous GTCA City 2013 Contact: Tom Piccone ([email protected]); Andy Wang ([email protected]) The Church of God in Pittsburgh The Church of God in Pittsburgh was originally established as the Church in Pittsburgh in 1983, primarily through a migration of saints mainly from Ohio. Some years after a turmoil, the Church of God in Pittsburgh was incorporated in 2017. The church does not presently have a meeting hall, but meets on university campuses and in various saints’ homes. Approximately 40 currently gather on Lord’s Day mornings, including four children. The racial composition of the church is 59% Chinese and 16% Caucasian, with the remaining 25% a mix of Korean, Vietnamese, Black, and Indian. The current church life in Pittsburgh focuses primarily on campus work at the University of Pittsburgh (Pitt) and Carnegie Mellon University (CMU), though the need to gain more families is of equal priority (and not necessarily separate). Each year, the Lord adds remaining fruit to His Body through the saints’ labor on the campuses to gain college and graduate students, and sometimes university staff. In the past 12 years of campus work, dozens have been gained, but most have moved away. Only a handful of them have not been Asian. While the saints in Pittsburgh welcome all who would like to move here, we particularly see a need for young American families to migrate to the Pittsburgh area in order to share the burden of shepherding and gaining some from the population of American students and families for the strengthening of His testimony in this locality and region. -

2019 Annual Report
Dear Friends, I’m excited to share with you our Annual Report for 2019, which marked Tickets for Kids’ 25th year! From grass-roots beginnings in Pittsburgh, to joining forces with great, like-minded organizations in Minneapolis and New York, the passion and enthusiasm of those who make this work possible has spread to all corners of the country. As a result, 206,663 experiences were provided last year to our nonprofit agency partners in 40 states. This milestone year also provided an opportunity to reflect on how to grow our mission and impact for the next 25 years, while maintaining the same levels of professionalism and service you have come to expect. To that end, we’ve begun targeting four key markets for focused growth — Pittsburgh, Minneapolis/St. Paul, New York, and Sarasota/Tampa (more on this inside). In meeting with ticket donors, financial supporters, and agency partners in each of these markets, the reception that this mission continues to receive has been awe- inspiring. In sharing our vision with new audiences, the resounding chorus of “yes” we almost invariably hear is a humbling affirmation that the TFK mission is more ANNUAL REPORT ANNUAL relevant and necessary than ever. Thank you for believing in the power of experiences, and for ensuring that all kids have access to a diversity of formative opportunities through the Tickets for Kids program. Together with you, we look forward to building our next 25 years. Warm regards, 2019 Jason J. Riley [email protected] Tickets Agencies Many new ticket providers from across the country In 2019, TFK provided opportunities to 1,349 AGENCY joined us in 2019 including the MINNESOTA HISTORICAL PARTNERS located in 40 STATES.