Infusion Therapy Standards of Practice 8Th Ed 2021.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Drill Bits 101 I've Used Dowels in a Variety of Woodworking Projects
Drill Bits 101 I’ve used dowels in a variety of woodworking projects having bought myself a pretty decent doweling jig a few years ago. The jig itself came with a twist drill bit for each of the three dowel sizes. For my dowel joinery I often need to drill holes of two different depths; so sometimes it is handy to have two bits of the same diameter with stops set at the different depths. One day I inadvertently was using both a twist bit and a brad point bit and noticed very different results. For example, drilling into end grain was far more difficult with a brad point bit than with the twist bit. All of this got me wondering about the different types of woodworking drill bits. Hence my investigation into the family tree of woodworking drill bits. Note that many drill bits may be multi-purpose, but generally speaking there are different families of bits for plastic, metal(s), tile, and masonry, etc. The basic job of a drill bit of course is to stay centered and not wander, cut the wood to form a round hole, and eject the chips. Seems simple, but not so perhaps, which is why there are so many types of drill bits and even options on lips, lands, flutes, margins, and other design elements – details beyond the scope of Bevel Cut. Of all the types, the common twist drill, invented by Steven Morse in 1863 and covered in US Patent 38119 is the simplest. The V-angle of the tip can vary from 60 to 118 degrees, with the latter being most common in today’s hardware stores according to my own research. -

Wowza Media Server® - Overview
Wowza Media Server® - Overview Wowza® Media Systems, LLC. June 2013, Wowza Media Server version 3.6 Copyright © 2006 – 2013 Wowza Media Systems, LLC. All rights reserved. Wowza Media Server version 3.6 Overview Copyright © 2006 - 2013 Wowza Media Systems, LLC. All rights reserved. This document is for informational purposes only and in no way shall be interpreted or construed to create any warranties of any kind, either express or implied, regarding the information contained herein. Third-Party Information This document contains links to third party websites that are not under the control of Wowza Media Systems, LLC ("Wowza") and Wowza is not responsible for the content on any linked site. If you access a third party website mentioned in this document, then you do so at your own risk. Wowza provides these links only as a convenience, and the inclusion of any link does not imply that Wowza endorses or accepts any responsibility for the content on third party sites. Trademarks Wowza, Wowza Media Systems, Wowza Media Server and related logos are either registered trademarks or trademarks of Wowza Media Systems, LLC in the United States and/or other countries. Adobe and Flash are either registered trademarks or trademarks of Adobe Systems Incorporated in the United States and/or other countries. Microsoft and Silverlight are either registered trademarks or trademarks of Microsoft Corporation in the United States and/or other countries. QuickTime, iPhone, iPad and iPod touch are either registered trademarks or trademarks of Apple, Inc. in the United States and/or other countries. Other product names, logos, designs, titles, words or phrases mentioned may be third party registered trademarks or trademarks in the United States and/or other countries. -

Dual Marking Gauge
Dual Marking Gauge U.S. Des. Pat. No. D677,179 The Veritas® Dual Marking Gauge has two rods mounted eccentrically in the reference face. One rod has a non-rotating wheel cutter whose bevel faces the reference face (outside cutter) and the other has a non-rotating wheel cutter whose bevel faces away from it (inside cutter), allowing the gauge to be used in a wide range of applications. The hardened steel wheel cutters cut wood fi bers rather than tear them, and produce fi ne cut- lines, ideal for chisel registration. The most common use for this gauge would be as a mortise gauge for scribing both sides of a mortise. Unlike other mortise gauges, the cutters on the Veritas Dual Marking Gauge are used independently, scribing just one line at a time. As a result, this marking gauge can be used anywhere a project requires repeated marking of two dimensions. The individual wheel cutters can be completely retracted into the reference face, and the gauge can function as a single-cutter marking gauge. For most traditional uses, the outside cutter (bevel facing the reference face) would be used; however, for thicknessing a workpiece, the inside cutter (bevel facing away from the reference face) would be used. The eccentric confi guration of the rods maximizes the size of the reference surface, while maintaining the overall size of the gauge. The short side can also be used if space is restricted. As an added advantage, the eccentric nature means this gauge is much less likely to roll off the work surface. -

Build a Plane That Cuts Smooth and Crisp Raised Panels With, Against Or Across the Grain – the Magic Is in the Spring and Skew
Fixed-width PanelBY WILLARD Raiser ANDERSON Build a plane that cuts smooth and crisp raised panels with, against or across the grain – the magic is in the spring and skew. anel-raising planes are used Mass., from 1790 to 1823 (Smith may to shape the raised panels in have apprenticed with Joseph Fuller doors, paneling and lids. The who was one of the most prolific of the profile has a fillet that defines early planemakers), and another similar Pthe field of the panel, a sloped bevel example that has no maker’s mark. to act as a frame for the field and a flat Both are single-iron planes with tongue that fits into the groove of the almost identical dimensions, profiles door or lid frame. and handles. They differ only in the I’ve studied panel-raising planes spring angles (the tilt of the plane off made circa the late 18th and early 19th vertical) and skew of the iron (which centuries, including one made by Aaron creates a slicing cut across the grain to Smith, who was active in Rehoboth, reduce tear-out). The bed angle of the Smith plane is 46º, and the iron is skewed at 32º. Combined, these improve the quality of cut without changing the tool’s cutting angle – which is what happens if you skew Gauges & guides. It’s best to make each of these gauges before you start your plane build. In the long run, they save you time and keep you on track. Shaping tools. The tools required to build this plane are few, but a couple of them – the firmer chisel and floats – are modified to fit this design. -

Ellsworth American : August 17, 1876
Cbf £llsiP0rty Kates of Advertisi^f. Li ^nrriran lwk. Swltn. 3 mos. Omoi. I TV. 1 $160 00 $«00 $10 00 IB PCBLISBBD *T inch, $100 $4 3 inches. 3 CO 4 60 ON 15 00 25 0$ 0$ U T 4 column, 8 03 13 00 80 00 48 00 85 i: I.LSWO H, M E, 1 column. 14 0$ 22 00 50 00 86 0$ 100 00 BT TH* Special Notices. One square 3 weeks, $2.00 Each additional week, 50 cents iaacock County Publishing Co moan j Administrator’s and Kxeeutor’s Notices, 1 50 Citation from Probate Court, 8 uO Commissioner’s Notices, 2 8$ T«m« at Messenger’s and Assignee’s Notioti, t-00 SaburiylioB. Editorial Notices, per Tine, -1® Notices, *1® n« copy, n paid within three month*.•'^tK Obituary per line, No charge less than •*w i>»: within three month*,.. if st the end ©t the One inch space will constitute a square. paid year.2 j< Advertisements to be in advaoco. r*ill be discontinued nntil all Transient paid arrear No advertisements reconed less than a *re paid, except at the square. publisher** option— and Deaths inserted free. » person wishing his Marriages sad paper stopped, must to loti'-e thereof at the 1 early advertisers pay quarterly. ( expimtion of the tern • ictner previous notice has been given or not ME., THURSDAY, A.TTCHJST 17, 1870. ELLSWORTH, Tol. MlIdUM-No. 33. Imsiness It was not long after Hus I « (him; which Miss Moggaridge did with her •Aud when It Is all gone/ coutinued Miss expostulation through these Luke Moggaridge* that’1 her willing hands; by the calls of Master i|arbs. -

Marking and Cutting Gauges
Well Stocked Shop Multi-Marker If you’re constantly resetting your gauge to a single measurement, a 3-in-1 Brass Wheel Marking Gauge second gauge, like Lee Valley’s brass Marking Gauge #153490, $15.99 05N65.01, $24.50 3-in-1 gauge, may solve the problem. leevalley.com This gauge sports a head that you Marking and can outfit with a pin, knife, or blade, so you can select the cutter best suited to the task at hand. Cutting Gauges What I like best about this tool is its size. More than one way to make your mark woods. Filing a flat on one side of Like a 4" square, the pin can correct the tendency the compact gauge By Jeff Day to tear out, but your best bet is to fits neatly into my cuttingpartner gauge it with a cutting gauge. apron pocket so it’s With a knife-edged marker, a always in easy reach. Marking and excels at making M cutting gauges crisp, clean lines across the any years ago when I A pin-headed gauge is good grain. Compared to a pin- began tooling up my shop, I for establishing lines parallel scratched line, the cutline helps quickly discovered how much One of my first purchases to the grain, such as you’d need prevent splintering and tear- I could accomplish with basic was the markingonly member gauge of the when laying out hinges, grooves out, a handy attribute when hand tools. Though many were gauge family that is technically for drawer bottoms, rabbets, or chiseling dovetails at their antiques, it wasn’t long before called a due to the thickness of a board when baseline. -

Website Specifications 20130106
Wowza Media Server® 3.6 Technical Specifications Wowza Media Server® software delivers market-leading functionality, reliability, and flexibility for streaming to any screen across a wide range of industries. Streaming Delivery Adobe Flash® RTMP Flash Player Multi-Protocol, Multi (RTMPE, RTMPT, RTMPTE, RTMPS) Adobe® AIR® Client Adobe Flash HTTP Dynamic Streaming (HDS) RTMP-compatible players HDS-compatible players Apple® HTTP Live Streaming (HLS) iPhone®, iPod®, iPad® (iOS 3.0 or later) QuickTime® Player (10.0 or later) Safari® (4.0 or later on Mac OS X version 10.6) Roku® streaming devices and other HLS-compatible players MPEG DASH DASH-264 Compatible Players Microsoft® Smooth Streaming Silverlight® 3 or later RTSP/RTP Quicktime Player VideoLAN VLC media player 3GPP-compatible mobile devices Other RTSP/RTP-compliant players MPEG2 Transport Protocol (MPEG-TS) IPTV set-top boxes Live Streaming RTMP Video: H.264, VP6, Sorenson Spark®, Screen Video v1 & v2 Compatible Encoding Audio: AAC, AAC-LC, HE-AAC, MP3, Speex, NellyMoser ASAO Inputs RTSP/RTP Video: H.264, H.263 Audio: AAC, AAC-LC, HE-AAC, MP3, Speex MPEG-TS Video: H.264 Audio: AAC, AAC-LC, HE-AAC, E-AC-3, AC-3, MP3 ICY (SHOUTcast/Icecast) Audio: AAC, AAC-LC, HE-AAC (aacPlus), v1 & v2, MP3 Support File Formats Video and Audio FLV (Flash Video - .flv) MP4 (QuickTime container - .mp4, .f4v, .mov, .m4v, .mp4a, .3gp, and .3g2) MP3 (.mp3) PIFF (.ism, .ismc, .ismv, .isma) Protocols and Payloads RTSP IETF RFC2326 RTP:H.264 IETF RFC3984, QuickTime Generic RTP Payload Format RTP:AAC IETF RFC3640, -

Catheter Associated Urinary Tract Infection (CAUTI) Prevention
Catheter Associated Urinary Tract Infection (CAUTI) Prevention System CAUTI Prevention Team 1 Objectives At the end of this module, the participant will be able to: Identify risk factors for CAUTI Explain the relationship between catheter duration and CAUTI risk List the appropriate indications for urinary catheter insertion and continued use Implement evidence-based nursing practice to decrease the risk and incidence of CAUTI 2 The Problem All patients with an indwelling urinary catheter are at risk for developing a CAUTI. CAUTI increases pain and suffering, morbidity & mortality, length of stay, and healthcare costs. Appropriate indwelling catheter use can prevent about 400,000 infections and 9,000 deaths every year! (APIC, 2008; Gould et al, 2009) 3 2012 National Patient Safety Goal Implement evidence-based practices to prevent indwelling catheter associated urinary tract infections (CAUTI) Insert indwelling urinary catheters according to evidence-based guidelines Limit catheter use and duration Use aseptic technique for site preparation, equipment, and supplies (The Joint Commission (TJC), 2011) 4 2012 National Patient Safety Goal Manage indwelling urinary catheters according to evidence-based guidelines Secure catheters for unobstructed urine flow and drainage Maintain the sterility of the urine collection system Replace the urine collection system when required Collect urine samples using aseptic technique (TJC, 2011) 5 Sources of CAUTI Microorganisms Endogenous Meatal, rectal, or vaginal colonization Exogenous -

Marking Gauge
Online Extra accurate layouts with a Marking Gauge When it comes to fast and accurate layouts, this traditional tool will more than earns its keep in the woodworking shop. Thumb If I were to make a list of the If you take a look at the various the amount of brass details used screw most-used tools in my shop, the marking gauges being sold today, in the construction. The more marking gauge would be you’ll notice two distinct types. expensive gauges have brass thumb near the top. Even with the Some use a steel pin to scribe a line myriad of rulers, calipers, while others use a flat blade. This and digital measuring second type is often called a “cut- devices that are available ting gauge” because the blade slices today, it’s hard to beat this the wood fibers rather than tearing simple tool for accuracy them, like the pin-style marking and ease of use. gauges (see photos at right). Of the two, I prefer the blade-style gauge. Blade Wedge It scores a cleaner, crisper line. DESIGN. A marking gauge is one of those simple tools whose basic design hasn’t changed much over the years. It has a beam and an adjustable fence (or stock) that is Brass wear strip held in place with a thumb screw, or sometimes, a wedge. Fence The only other differences you’re (or stock) Beam likely to find between the various { A marking gauge (top) tears gauges on the market have to do its way across the wood, while with the level of fit and finish and a cutting gauge scores a line. -

Caring for Your Urinary (Foley) Catheter
Caring for Your Urinary (Foley) Catheter This information will help you care for your urinary (Foley) catheter while you’re at home. You have had a urinary catheter (a thin, flexible tube) placed in your bladder to drain your urine (pee). It’s held inside your bladder by a balloon filled with water. The parts of the catheter outside your body are shown in Figure 1. Catheter Care ● You need to clean your catheter, change your drainage bags, and wash your drainage bags every day. ● You may see some blood or urine around where the catheter enters your body, especially when walking or having a bowel movement. This is normal, as long as there’s urine draining into the drainage bag. If there’s not, call your healthcare provider. ● While you have your catheter, drink 1 to 2 glasses of liquids every 2 hours while you’re awake. ● Make sure that the catheter is in place in a tension free manner. The catheter should not be tight and should sit loosely. Showering ● You can shower while you have your catheter in place. Don’t take a bath until after your catheter is removed. ● Make sure you always shower with your night bag. Don’t shower with your leg bag. You may find it easier to shower in the morning. Cleaning Your Catheter You can clean your catheter while you’re in the shower. You will need the following supplies: 1. Gather your supplies. You will need: ○ Mild soap ○ Water 2. Wash your hands with soap and water for at least 20 seconds. -
Jointing Sharpening Now Observe How the Clock
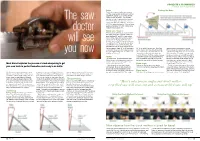
PROJECTS & TECHNIQUES Product tech – saw doctor PHOTOGRAPHS BY MARK HARRELL Rake Finding the Rake Rake is the degree of offset from vertical, and this angle governs whether you want an aggressive, ripping cut, or a clean, slower crosscut. Note the angle – we generally set rake for a rip filing somewhere between The saw 0° to 8°. Establish rake closer to zero for aggressive ripping in softwoods, and closer to 10° for dense hardwoods. Crosscut filings generally mandate 15° to 20°. Hybrid-filing finds the sweet spot at 10°. Bevel (aka ‘fleam’) doctor Bevel indicates whether you desire to knife the cutting edge of a sawtooth. Little to no bevel (between 0° and 8°), is best suited for rip filings. Again, the rule here is select closer to 0° for ripping softwoods, and gravitate closer to 8° for ripping hardwoods. will see I usually find that 5° for dedicated rip either way delivers a crisp, assertive action, and mitigates tear-out on the far side of the cut. As for crosscut filings, 15° to 20° delivers a 20° is the perfect bevel angle.” Don’t buy and somewhere in between for hybrid. clean, knife-like action when sawing across into it. Anyone who says they consistently Here’s why precise angles just don’t matter: the grain. Hybrid-filing finds the sweet spot hit a certain degree standard when hand- a rip-filed saw will crosscut, and a crosscut- you now for both at 10° to 12°. sharpening a saw is full of it. Again, the filed saw will rip. The point is, any properly important thing isn’t hitting a certain degree. -

A Single-Chip MPEG-2 Codec Based on Customizable Media Embedded Processor
530 IEEE JOURNAL OF SOLID-STATE CIRCUITS, VOL. 38, NO. 3, MARCH 2003 A Single-Chip MPEG-2 Codec Based on Customizable Media Embedded Processor Shunichi Ishiwata, Tomoo Yamakage, Yoshiro Tsuboi, Takayoshi Shimazawa, Tomoko Kitazawa, Shuji Michinaka, Kunihiko Yahagi, Hideki Takeda, Akihiro Oue, Tomoya Kodama, Nobu Matsumoto, Takayuki Kamei, Mitsuo Saito, Takashi Miyamori, Goichi Ootomo, and Masataka Matsui, Member, IEEE Abstract—A single-chip MPEG-2 MP@ML codec, integrating microprocessors, such as out-of-order speculative execution, P 3.8M gates on a 72-mm die, is described. The codec employs a branch prediction, and circuit technologies to achieve high heterogeneous multiprocessor architecture in which six micropro- clock frequency, are unsuitable for these application-specific cessors with the same instruction set but different customization execute specific tasks such as video and audio concurrently. processors. On the other hand, the addition of application-spe- The microprocessor, developed for digital media processing, cific instructions and/or hardware engines to accelerate heavy provides various extensions such as a very-long-instruction-word iteration of relatively simple tasks often results in a large gain coprocessor, digital signal processor instructions, and hardware in performance at little additional cost, especially in DSP ap- engines. Making full use of the extensions and optimizing the plications. A heterogeneous multiprocessor architecture using architecture of each microprocessor based upon the nature of specific tasks, the chip can execute not only MPEG-2 MP@ML simple and small microprocessors achieves a better cost–per- video/audio/system encoding and decoding concurrently, but also formance tradeoff than a single high-end general-purpose MPEG-2 MP@HL decoding in real time.