Physiology of Adventure Racing – with Emphasis on Circulatory Response and Cardiac Fatigue
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

I Love to Challenge Myself
Kim Collison: I love to challenge myself I am passionate about running and off-road in particular. Fell, trail, ultra - all of them. I guess my main passion is mountains. Being out in nature and exploring comes into it too. I am quite competitive. The race element comes right to the fore for me. I love to challenge myself. Kim Collison attempts to summarise his passion for being out in the mountains. I talked to him just after he had set a new winter Bob Graham Round record this December. He went on to explain his background and how he got into his sport, whilst also giving details of that impressive winter effort. Kim Collison is not a native of Cumbria, although he has lived there for a while now. He grew up in Tring, in Hertfordshire, and ended up at Tring Running Club. His father was interested in sports and in running in particular. Kim enjoyed running from a very early age. As a young kid he was always outside playing. At Secondary School, Hemel Hempstead School, he did a bit of cross country, but says he wasn't so good at team games. ‘One year I remember not getting in the school cross country team’, he recalls, ‘and then going on and winning all the PE lesson cross countries the next year. I was that driven and competitive. I didn't stand out at County level or anything mind.’ He was in the Scouts and did a lot of hiking in the mountains. Through this he was learning navigation, being taken to the Lakes and Snowdonia. -
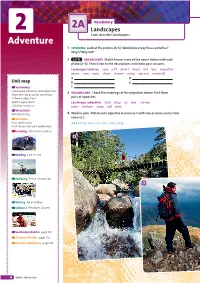
Adventure 1 Speaking Look at the Photos (A–E)
2A Vocabulary 2 Landscapes I can describe landscapes. Adventure 1 speaking Look at the photos (A–E). Would you enjoy these activities? Why? / Why not? 2 1.15 vocabulary Match two or more of the nouns below with each photo (A–E). Then listen to the descriptions and check your answers. Landscape: features cave cliff desert forest hill lake mountain ocean river rocks shore stream valley volcano waterfall A D Unit map B E Vocabulary C Landscape: features and adjectives 3 vocabulary Check the meanings of the adjectives below. Find three Adjectives to describe adventure Extreme adjectives pairs of opposites. Sports equipment Landscape: adjectives dark deep icy low narrow Outdoor activities rocky shallow steep tall wide Word Skills Word building 4 Work in pairs. Match each adjective in exercise 3 with two or more nouns from exercise 2. Grammar Past continuous dark forest, dark cave, dark valley; deep … Past simple and past continuous Listening Adrenaline junkies A Reading Lost at sea Speaking Photo description B Writing An invitation Culture 2 Robinson Crusoe Vocabulary Builder page 118 Grammar Builder page 126 Grammar Reference page 127 18 Unit 2 Adventure Sol3rdEd Inter Pre-Int SB.indb 18 22/09/2016 09:38 2A 5 1.16 Listen to four adverts. Match three of them with RECYCLE! There is and There are photos A–E. We use There’s … for singular countable nouns and 1 2 3 4 uncountable nouns. We use There are … for plural nouns. There’s a forest. There are trees. There’s (some) snow. 6 1.16 Listen again. -

A Kite Surfing Scenario
Biomechanics of extreme sports – a kite surfing scenario Lina Lundgren 1, Sofia Olandersson 1, Marita Hilliges 1, Anna-Lisa Osvalder 2 1Product Development in Healthcare, PRODEA research group, Halmstad University, Halmstad, Sweden Email: [email protected] 2 Department of Product- and Production Development, Division of Design Chalmers University of Technology, Gothenburg, Sweden Do extreme sports contribute to higher biomechanical stress compared to other sports? Kite surfing is one of the upcoming popular extreme sports, where very few have studied the mechanical forces that act on the body. There are several factors that contribute to mechanical stress, and for preventing injuries it is of interest to investigate how these forces affect the body and how we can develop the equipment and prepare the athletes for making it as safe as possible. This project will study injury prevalence, motion analysis and mapping of forces and pressure during kite surfing. The outcome will be a better understanding of biomechanics of kite surfing and a construction for testing and training. biomechanics, kite surfing, injuries, muscle strength, motion analysis 1 Introduction Extreme sports are becoming more and more popular, and since these sports often are associated with higher risks than other sports (Slanger, Rudestam, 1997), it is also possible that the biomechanical stress is higher and contributes to more injuries. Kite surfing is a water sport where the practitioner goes on water with a board through the power of a kite 25 meters up in the air. The kite is attached to the body via a Force from harness around the waist or hip (see Fig. -

8 Must See Gear Items Remembering Dave Boyd
Showdown In The Land Of Fire by Nathan Ward Out Of The Office And Into The 2008 USARA National The Wild Championship 8 Must See Gear Items Plus • Czech Adventure Race Remembering Dave Boyd • Trinidad Coast to Coast • Taking a Bearing DecemberAdventure World Magazine 2008 is a GreenZine 1 Maybe you snowshoe. Explore the narrows. Or chance the rapids. However you define your love of the outdoors, we define ours by supporting grassroots conservation efforts to protect North America’s wildest places. Hunter Shotwell dedicated his life to Castleton Tower. Surely, you can dedicate an hour to yours. AdventureQMPPMSRTISTPI World Magazine December 20083RILSYVE[IIO1EOIMXLETTIR www.conservationalliance.com2 contents Features 14 Remembering Dave Boyd 18 Showdown in the Land of Fire by Nathan Ward 26 BG US Challenge Out of the Office and Into the Wild 29 Czech Adventure Race Departments 37 2008 USARA National 45 Training Championship Adventure Racing Navigation Part 5: Taking A Bearing Trinidad Coast to Coast 52 57 Gear Closet 4 Editor’s Note 5 Contributors 7 News From the Field 13 Race Director Profile Cover Photo: Patagonia Expedition Race 33 Athlete Profile Photo by Nathan Ward 34 Where Are They Now? This Page: Abu Dhabi Adventure Challenge 2008 63 It Happened To Me Photo by Monica Dalmasso editor’s note Adventure World magazine Editor-in-Chief Clay Abney Managing Editor Dave Poleto Contributing Writers Jacob Thompson • Kip Koelsch Jan Smolík • Nathan Ward Troy Farrar • Andrea Dahlke Mark Manning • Tom Smith Tim Holmstrom Contributing Photographers Will Ramos • Monica Dalmasso Nathan Ward • Tim Holmstrom James O’Connor • Jiri Struk Glennon Simmons Adventure World Magazine is dedicated to the preservation our natural resources Sunset on Tobago --- after the Trinidad Coast to Coast by producing a GreenZine. -

Mountain Bike Performance and Recreation
sports and exercise medicine ISSN 2379-6391 http://dx.doi.org/10.17140/SEMOJ-SE-1-e001 Open Journal Special Edition “Mountain Bike Performance Mountain Bike Performance and and Recreation” Recreation Editorial Paul W. Macdermid, PhD* *Corresponding author Paul W. Macdermid, PhD Lecturer College of Health, School of Sport and Exercise, Massey University, Palmerston North, New College of Health Zealand School of Sport and Exercise Massey University Private Bag 11-222, Palmerston North 4474, New Zealand 1 The recreational activity of riding a bicyle off-road is very popular, and consequently Tel. +64 6 951 6824 2 E-mail: [email protected] a major contributor to tourism across the globe. As such the label accorded to the activity (“Mountain Biking (MTB)”), presents the image of an extreme sport. For many, this presents a Special Edition 1 picture of highly drilled and trained athletes performing gymnastic like tricks; hurtling down- Article Ref. #: 1000SEMOJSE1e001 hill at speeds >70 km/h (Downhill racing) or negotiating a short lap numerous times (Country Racing), to prove ascendancy over an opponent(s). For the majority of consumers/participants the French term “Velo Tout Terrain (VTT)” is a better decriptor and indicates the fact that the Article History bicycle is being purchased to ride on all terrain surfaces and profiles, by a diverse range of rd Received: August 23 , 2016 participants. Nevertheless, just like the world of motor car racing, technological development, rd Accepted: August 23 , 2016 physical understanding and skill development focuses on the very small percentage at the top of rd Published: August 23 , 2016 the pyramid in order to increase media exposure. -

Xc Ski Racing Plus
XC SKI RACING PLUS XC ski racing is fun… right? Well, what about ski racing with your brain turned on? That’s ski orienteering! What’s the difference? In xc skiing, the course is marked to tell you where to go – just apply the horsepower. In Ski-O, you still have to apply the horsepower, but you have to decide where to go while doing it. How does it work? At the start, you’re given a map of your course, like the map shown here. The pink circles represent control points that you must visit, in the right order, as fast as you can. The solid lines are wide, skateable trails, and dashed lines are narrower trails where you can only double pole. Knowing your relative strength as a skier affects your route choices – how would YOU go from #10 to #11 on this map? What do you do at the controls? At each control, there is a flag to mark the spot. To record that you’ve been there, you “punch” with an electronic recording device, worn on your finger. It makes a beep, and when you finish, the officials download the data from your finger stick and give you instant Equipment: results and your splits between all To carry your map, you use a map holder that mounts to controls. your chest, so that the map is always right in front of you, and can be rotated to align it with the direction you’re skiing. Races are freestyle, so most skiers use race skate skis. Poles are modified to have larger baskets to deal with the soft snow on narrow trails. -
007: the World Is Not Enough 1080 Teneighty Snowboarding a Bug's
007: The World Is Not Enough 1080 TenEighty Snowboarding A Bug's Life Aerofighter Assault AeroGauge Aidyn Chronicles : The First Mage All Star Tennis 99 All-Star Baseball 2000 All-Star Baseball 2001 All-Star Baseball 99 Armorines - Project S.W.A.R.M. Army Men : Air Combat Army Men : Sarge's Heroes Army Men : Sarge's Heroes 2 Asteroids Hyper 64 Automobili Lamborghini Banjo-Kazooie Banjo-Tooie Bassmasters 2000 Batman Beyond : Return of the Joker BattleTanx BattleTanx - Global Assault Battlezone : Rise of the Black Dogs Beetle Adventure Racing! Big Mountain 2000 Bio F.R.E.A.K.S. Blast Corps Blues Brothers 2000 Body Harvest Bomberman 64 Bomberman 64 : The Second Attack! Bomberman Hero Bottom of the 9th Brunswick Circuit Pro Bowling Buck Bumble Bust-A-Move '99 Bust-A-Move 2: Arcade Edition California Speed Carmageddon 64 Castlevania Castlevania : Legacy of Darkness Chameleon Twist Chameleon Twist 2 Charlie Blast's Territory Chopper Attack Clay Fighter : Sculptor's Cut Clay Fighter 63 1-3 Command & Conquer Conker's Bad Fur Day Cruis'n Exotica Cruis'n USA Cruis'n World CyberTiger Daikatana Dark Rift Deadly Arts Destruction Derby 64 Diddy Kong Racing Donald Duck : Goin' Qu@ckers*! Donkey Kong 64 Doom 64 Dr. Mario 64 Dual Heroes Duck Dodgers Starring Daffy Duck Duke Nukem : Zero Hour Duke Nukem 64 Earthworm Jim 3D ECW Hardcore Revolution Elmo's Letter Adventure Elmo's Number Journey Excitebike 64 Extreme-G Extreme-G 2 F-1 World Grand Prix F-Zero X F1 Pole Position 64 FIFA 99 FIFA Soccer 64 FIFA: Road to World Cup 98 Fighter Destiny 2 Fighters -

Flowers Racing
Salesforce Certified Technical Architect Mock Review Board Scenario: Flowers Racing Contents HYPOTHETICAL SCENARIO INSTRUCTIONS ...................................................................................................... 3 PROJECT OVERVIEW - FLOWERS RACING (FR) ................................................................................................. 4 CURRENT SYSTEMS ........................................................................................................................................ 4 BUSINESS PROCESS REQUIREMENTS .............................................................................................................. 5 RACE PLANNING AND RACER REGISTRATION ................................................................................................................ 5 RACER TRACKING AND CHARITY PLEDGES ................................................................................................................... 6 RACE LOGISTICS ..................................................................................................................................................... 7 CUSTOMER SUPPORT .............................................................................................................................................. 8 DATA MIGRATION REQUIREMENTS ............................................................................................................................ 8 ACCESSIBILITY REQUIREMENTS ................................................................................................................................. -

Motorsport News
Motorsport News International Edition – April 2019 Romania FUCHS sponsors Valentin Dobre in 2019 Under Managing Director Camelia Popa, FUCHS Romania joins Valentin Dobre in the Romania Hill Climb Championship. These very popular races attract numerous visitors and are broadcast by Romanian Television. // Page 3. Portugal FUCHS develops a new partnership with Teodósio Motorsport team Ricardo Teodósio and co-driver José Teixeira of the Teodósio Motorsport team represent FUCHS in the Portugal Rally Championship with a Škoda Fabia R5. The Teodósio team win their first race of the PRC, followed by three stage podiums in the FIA ERC, proving themselves worthy competitors and claiming the 2019 title. // Page 7. Spain FUCHS official partner of Yamaha R1 Cup Mario Castillejo, FUCHS Automotive Director, signs a sponsorship deal with Yamaha Motor Sport for the second edition of the Yamaha R1 Cup. In this series 23 drivers compete in six races on the most renowned tracks in Spain; a great business strategy for FUCHS. // Page 12. www.fuchs.com/group Motorsport News International Edition – April 2019 South Africa Scribante succeeds at Zwartkops Coming off a disappointing second round of the G&H Transport Series race in Cape Town, the Franco Scribante Racing team put in some hard work and made a few mechanical tweaks to their Porsche 997 Turbo in preparation for round 3 which took place at Zwartkops Raceway. A rain drenched track didn’t stop FUCHS sponsored Franco Scribante from asserting his dominance, winning round 3 of the Supercar Series. Scribante was quick to demonstrate his intentions in the qualifying race, claiming pole position. -

Physiological Determinants of Ultramarathon Trail-Running Performance
International Journal of Sports Physiology and Performance, (Ahead of Print) https://doi.org/10.1123/ijspp.2020-0766 © 2021 Human Kinetics, Inc. ORIGINAL INVESTIGATION Physiological Determinants of Ultramarathon Trail-Running Performance Alexandra M. Coates, Jordan A. Berard, Trevor J. King, and Jamie F. Burr Context: The physiological determinants of ultramarathon success have rarely been assessed and likely differ in their contributions to performance as race distance increases. Purpose: To examine predictors of performance in athletes who completed either a 50-, 80-, or 160-km trail race over a 20-km loop course on the same day. Methods: Measures of running history, aerobic fitness, running economy, body mass loss, hematocrit alterations, age, and cardiovascular health were examined in relation to race-day performance. Performance was defined as the percentage difference from the winning time at a given race distance, with 0% representing the fastest possible time. Results: In the 50-km race, training volumes, cardiovascular health, aerobic fitness, and a greater loss of body mass during the race were all related to better performance (all P < .05). Using multiple linear regression, peak velocity achieved in the maximal oxygen uptake test (β = −11.7, P = .002) and baseline blood pressure (β =3.1,P = .007) were the best performance predictors for the men’s 50-km race (r =.98,r2 = .96, P < .001), while peak velocity achieved in the maximal oxygen uptake test (β = −13.6, P = .001) and loss of body mass (β =12.8,P = .03) were the best predictors for women (r = .94, r2 = .87, P =.001).Inthe 80-km race, only peak velocity achieved in the maximal oxygen uptake test predicted performance (β = −20.3, r = .88, r2 = .78, P < .001). -

March 5-10 • 2018 • USA Welcome from the Craftsbury Outdoor Center
Ski Orienteering World Cup Round 3 World Masters Ski Orienteering Championships Bulletin 1 March 5-10 • 2018 • USA www.craftsbury.com/skio18 Welcome from the Craftsbury Outdoor Center The Town of Craftsbury and the Craftsbury Outdoor Center invite you to attend the March 2018 week of ski-orienteering races. We are excited to host this event in our special part of Vermont and the United States of America. We believe you will find a more friendly, welcoming, and beautiful part of America than you typically see in the media. Over the past 9 years, Craftsbury athletes have enjoyed competing around the world in ski-orienteering competitions. This week of competitions is one way to say thank you to all the people, organizations, and countries that have hosted ski-orienteering in the past. Contents Welcome from the Craftsbury Outdoor Center 2 Organizing Committee 4 Competition Schedule 4 Classes and Participation Restrictions 5 Housing 5 Location, Terrain, and Pre-Training Opportunities 5 Transportation 6 Embargoed Area 6 Embargoed Area Map 6 Doping control 7 Previous orienteering map 8 Organizing Committee Event Director: Adrian Owens Technical Director: Ed Despard Course Setters: Alex Jospe and Andy Hall Contact Website: craftsbury.com/skio18 E-mail: [email protected] Phone: +1 802.289.2890 Paper Mail: Adrian Owens 400 Post Rd Craftsbury Common, VT 05827 Controllers National Event Controller: Ken Walker, Sr (USA) IOF Event Advisor: Staffan Tunis (FIN) IOF Senior Event Advisor: Antti Myllärinen (FIN) Competition Schedule Date World Cup World -

Mongolian Derby
Adventure World magazine WINTER 2016 Mongolian Derby {Adventure World Magazine - Winter 2016} 1 presented by: USARA National Rankings Control Freaks 30.00 Checkpoint Zero 30.00 Topo Adventure Sports 29.00 Layer 3 29.00 Will Race For Food 28.00 No Sleep 28.00 Adventure Capitalists/BDAR 26.00 Team Lupine Racing USA 23.00 Hefner Bunny Pie 6.00 2 {Adventure World Magazine - Winter 2016} Contents Winter 2016 11 02 2016 USARA National Rankings 05 The Soul Man 08 USARA News 51 11 Pats Mongolian Derby 23 Product Reviews Editor: 28 The Sacred Door Trail Troy Farrar 37 Digiscoping Assistant Editor: Debbie Farrar 41 Exploring Orlando Graphic Designer: articles: 47 Gun Reviews Rae Zurcher 51 2015 USARA Adventure Race National Championship {Adventure World Magazine - Winter 2016} 3 4 {Adventure World Magazine - Winter 2016} The Soul Man by Melanie Ho When Charlie Engle reached the point where he wanted to quit RacingThePlanet: Ecuador 2015, he knew a goal to hit his own peak effort had been reached. Even for this seasoned veteran of long-distance multi-stage events, this year’s edition of the Roving Race with its Route of the Volcanoes was challenging. But the lure to take part could not be resisted. The inaugural Gobi March champion from the first 4 Deserts Series race in 2003 returned for the eighth edition of the Roving Race series, from July 26 to August 1. The American writer, film and television producer has run dozens of marathons and multi-stage events since taking up running in 1989. He placed third in the team category in the Gobi March 2006, has claimed podium finishes in other 4 Deserts Series races, and famously took his passion for running across the entire width of the Sahara Desert, which became the Running the Sahara documentary.