HQ-2019-1340.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NSG 604 Indicators and Signs
This is an uncontrolled copy. Before use, make sure that this is the current version by visiting www.railsafe.org.au/nsg NSG 604 signals and signs Indicators and signs General To describe the types of indicators and signs used in the Network. ............................................................................................... NOTE The Figures in this Rule show examples of the indicators and signs used in the Network. White or lunar white lights are shown in blue . ............................................................................................... Clearance posts Clearance posts may be located between two converging lines to show the clearance limit. Some clearance posts have: • a reflective background, or • a white light that must be illuminated at night or in conditions of low visibility. White reflective post forms Illuminated post form FIGURE 1: Examples of clearance posts ............................................................................................... NETWORK RULES MARCH 2019 V10.0 © SYDNEY TRAINS 2019 PAGE 1 OF 38 This is an uncontrolled copy. Before use, make sure that this is the current version by visiting www.railsafe.org.au/nsg NSG 604 signals and signs Indicators and signs Dead end lights Dead end lights are small red lights to indicate the end of dead end sidings. The lights display STOP indications only. If it is possible for a dead end light to be mistaken as a running signal at STOP, a white light above the red light is used to distinguish it from a running signal. FIGURE 2: Examples of dead end lights ............................................................................................... NETWORK RULES MARCH 2019 V10.0 © SYDNEY TRAINS 2019 PAGE 2 OF 38 This is an uncontrolled copy. Before use, make sure that this is the current version by visiting www.railsafe.org.au/nsg NSG 604 signals and signs Indicators and signs Guard’s indicator If it is possible for the signal at the exit-end of a platform to be obscured from a Guard’s view, a Guard’s indicator is placed over the platform. -

RAIB Report: Freight Train Derailment at Angerstein Junction on 3 June 2015
Oliver Stewart Senior Executive, RAIB Relationship and Recommendation Handling Telephone 020 7282 3864 E-mail [email protected] 4 June 2020 Mr Andrew Hall Deputy Chief Inspector of Rail Accidents Cullen House Berkshire Copse Rd Aldershot Hampshire GU11 2HP Dear Andrew, RAIB Report: Freight train derailment at Angerstein Junction on 3 June 2015 I write to provide an update1 on the action taken in respect of recommendation 3 addressed to ORR in the above report, published on 1 June 2016. The annex to this letter provides details of the action taken regarding the recommendation. The status of recommendation 3 is ‘Implemented’. We do not propose to take any further action in respect of the recommendation, unless we become aware that any of the information provided has become inaccurate, in which case I will write to you again. We will publish this response on the ORR website on 5 June 2020. Yours sincerely, Oliver Stewart 1 In accordance with Regulation 12(2)(b) of the Railways (Accident Investigation and Reporting) Regulations 2005 Annex A Recommendation 3 The intent of this recommendation is to ensure that the derailment risk at Angerstein Junction is adequately controlled. Network Rail should review and, if appropriate, alter the infrastructure configuration on the line between Angerstein Junction and Angerstein Wharf sidings to reduce its contribution to the derailment risk in the immediate vicinity of the 851A trap points. This review should include, but not be limited to, consideration of: • the wagon types and loads normally using the line; • the layout of the check rail; • the speed and braking profiles of trains using the line; • the locations and operation of signalling equipment; and • the location of the trap points, or the provision of alternative risk mitigation measures ORR decision 1. -

Federal Railroad Administration Office of Safety Headquarters Assigned Accident Investigation Report HQ-2006-24 CSX Transportati
Federal Railroad Administration Office of Safety Headquarters Assigned Accident Investigation Report HQ-2006-24 CSX Transportation (CSX) Richmond, Virginia April 22, 2006 Note that 49 U.S.C. §20903 provides that no part of an accident or incident report made by the Secretary of Transportation/Federal Railroad Administration under 49 U.S.C. §20902 may be used in a civil action for damages resulting from a matter mentioned in the report. DEPARTMENT OF TRANSPORTATION FRA FACTUAL RAILROAD ACCIDENT REPORT FRA File # HQ-2006-24 FEDERAL RAILROAD ADMINISTRATION 1.Name of Railroad Operating Train #1 1a. Alphabetic Code 1b. Railroad Accident/Incident No. CSX Transportation [CSX ] CSX R000022015 2.Name of Railroad Operating Train #2 2a. Alphabetic Code 2b. Railroad Accident/Incident N/A N/A N/A 3.Name of Railroad Responsible for Track Maintenance: 3a. Alphabetic Code 3b. Railroad Accident/Incident No. CSX Transportation [CSX ] CSX N/A 4. U.S. DOT_AAR Grade Crossing Identification Number 5. Date of Accident/Incident 6. Time of Accident/Incident Month Day Year 04 22 2006 05:19:00 AM PM 7. Type of Accident/Indicent 1. Derailment 4. Side collision 7. Hwy-rail crossing 10. Explosion-detonation 13. Other (single entry in code box) 2. Head on collision 5. Raking collision 8. RR grade crossing 11. Fire/violent rupture (describe in narrative) 3. Rear end collision 6. Broken Train collision 9. Obstruction 12. Other impacts 01 8. Cars Carrying 9. HAZMAT Cars 10. Cars Releasing 11. People 12. Division HAZMAT Damaged/Derailed HAZMAT Evacuated 0 0 0 0 FLORENCE 13. Nearest City/Town 14. -
Rtd Light Rail Design Criteria
RTD LIGHT RAIL DESIGN CRITERIA Regional Transportation District November 2005 Prepared by the Engineering Division of the Regional Transportation District Regional Transportation District 1600 Blake Street Denver, Colorado 80202-1399 303.628.9000 RTD-Denver.com November 28, 2005 The RTD Light Rail Design Criteria Manual has been developed as a set of general guidelines as well as providing specific criteria to be employed in the preparation and implementation of the planning, design and construction of new light rail corridors and the extension of existing corridors. This 2005 issue of the RTD Light Rail Design Criteria Manual was developed to remain in compliance with accepted practices with regard to safety and compatibility with RTD's existing system and the intended future systems that will be constructed by RTD. The manual reflects the most current accepted practices and applicable codes in use by the industry. The intent of this manual is to establish general criteria to be used in the planning and design process. However, deviations from these accepted criteria may be required in specific instances. Any such deviations from these accepted criteria must be approved by the RTD's Executive Safety & Security Committee. Coordination with local agencies and jurisdictions is still required for the determination and approval for fire protection, life safety, and security measures that will be implemented as part of the planning and design of the light rail system. Conflicting information or directives between the criteria set forth in this manual shall be brought to the attention of RTD and will be addressed and resolved between RTD and the local agencies andlor jurisdictions. -

LNW Route Specification 2017
Delivering a better railway for a better Britain Route Specifications 2017 London North Western London North Western July 2017 Network Rail – Route Specifications: London North Western 02 SRS H.44 Roses Line and Branches (including Preston 85 Route H: Cross-Pennine, Yorkshire & Humber and - Ormskirk and Blackburn - Hellifield North West (North West section) SRS H.45 Chester/Ellesmere Port - Warrington Bank Quay 89 SRS H.05 North Transpennine: Leeds - Guide Bridge 4 SRS H.46 Blackpool South Branch 92 SRS H.10 Manchester Victoria - Mirfield (via Rochdale)/ 8 SRS H.98/H.99 Freight Trunk/Other Freight Routes 95 SRS N.07 Weaver Junction to Liverpool South Parkway 196 Stalybridge Route M: West Midlands and Chilterns SRS N.08 Norton Bridge/Colwich Junction to Cheadle 199 SRS H.17 South Transpennine: Dore - Hazel Grove 12 Hulme Route Map 106 SRS H.22 Manchester Piccadilly - Crewe 16 SRS N.09 Crewe to Kidsgrove 204 M1 and M12 London Marylebone to Birmingham Snow Hill 107 SRS H.23 Manchester Piccadilly - Deansgate 19 SRS N.10 Watford Junction to St Albans Abbey 207 M2, M3 and M4 Aylesbury lines 111 SRS H.24 Deansgate - Liverpool South Parkway 22 SRS N.11 Euston to Watford Junction (DC Lines) 210 M5 Rugby to Birmingham New Street 115 SRS H.25 Liverpool Lime Street - Liverpool South Parkway 25 SRS N.12 Bletchley to Bedford 214 M6 and M7 Stafford and Wolverhampton 119 SRS H.26 North Transpennine: Manchester Piccadilly - 28 SRS N.13 Crewe to Chester 218 M8, M9, M19 and M21 Cross City Souh lines 123 Guide Bridge SRS N.99 Freight lines 221 M10 ad M22 -
UPRR - General Code of Operating Rules
Union Pacific Rules UPRR - General Code of Operating Rules Seventh Edition Effective April 1, 2020 Includes Updates as of September 28, 2021 PB-20280 1.0: GENERAL RESPONSIBILITIES 2.0: RAILROAD RADIO AND COMMUNICATION RULES 3.0: Section Reserved 4.0: TIMETABLES 5.0: SIGNALS AND THEIR USE 6.0: MOVEMENT OF TRAINS AND ENGINES 7.0: SWITCHING 8.0: SWITCHES 9.0: BLOCK SYSTEM RULES 10.0: RULES APPLICABLE ONLY IN CENTRALIZED TRAFFIC CONTROL (CTC) 11.0: RULES APPLICABLE IN ACS, ATC AND ATS TERRITORIES 12.0: RULES APPLICABLE ONLY IN AUTOMATIC TRAIN STOP SYSTEM (ATS) TERRITORY 13.0: RULES APPLICABLE ONLY IN AUTOMATIC CAB SIGNAL SYSTEM (ACS) TERRITORY 14.0: RULES APPLICABLE ONLY WITHIN TRACK WARRANT CONTROL (TWC) LIMITS 15.0: TRACK BULLETIN RULES 16.0: RULES APPLICABLE ONLY IN DIRECT TRAFFIC CONTROL (DTC) LIMITS 17.0: RULES APPLICABLE ONLY IN AUTOMATIC TRAIN CONTROL (ATC) TERRITORY 18.0: RULES APPLICABLE ONLY IN POSITIVE TRAIN CONTROL (PTC) TERRITORY GLOSSARY: Glossary For business purposes only. Unauthorized access, use, distribution, or modification of Union Pacific computer systems or their content is prohibited by law. Union Pacific Rules UPRR - General Code of Operating Rules 1.0: GENERAL RESPONSIBILITIES 1.1: Safety 1.1.1: Maintaining a Safe Course 1.1.2: Alert and Attentive 1.1.3: Accidents, Injuries, and Defects 1.1.4: Condition of Equipment and Tools 1.2: Personal Injuries and Accidents 1.2.1: Care for Injured 1.2.2: Witnesses 1.2.3: Equipment Inspection 1.2.4: Mechanical Inspection 1.2.5: Reporting 1.2.6: Statements 1.2.7: Furnishing Information -
Derail Pockets for Interlocking of Crossing at Joint Passenger Station
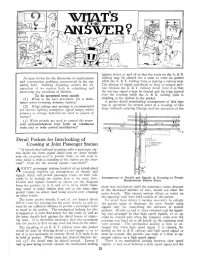
against levers 21 and 16 so that the route on the A. & B. An open forum for the discussion of maintenance railway may be cleared for a train to enter its pocket and construction problems encountered in the sig while the X. & Y. railway train is making a station stop. naling field. Railway Signaling solicits the co The placing of signal and.derail 21 back to normal posi operation of its readers both in submitting and tion releases the X. & Y. railway derail lever 8,$.0 that answering any questions of interest. the starting signal 9 may be cleared and the tritir 'moved tr~in To be -answered next month over the crossing while the A. & B. railway - is (1) What is the best procedure for a mam standing at the station in the pocket. .. , .. tainer when renewing primary battery? A pocket derail interlocking arrangement of this tYpe (2) What voltage and wattag-e is recommended was in operation for several years at a crossing of two for electric lighting semaphore signal lamps, where large railroads entering Chicago and the operation of the primary 0'1' storage batteries are used as fource of energy'! 9 10 (3) What circuits a-re used to control the recur II If! rent acknowledgment loop feeds on contmuous S I~ itl x .. y Rv "-!"- train stop or train control installations? J '"U4 I IJVIJ ~e /8 17 r 1C"!15 I I' Derail Pockets for Interlocking of passenger Crossing at Joint Passenger Station D1t.slot/on "At interlocked railroad crossings with a passenger sta ~ tion inside the home signal limits how are inller derails '".. -

TCQSM Part 8
Transit Capacity and Quality of Service Manual—2nd Edition PART 8 GLOSSARY This part of the manual presents definitions for the various transit terms discussed and referenced in the manual. Other important terms related to transit planning and operations are included so that this glossary can serve as a readily accessible and easily updated resource for transit applications beyond the evaluation of transit capacity and quality of service. As a result, this glossary includes local definitions and local terminology, even when these may be inconsistent with formal usage in the manual. Many systems have their own specific, historically derived, terminology: a motorman and guard on one system can be an operator and conductor on another. Modal definitions can be confusing. What is clearly light rail by definition may be termed streetcar, semi-metro, or rapid transit in a specific city. It is recommended that in these cases local usage should prevail. AADT — annual average daily ATP — automatic train protection. AADT—accessibility, transit traffic; see traffic, annual average ATS — automatic train supervision; daily. automatic train stop system. AAR — Association of ATU — Amalgamated Transit Union; see American Railroads; see union, transit. Aorganizations, Association of American Railroads. AVL — automatic vehicle location system. AASHTO — American Association of State AW0, AW1, AW2, AW3 — see car, weight Highway and Transportation Officials; see designations. organizations, American Association of State Highway and Transportation Officials. absolute block — see block, absolute. AAWDT — annual average weekday traffic; absolute permissive block — see block, see traffic, annual average weekday. absolute permissive. ABS — automatic block signal; see control acceleration — increase in velocity per unit system, automatic block signal. -

Finished Vehicle Logistics by Rail in Europe
Finished Vehicle Logistics by Rail in Europe Version 3 December 2017 This publication was prepared by Oleh Shchuryk, Research & Projects Manager, ECG – the Association of European Vehicle Logistics. Foreword The project to produce this book on ‘Finished Vehicle Logistics by Rail in Europe’ was initiated during the ECG Land Transport Working Group meeting in January 2014, Frankfurt am Main. Initially, it was suggested by the members of the group that Oleh Shchuryk prepares a short briefing paper about the current status quo of rail transport and FVLs by rail in Europe. It was to be a concise document explaining the complex nature of rail, its difficulties and challenges, main players, and their roles and responsibilities to be used by ECG’s members. However, it rapidly grew way beyond these simple objectives as you will see. The first draft of the project was presented at the following Land Transport WG meeting which took place in May 2014, Frankfurt am Main. It received further support from the group and in order to gain more knowledge on specific rail technical issues it was decided that ECG should organise site visits with rail technical experts of ECG member companies at their railway operations sites. These were held with DB Schenker Rail Automotive in Frankfurt am Main, BLG Automotive in Bremerhaven, ARS Altmann in Wolnzach, and STVA in Valenton and Paris. As a result of these collaborations, and continuous research on various rail issues, the document was extensively enlarged. The document consists of several parts, namely a historical section that covers railway development in Europe and specific EU countries; a technical section that discusses the different technical issues of the railway (gauges, electrification, controlling and signalling systems, etc.); a section on the liberalisation process in Europe; a section on the key rail players, and a section on logistics services provided by rail. -

Tampa Bay's Railroad History
Tampa Bay’s RailRoad HisToRy all aboard: Tampa Bay’s railroad history Silvery-sleek, on sun-bleached tracks With barrel-chested engines, Dolomite black “Those were the trains of yesterday! “ But where might smoke and thunder stay? 71st New York Where might great metro-liners rest, Volunteers arrive in Port Tampa, As they rumble ’cross-the-country with their smoke-filled crests? 1898, courtesy USF Library from The Epic of Tampa Union Station Special Collections by James E. Tokley Sr., Hillsborough County Poet Laureate Sanford-St. Petersburg train, 1893, courtesy Tampa-Hillsborough County Public Library System Henry Plant supervising the transport of Army troops by railroad to Tampa, where they boarded ships to fight the Spanish-American War in Cuba, 1898; Tampa Bay Times photo Newspaper in Education NIE staff LAFS.4-5.L.1.2; LAFS.4-5.L.1.3; LAFS.4-5.L.1.4; LAFS.4-5.L.1.5; LAFS.4- The Tampa Bay Times Newspaper in Jodi Pushkin, manager, [email protected] 5.L.1.6 Education (NIE) program is a cooperative Sue Bedry, development specialist, [email protected] effort between schools and the Times Hillsborough County Historic Preservation Challenge Grant to encourage the use of newspapers in © Tampa Bay Times 2014 This project was supported by a Historic Preservation Challenge Grant print and electronic form as educational awarded by the Hillsborough County Board of County Commissioners. The resources. Credits Hillsborough County Historic Preservation program aims to foster planning Our educational resources fall Researched and written by Jodi Pushkin and Sue Bedry, Tampa Bay Times that “encourages the continued use and preservation of historic sites and into the category of informational Designed by Stacy Rector, Fluid Graphic Design LLC structures.” The Historic Preservation Challenge Grant program was founded in text. -
Indication Locking Test
ONLY Inspection and Maintenance of Interlockings Course 206 PREVIEWPARTICIPANT GUIDE COURSE 206: INSPECTION AND MAINTENANCE OF INTERLOCKINGS MODULE 1: OVERVIEW & SAFETY Inspection and Maintenance of Interlockings Participant Guide Signals Maintenance Training Consortium COURSE 206 ONLY PREVIEW DRAFT ● Intended For Use by Transit Elevator/Escalator Consortium Members Only Page i COURSE 206: INSPECTION AND MAINTENANCE OF INTERLOCKINGS MODULE 1: OVERVIEW & SAFETY TABLE OF CONTENTS PAGE How to Use the Participant Guide .................................................................................................... V MODULE 1 OVERVIEW AND SAFETY ................................................................................1 1-1 OVERVIEW ......................................................................................................................2 1-2 SAFETY ............................................................................................................................3 1-3 TOOLS AND MATERIALS .............................................................................................7 1-4 TESTING .........................................................................................................................10 1-5 DOCUMENTATION ......................................................................................................15 1-6 SUMMARY .....................................................................................................................16 MODULE 2 TESTING & MAINTENANCE OF INTERLOCKINGSONLY -

634 Part 236—Rules, Standards, And
Pt. 235, App. A 49 CFR Ch. II (10–1–07 Edition) (d) The protestant shall certify that EFFECTIVE DATE NOTE: At 49 FR 3380, Jan. service of a copy of its protest was 26, 1984, part 235 was revised. This section made upon each applicant. contains information collection and record- (e) Request for hearing must be ac- keeping requirements and will not become companied with a showing why the effective until approval has been given by protestant is unable to properly the Office of Management and Budget. present his or her position by written statements. APPENDIX A TO PART 235—SCHEDULE OF CIVIL PENALTIES1 Willful viola- Section Violation tion 235.5 Changes requiring filing of application $5,000 $7,500 [53 FR 52936, Dec. 29, 1988, as amended at 69 FR 62818, Oct. 28, 2004] PART 236—RULES, STANDARDS, 236.13 Spring switch; selection of signal con- trol circuits through circuit controller. AND INSTRUCTIONS GOVERNING 236.14 Spring switch signal protection; re- THE INSTALLATION, INSPECTION, quirements. MAINTENANCE, AND REPAIR OF 236.15 Timetable instructions. SIGNAL AND TRAIN CONTROL 236.16 Electric lock, main track releasing SYSTEMS, DEVICES, AND APPLI- circuit. 236.17 Pipe for operating connections, re- ANCES quirements. 236.18 Software management control plan. Sec. 236.0 Applicability, minimum requirements, ROADWAY SIGNALS AND CAB SIGNALS and penalties. 236.21 Location of roadway signals. 236.22 Semaphore signal arm; clearance to Subpart A—Rules and Instructions: All other objects. Systems 236.23 Aspects and indications. 236.24 Spacing of roadway signals. GENERAL 236.25 [Reserved] 236.1 Plans, where kept.