Zimbabwe – Cholera Outbreak
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Integrated Testing for TB and HIV Zimbabwe
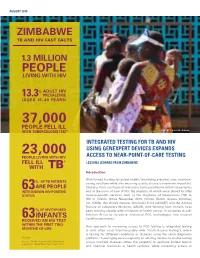
AUGUST 2019 ZIMBABWE TB AND HIV FAST FACTS 1.3 MILLION PEOPLE LIVING WITH HIV % ADULT HIV 13.3 PREVALENCE (AGES 15–49 YEARS) 37,000 PEOPLE FELL ILL WITH TUBERCULOSIS (TB)* © UNICEF/Costa/Zimbabwe INTEGRATED TESTING FOR TB AND HIV 23,000 USING GENEXPERT DEVICES EXPANDS PEOPLE LIVING WITH HIV ACCESS TO NEAR-POINT-OF-CARE TESTING FELL ILL * LESSONS LEARNED FROM ZIMBABWE WITH TB Introduction With limited funding for global health, identifying practical, cost- and time- OF TB PATIENTS % saving solutions while also ensuring quality of care is evermore important. 63ARE PEOPLE Globally, there are fleets of molecular testing platforms within laboratories WITH KNOWN HIV-POSITIVE and at the point of care (POC), the majority of which were placed to offer STATUS disease-specific services such as the diagnosis of tuberculosis (TB) or HIV in infants. Since November 2015, Clinton Health Access Initiative, Inc. (CHAI), the United Nations Children’s Fund (UNICEF) and the African Society of Laboratory Medicine (ASLM), with funding from Unitaid, have % OF HIV-EXPOSED been working closely with ministries of health across 10 countries in sub- Saharan Africa to introduce innovative POC technologies into national INFANTS 1 63 health programmes. RECEIVED AN HIV TEST WITHIN THE FIRST TWO One approach to increasing access to POC testing is integrated testing MONTHS OF LIFE (a term often used interchangeably with “multi-disease testing”), which is testing for different conditions or diseases using the same diagnostic *Annually platform.2 Leveraging excess capacity on existing devices to enable testing Sources: UNAIDS estimates 2019; World Health across multiple diseases offers the potential to optimize limited human Organization, ‘Global Tuberculosis Report 2018’ and financial resources at health facilities, while increasing access to rapid testing services. -

Zimbabwe Rapid Response Drought 2015
Resident / Humanitarian Coordinator Report on the use of CERF funds RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS ZIMBABWE RAPID RESPONSE DROUGHT 2015 RESIDENT/HUMANITARIAN COORDINATOR Bishow Parajuli REPORTING PROCESS AND CONSULTATION SUMMARY a. Please indicate when the After Action Review (AAR) was conducted and who participated. The CERF After Action Review took place on 25 May 2016. The review brought together focal points from the following key sectors and agencies: Health and Nutrition: UNICEF and WHO, Agriculture: FAO, Food Security: WFP and WASH: UNICEF. Considering the importance of the lessons learnt element, some sectors which did not benefit from the funding did nevertheless participate in order to gain a better understanding of CERF priorities, requirements and implementation strategies. b. Please confirm that the Resident Coordinator and/or Humanitarian Coordinator (RC/HC) Report was discussed in the Humanitarian and/or UN Country Team and by cluster/sector coordinators as outlined in the guidelines. YES X NO Sector focal points were part of the CERF consultation from inception through to final reporting. In addition, a CERF update was a standing agenda item discussed during the monthly Humanitarian Country Team meetings. c. Was the final version of the RC/HC Report shared for review with in-country stakeholders as recommended in the guidelines (i.e. the CERF recipient agencies and their implementing partners, cluster/sector coordinators and members and relevant government counterparts)? YES X NO All -

GOVERNMENT GAZETTE, 31ST Ocromer, 1986
_ ZIMBABWEAN GOVERNMENT GAZETTE Po a a Published by Authority ra Vol. LXIV, No. 56 31st OCTOBER, 1986 . Price 40c ’ General Notice 740 of 1986. The service to operate as follows— - . ; (a) depart Bulawayo Wednesday and Saturday 9 a.m., arrive i Se at ROAD MOTOR TRANSPORTATION ACT [CHAPTER262] Shashi 2.15 p.m.; i eae (b) depart, Bulawayo ¢ Friday and Sunday..5 p.m., arrive ‘ Applications in Connexion with Road Service Permits . Shashi 10.15 p.m.; , , (c) depart Shashi Monday and Thursday ~ 6 am., arrive Bula- ‘IN terms of subsection (4) of section 7 of the Road Motor wayo 11.15 a.m.; Transportation Act [Chapter 262], notice is hereby given that. (d) depart Shashi Saturday 3.am., arrive Bulawayo the applications detailed in the Schedule, for the issue or . 7.15 a.m.; amendment of road service permits, have been received for the (e). depart Shashi Sunday 7 a.m., arrive Bulawayo 12.15 p.m. consideration of the Controller of Road Motor Transportation. - Any person wishing to object to any such applicationmust lodge with the Controller of Road Motor Transportation, Kukura Kurerwa Bus Co. ' P.O. Box 8332, Causeway— a LOVNAIROBL go186. Permit: 14411. Motor-omnibus. Passenger-capacity: (a) a notice, in writing, of-his intention to ‘object, so asto ~ each the Controller’s office not later than the 21st Route: Nyamasoto Airfield - Masosowa Kraal - Charuwa November; 1986; / Kraal - Fosiyasi Store - Jairosi Kraal - Chironga Mission - (b) his objection and the grounds therefore, on form R.M-T. Chawanda ~ Mt, Darwin - Argyle Park - Bindura - Wayerera "24, together with twocopies thereof, so as to reach the School - Muchapondwa School - Shangwa Kraal - Chabwino Controller’s office not later than the 12th December, Farm - Shamva Road Junction - Harare. -
Making Sense of TB Data Guide for Collection, Analysis and Use of TB Data for Health Workers in Zimbabwe
Ministry of Health and Child Care Zimbabwe National Tuberculosis Control Programme Making Sense of TB data Guide for collection, analysis and use of TB data for health workers in Zimbabwe 1 ACKNOWLEDGEMENTS The Government of Zimbabwe is grateful to the US Agency for International Development (USAID) and the International Union Against Tuberculosis and Lung Disease (The Union), through the TB CARE I/Challenge TB funding mechanisms, for the technical and financial support in developing this guide. The Ministry of Health and Child Care extends its profound gratitude to Dr Einar Heldal (Senior Consultant, The Union), Dr Riitta Dlodlo (Director - TB-HIV, The Union) and Dr. C Zishiri, (Country Director –Challenge TB and The Union), Dr. R. Ncube (Deputy Country Director Challenge TB and The Union), Dr Barnet Nyathi (former Country Director, TB CARE I and The Union) who provided technical support. A special recognition goes to Mr Nicholas Siziba, NTP Monitoring and Evaluation Officer and Mr Nqobile Mlilo, TB CARE I Monitoring and Evaluation Coordinator who worked tirelessly from the first to the final version of the guide. Remarkable acknowledgements go the Matabeleland South Provincial Health Executive and Umzingwane District Health Executive for providing their data. The following have made substantial contributions to the document. Name Designation P T Shiri National Programme Assistant, NTP M Mukorera Training Coordinator, TB CARE I, The Union E Basvi Data Manager, NTP S Khumalo Provincial TB and Leprosy Coordinator, Matabeleland North S -
Approval Form
APPROVAL FORM Midlands State University The undersigned certify that they have read and made recommendations to the Midlands State University for acceptance of a research project entitled: Rural Local Authorities and investment attraction. The case of UMzingwane Rural District Council. The project was submitted in partial fulfilment of the requirements of the Bachelor of Science Honours Degree in Local Governance Studies. Supervisor Signature ………………………………………Date ………/………/………… Chairperson Signature ………………………………………Date ………/………/………… i RELEASEFORM Name of Student: Khulani Dube Registration Number: R101338f Dissertation Title: Rural Local Authorities and investment attraction. The case of UMzingwane Rural District Council. Degree Title: Bachelor of Science Honours Degree inLocal Governance Studies. Year of Completion: 2013 Permission is hereby being granted to Midlands State University Library to produce copies of this dissertation to lendcopies for private, scholarly or scientific research only. The author reserves the publication rights. Neither the dissertation nor extensive extracts from it may be printed or reproduced without the author’s written permission. Signed……………………………………………………………………………………… Date……………………………………………………………………………………….. Contact Details:15255Pumula South Bulawayo Telephone Number: 0772 528 806 Email address : [email protected] ii DECLARATION I KhulaniDubedeclare that this research is my original work that has not been submitted to any other University. The sources I used have been acknowledged. Date : October 2013 Student’s name : KhulaniDube Signature : ………………… iii DEDICATIONS I dedicate this research to my aunt Mrs P Bhebhe and my mother Mrs P Dube. iv ACKNOWLEDGEMENTS I would like to extend my gratitudeto my learning institution Midlands State University for the consistent support in all my academic endeavours. Special mention is due to the Local Governance Studies Department and its dedicated staff for providing me with the necessary and requisite skills and knowledge that have proved to be useful during the compilation of this project. -

Agnes Asekenye-Oonyu/OCHA/Zimbabwe/2006
Agnes Asekenye-Oonyu/OCHA/Zimbabwe/2006 SAMPLE OF ORGANISATIONS PARTICIPATING IN CONSOLIDATED APPEALS AARREC CRS HT MDM TEARFUND ACF CWS Humedica MEDAIR TGH ACTED Danchurchaid IA MENTOR UMCOR ADRA DDG ILO MERLIN UNAIDS Africare Diakonie Emergency Aid IMC NCA UNDP AMI-France DRC INTERMON NPA UNDSS ARC EM-DH Internews NRC UNEP ASB FAO INTERSOS OCHA UNESCO ASI FAR IOM OHCHR UNFPA AVSI FHI IPHD OXFAM UN-HABITAT CARE Finnchurchaid IR OXFAM UK UNHCR CARITAS French RC IRC PA (formerly ITDG) UNICEF CEMIR INTERNATIONAL FSD IRD PACT UNIFEM CESVI GAA IRIN PAI UNJLC CFA GOAL IRW Plan UNMAS CHF GTZ Islamic RW PMU-I UNOPS CHFI GVC JOIN PU UNRWA CISV Handicap International JRS RC/Germany VIS CMA HealthNet TPO LWF RCO WFP CONCERN HELP Malaria Consortium Samaritan's Purse WHO Concern Universal HelpAge International Malteser SECADEV World Concern COOPI HKI Mercy Corps Solidarités World Relief CORDAID Horn Relief MDA SUDO WV COSV TABLE OF CONTENTS 1. EXECUTIVE SUMMARY ............................................................................................................................. 1 Table I: Requirements, Commitments/Contributions and Pledges per Sector ............................................. 3 Table II. Requirements, Commitments/Contributions and Pledges by Priority............................................. 3 Table III. Requirements, Commitments/Contributions and Pledges per Appealing Organisation................. 4 2. CHANGES IN THE CONTEXT, HUMANITARIAN NEEDS, AND RESPONSE........................................... 6 3. RESPONSE PLANS................................................................................................................................... -

Grant Assistance for Grassroots Human Projects in Zimbabwe
Grant Assistance for Grassroots Human Projects in Zimbabwe Amount Amount No Year Project Title Implementing Organisation District (US) (yen) 1 1989 Mbungu Primary School Development Project Mbungu Primary School Gokwe 16,807 2,067,261 2 1989 Sewing and Knitting Project Rutowa Young Women's Club Gutu 5,434 668,382 3 1990 Children's Agricultural Project Save the Children USA Nyangombe 8,659 1,177,624 Mbungo Uniform Clothing Tailoring Workshop 4 1990 Mbungo Women's Club Masvingo 14,767 2,008,312 Project Construction of Gardening Facilities in 5 1991 Cold Comfort Farm Trust Harare 42,103 5,431,287 Support of Small-Scale Farmers 6 1991 Pre-School Project Kwayedza Cooperative Gweru 33,226 4,286,154 Committee for the Rural Technical 7 1992 Rural Technical Training Project Murehwa 38,266 4,936,314 Training Project 8 1992 Mukotosi Schools Project Mukotosi Project Committee Chivi 20,912 2,697,648 9 1992 Bvute Dam Project Bvute Dam Project Committee Chivi 3,558 458,982 10 1992 Uranda Clinic Project Uranda Clinic Project Committee Chivi 1,309 168,861 11 1992 Utete Dam Project Utete Dam Project Committee Chivi 8,051 1,038,579 Drilling of Ten Boreholes for Water and 12 1993 Irrigation in the Inyathi and Tsholotsho Help Age Zimbabwe Tsholotsho 41,574 5,072,028 PromotionDistricts of ofSocialForestry Matabeleland andManagement Zimbabwe National Conservation 13 1993 Buhera 46,682 5,695,204 ofWoodlands inCommunalAreas ofZimbabwe Trust Expansion of St. Mary's Gavhunga Primary St. Mary's Gavhunga Primary 14 1994 Kadoma 29,916 3,171,096 School School Tsitshatshawa -
ANALYSIS of SPATIAL PATTERNS of SETTLEMENT, INTERNAL MIGRATION, and WELFARE INEQUALITY in ZIMBABWE 1 Analysis of Spatial
ANALYSIS OF SPATIAL PATTERNS OF SETTLEMENT, INTERNAL MIGRATION, AND WELFARE INEQUALITY IN ZIMBABWE 1 Analysis of Spatial Public Disclosure Authorized Patterns of Settlement, Internal Migration, and Welfare Inequality in Zimbabwe Public Disclosure Authorized Public Disclosure Authorized Rob Swinkels Therese Norman Brian Blankespoor WITH Nyasha Munditi Public Disclosure Authorized Herbert Zvirereh World Bank Group April 18, 2019 Based on ZIMSTAT data Zimbabwe District Map, 2012 Zimbabwe Altitude Map ii ANALYSIS OF SPATIAL PATTERNS OF SETTLEMENT, INTERNAL MIGRATION, AND WELFARE INEQUALITY IN ZIMBABWE TABLE OF CONTENTS ACKNOWLEDGMENTS iii ABSTRACT v EXECUTIVE SUMMARY ix ABBREVIATIONS xv 1. INTRODUCTION AND OBJECTIVES 1 2. SPATIAL ELEMENTS OF SETTLEMENT: WHERE DID PEOPLE LIVE IN 2012? 9 3. RECENT POPULATION MOVEMENTS 27 4. REASONS BEHIND THE SPATIAL SETTLEMENT PATTERN AND POPULATION MOVEMENTS 39 5. CONSEQUENCES OF THE POPULATION’S SPATIAL DISTRIBUTION 53 6. POLICY DISCUSSION 71 AREAS FOR FURTHER RESEARCH 81 REFERENCES 83 APPENDIX A. SUPPLEMENTAL MAPS AND CHARTS 87 APPENDIX B. RESULTS OF REGRESSION ANALYSIS 99 APPENDIX C. EXAMPLE OF LOCAL DEVELOPMENT INDEX 111 ACKNOWLEDGMENTS This report was prepared by a team led by Rob Swinkels, comprising Therese Norman and Brian Blankespoor. Important background work was conducted by Nyasha Munditi and Herbert Zvirereh. Wishy Chipiro provided valuable technical support. Overall guidance was provided by Andrew Dabalen, Ruth Hill, and Mukami Kariuki. Peer reviewers were Luc Christiaensen, Nagaraja Rao Harshadeep, Hans Hoogeveen, Kirsten Hommann, and Marko Kwaramba. Tawanda Chingozha commented on an earlier draft and shared the shapefiles of the Zimbabwe farmland use types. Yondela Silimela, Carli Bunding-Venter, Leslie Nii Odartey Mills, and Aiga Stokenberga provided inputs to the policy section. -

Original Research Article the Spatial Dimension of Health Service
Scholars Journal of Applied Medical Sciences (SJAMS) ISSN 2320-6691 (Online) Sch. J. App. Med. Sci., 2016; 4(1C):201-204 ISSN 2347-954X (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Original Research Article The Spatial Dimension of Health Service Provision in Mashonaland West Province, Zimbabwe Takudzwa Mhandu, Dr Evans Chazireni Great Zimbabwe University, P O Box 1235, Masvingo, Zimbabwe *Corresponding author Dr Evans Chazireni Email: Abstract: Zimbabwe like many other developing countries has serious problems in its healthcare system. The quality of health service provision in Zimbabwe is generally poor Chazireni. Different parts of the country have serious healthcare problems. Mashonaland West, like other provinces in Zimbabwe, experiences numerous healthcare challenges. The research examines health service provision in Mashonaland West province in Zimbabwe. Data for this study was collected from ZIMSTAT published census reports and Ministry of health and Child Welfare published national health profiles. The analysis of the data was done through the composite index method. The calculated composite indices were used to rank the districts according to the level of health service provision. The researcher found out that there overall, the conditions of health service provision in Mashonaland West province is poor and that there are health service disparities among administrative districts in Mashonaland West province of Zimbabwe. There are many reasons which contribute to disparities in health care services at different levels (global, continental, regional, national and district level). It emerged from the research that the disparities are due to social, economic, physical and political factors. -
A Golden Opportunity: Scoping Study of Artisanal and Small Scale Gold Mining in Zimbabwe
pactworld.orgpactworld.org July 2015July 2015 pactworld.orgpactworld.org JulyJuly 20152015 AA Golden Golden Opportunity:Opportunity: ScopingScoping Study Study of Artisanal of Artisanal and Small Scale Gold Mining and Small Scale Gold Mining inin Zimbabwe in Zimbabwe SUBMITTED TO Phil Johnston Economic Adviser UK Department for International Development Zimbabwe British Embassy 3 Norfolk Road, Mount Pleasant, Harare, Zimbabwe TEL: +263 (0)4 8585 5375 E-MAIL: [email protected] UPDATED DOCUMENT SUBMITTED ON 22 June2015 SUBMITTED BY Pact Institute, 1828 L Street, NW, Suite 300 Washington, DC 20036, USA TEL: +1-202-466-5666 FAX: +1-202-466-5665 [email protected] CONTACT Peter Mudzwiti, ASM Scoping Study Lead E-MAIL: [email protected] Trevor Maisiri Country Director, Pact Zimbabwe TEL: +263 (0)4 250 942, +263 (0)772 414 465 E-MAIL: [email protected] ii Foreword Dear reader, We all rely on stereotypes to make sense of the world around us. The problem, of course, is that stereotypes aren’t always accurate. Many people believe that the typical artisanal gold miner in Zimbabwe is a single, migratory man in his early 20s who has no education, gambles away his money, and is likely to contract HIV. But the picture of the miners who participated in this study is rather different. In fact, mining is carried out by men, women, youth and children. The average miner is older and married with more children than non-miners in their community. They have more formal education, and earn and save more money than non-miners. And despite assumptions about lifestyles, miners are no more likely to be HIV-positive than non-miners. -

Zimbabwe Livelihood Baseline Profile
Zimbabwe Livelihood Baseline Profile Kariba Valley Kariangwe Jambezi Communal August-September 20101 Main Conclusions and Implications Crop production is the main food source over the reference year contributing 38 percent of very poor household food access and 82 percent for the Better-off. The main constraints to improved land utilisation and crop production are lack of draught power and poor access to seeds and fertiliser. Extension services and monitoring of agriculture activities should be strengthened through support to the ministry of agriculture’s department of extension services (AGRITEX). The livelihood zone borders with Mutusadona and Chizarira national parks. Proximity to national parks increases human, livestock and wildlife interaction. Elephants, Baboons, Buffaloes and Quela birds often stray into fields and destroy crops. Livestock production, which has relatively increased in recent years, is also limited by concerns over tsetse fly outbreaks. Surrounding communities receive little benefit from resources in the national parks except for the occasional slaughter of wild animals. Strengthening the CAMPFIRE scheme provides a framework for legal and sustainable access to natural resources found in the national parks. Food aid distributed for six months enabled very poor and poor households to access their minimum food requirements. Limited livelihood options and adverse weather conditions combine to increase very poor and poor households’ vulnerability to food insecurity and poverty. Over the last ten years, the risk of food insecurity has been addressed primarily through food aid distributions. External assistance whose focus has been on addressing immediate consumption needs has created dependency and is undermining long term household coping capacity and development prospects. -

PARKS and WILD LIFE ACT Acts 14/1975, 42/1976 (S
TITLE 20 TITLE 20 Chapter 20:14 PREVIOUS CHAPTER PARKS AND WILD LIFE ACT Acts 14/1975, 42/1976 (s. 39), 48/1976 (s. 82), 4/1977, 22/1977, 19/1978, 5/1979, 4/1981 (s. 19), 46/1981, 20/1982 (s.19 and Part XXVI), 31/1983, 11/1984, 35/1985, 8/1988 (s. 164), 1/1990, 11/1991 (s. 24), 22/1992 (s. 14); 19/2001; 22/2001; 13/2002. R.G.Ns 1135/1975, 52/1977, 126/1979, 294/1979, 265/1979, 294/1979, 748/1979; S.Is 675/1979, 632/1980, 640/1980, 704/1980, 773/1980, 781/1980, 786/1980, 139/1981, 140/1981, 181/1981, 183/1981, 639/1981, 860/1981, 139/1982, 140/1982, 337/1983, 454/1983, 123/1991 ARRANGEMENT OF SECTIONS PART I PRELIMINARY Section 1. Short title. 2. Interpretation. PART II PARKS AND WILD LIFE MANAGEMENT AUTHORITY 3. Establishment of Parks and Wild Life Management Authority. 4. Functions of Parks and Wild Life Management Authority. 5. Establishment and composition of Parks and Wild Life Management Authority Board. 6. Minister may give Board policy directions. 7. Minister may direct Board to reverse, suspend or rescind its decisions or actions. 8. Execution of contracts and instruments by Authority. 9. Reports of Authority. 10. Appointment and functions of Director-General and Directors of Authority. 11. Appointment of other staff of Authority. PART IIA FINANCIAL PROVISIONS 12. Funds of Authority. 13. Financial year of Authority. 14. Annual programmes and budgets of Authority. 15. Investment of moneys not immediately required by Authority. 16. Accounts of Authority.