For Peer Review Only - Page 1 of 17 BMJ Open
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

China Russia
1 1 1 1 Acheng 3 Lesozavodsk 3 4 4 0 Didao Jixi 5 0 5 Shuangcheng Shangzhi Link? ou ? ? ? ? Hengshan ? 5 SEA OF 5 4 4 Yushu Wuchang OKHOTSK Dehui Mudanjiang Shulan Dalnegorsk Nongan Hailin Jiutai Jishu CHINA Kavalerovo Jilin Jiaohe Changchun RUSSIA Dunhua Uglekamensk HOKKAIDOO Panshi Huadian Tumen Partizansk Sapporo Hunchun Vladivostok Liaoyuan Chaoyang Longjing Yanji Nahodka Meihekou Helong Hunjiang Najin Badaojiang Tong Hua Hyesan Kanggye Aomori Kimchaek AOMORI ? ? 0 AKITA 0 4 DEMOCRATIC PEOPLE'S 4 REPUBLIC OF KOREA Akita Morioka IWATE SEA O F Pyongyang GULF OF KOREA JAPAN Nampo YAMAJGATAA PAN Yamagata MIYAGI Sendai Haeju Niigata Euijeongbu Chuncheon Bucheon Seoul NIIGATA Weonju Incheon Anyang ISIKAWA ChechonREPUBLIC OF HUKUSIMA Suweon KOREA TOTIGI Cheonan Chungju Toyama Cheongju Kanazawa GUNMA IBARAKI TOYAMA PACIFIC OCEAN Nagano Mito Andong Maebashi Daejeon Fukui NAGANO Kunsan Daegu Pohang HUKUI SAITAMA Taegu YAMANASI TOOKYOO YELLOW Ulsan Tottori GIFU Tokyo Matsue Gifu Kofu Chiba SEA TOTTORI Kawasaki KANAGAWA Kwangju Masan KYOOTO Yokohama Pusan SIMANE Nagoya KANAGAWA TIBA ? HYOOGO Kyoto SIGA SIZUOKA ? 5 Suncheon Chinhae 5 3 Otsu AITI 3 OKAYAMA Kobe Nara Shizuoka Yeosu HIROSIMA Okayama Tsu KAGAWA HYOOGO Hiroshima OOSAKA Osaka MIE YAMAGUTI OOSAKA Yamaguchi Takamatsu WAKAYAMA NARA JAPAN Tokushima Wakayama TOKUSIMA Matsuyama National Capital Fukuoka HUKUOKA WAKAYAMA Jeju EHIME Provincial Capital Cheju Oita Kochi SAGA KOOTI City, town EAST CHINA Saga OOITA Major Airport SEA NAGASAKI Kumamoto Roads Nagasaki KUMAMOTO Railroad Lake MIYAZAKI River, lake JAPAN KAGOSIMA Miyazaki International Boundary Provincial Boundary Kagoshima 0 12.5 25 50 75 100 Kilometers Miles 0 10 20 40 60 80 ? ? ? ? 0 5 0 5 3 3 4 4 1 1 1 1 The boundaries and names show n and t he designations us ed on this map do not imply of ficial endors ement or acceptance by the United N at ions. -

The Comparison of Different Calculation Methods of Pollution Receiving Capacity for Jilin Province Huifa River
Nature Environment and Pollution Technology ISSN: 0972-6268 Vol. 15 No. 4 pp. 1169-1176 2016 An International Quarterly Scientific Journal Original Research Paper The Comparison of Different Calculation Methods of Pollution Receiving Capacity for Jilin Province Huifa River Yao Liwei and Men Baohui† Renewable Energy Institute, North China Electric Power University, Beijing-102206, China †Corresponding author: Men Baohui ABSTRACT Nat. Env. & Poll. Tech. Website: www.neptjournal.com Huifa River is the largest tributary of the Second Songhua River. Songhua River Basin is the concentrated area of Northeast Old Industrial Base, and it is also the distribution area of major cities, bearing Received: 19-12-2015 production task of national commodity grain. In recent years, with the rapid development of economy, Accepted: 28-01-2016 the deterioration of water quality is serious and the water environment problem is becoming more and Key Words: more outstanding, which have affected the sustainable development of the economic and social of Pollution receiving capacity Jilin province, so it is necessary to analyse and study the pollution receiving capacity of the river and Water quality model control the water pollution source to protect the water environment and strengthen water resources Sewage outfall protection. Based on one-dimensional water quality model, this paper use three kinds of different Huifa river generalization methods, such as midpoint generalization, uniform generalization and sewage outfall barycenter generalization, to calculate -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Daily Life for the Common People of China, 1850 to 1950
Daily Life for the Common People of China, 1850 to 1950 Ronald Suleski - 978-90-04-36103-4 Downloaded from Brill.com04/05/2019 09:12:12AM via free access China Studies published for the institute for chinese studies, university of oxford Edited by Micah Muscolino (University of Oxford) volume 39 The titles published in this series are listed at brill.com/chs Ronald Suleski - 978-90-04-36103-4 Downloaded from Brill.com04/05/2019 09:12:12AM via free access Ronald Suleski - 978-90-04-36103-4 Downloaded from Brill.com04/05/2019 09:12:12AM via free access Ronald Suleski - 978-90-04-36103-4 Downloaded from Brill.com04/05/2019 09:12:12AM via free access Daily Life for the Common People of China, 1850 to 1950 Understanding Chaoben Culture By Ronald Suleski leiden | boston Ronald Suleski - 978-90-04-36103-4 Downloaded from Brill.com04/05/2019 09:12:12AM via free access This is an open access title distributed under the terms of the prevailing cc-by-nc License at the time of publication, which permits any non-commercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited. An electronic version of this book is freely available, thanks to the support of libraries working with Knowledge Unlatched. More information about the initiative can be found at www.knowledgeunlatched.org. Cover Image: Chaoben Covers. Photo by author. Library of Congress Cataloging-in-Publication Data Names: Suleski, Ronald Stanley, author. Title: Daily life for the common people of China, 1850 to 1950 : understanding Chaoben culture / By Ronald Suleski. -
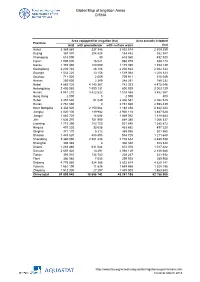
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52 -

Heilongjiang Road Development II Project (Yichun-Nenjiang)
Technical Assistance Consultant’s Report Project Number: TA 7117 – PRC October 2009 People’s Republic of China: Heilongjiang Road Development II Project (Yichun-Nenjiang) FINAL REPORT (Volume II of IV) Submitted by: H & J, INC. Beijing International Center, Tower 3, Suite 1707, Beijing 100026 US Headquarters: 6265 Sheridan Drive, Suite 212, Buffalo, NY 14221 In association with WINLOT No 11 An Wai Avenue, Huafu Garden B-503, Beijing 100011 This consultant’s report does not necessarily reflect the views of ADB or the Government concerned, ADB and the Government cannot be held liable for its contents. All views expressed herein may not be incorporated into the proposed project’s design. Asian Development Bank Heilongjiang Road Development II (TA 7117 – PRC) Final Report Supplementary Appendix A Financial Analysis and Projections_SF1 S App A - 1 Heilongjiang Road Development II (TA 7117 – PRC) Final Report SUPPLEMENTARY APPENDIX SF1 FINANCIAL ANALYSIS AND PROJECTIONS A. Introduction 1. Financial projections and analysis have been prepared in accordance with the 2005 edition of the Guidelines for the Financial Governance and Management of Investment Projects Financed by the Asian Development Bank. The Guidelines cover both revenue earning and non revenue earning projects. Project roads include expressways, Class I and Class II roads. All will be built by the Heilongjiang Provincial Communications Department (HPCD). When the project started it was assumed that all project roads would be revenue earning. It was then discovered that national guidance was that Class 2 roads should be toll free. The ADB agreed that the DFR should concentrate on the revenue earning Expressway and Class I roads, 2. -
INTERIM REPORT 2020 Contents
INTERIM REPORT 2020 Contents 2 Corporate Profile 29 Interim Condensed Consolidated Statement of 3 Interim Results Changes in Equity 4 Management Discussion and Analysis 30 Interim Condensed Consolidated Statement of 18 Corporate Governance Cash Flows 21 Other Information 31 Notes to Interim Condensed Consolidated 25 Independent Review Report Financial Information 26 Interim Condensed Consolidated Statement of 65 Glossary Profit or Loss and Other Comprehensive Income 67 Corporate Information 27 Interim Condensed Consolidated Statement of Financial Position 2 CORPORATE PROFILE JILIN PROVINCE CHUNCHENG HEATING COMPANY LIMITED I INTERIM REPORT 2020 Jilin Province Chuncheng Heating Company Limited* (吉林省春城熱力股份有限公司) (the “Company”, together with its subsidiaries, the “Group”) was established in Changchun City, Jilin Province, the People’s Republic of China (the “PRC”) on 23 October 2017. Heat supply is the Group’s core business. Over two decades’ operating history of heat supply enabled the Group to accumulate extensive experience and gradually consolidate its leading position in the industry. The Company transmits heat to the main municipal areas in Changchun using the cogeneration technology, the best heat supply mode in the industry which is energy-saving, efficient and environmentally-friendly. During the Reporting Period, the on-grid heat service area of the Group in Changchun amounted to approximately 42.73 million sq.m. and the Group is responsible for the provision of heat supply services for approximately 350,000 residential and non-residential -

Typhoon Annual Report of China
Member Report China April 9, 2021 CONTENTS I. Review of Tropical Cyclones Affecting China since Last Session of ESCAP/WMO Typhoon Committee ........................................................ 1 1.1 Meteorological and Hydrological Assessment .............................. 1 1.2 Socio-Economic Assessment ...................................................... 17 1.3 Regional Cooperation Assessment .............................................. 20 II. Progress in Key Research Areas ........................................................ 22 2.1 Application of Machine Learning (ML) in TC Intensity Estimation ......................................................................................................... 22 2.2 Advances in Typhoon Numerical Modeling ............................... 24 2.3 FY Satellite-Based Typhoon Monitoring and Disaster Pre-Evaluation .................................................................................. 28 2.4 Typhoon Field Observation Experiments.................................... 30 2.5 Advances in TC Scientific Research ........................................... 34 2.6 Enhancement of Typhoon Disaster Emergency Rescue .............. 38 2.7 Renaming Yutu - a Public Science Awareness Promotion Event 40 2.8 CMA-sponsored Training on Skills in TC .................................. 41 I. Review of Tropical Cyclones Affecting China since Last Session of ESCAP/WMO Typhoon Committee 1.1 Meteorological and Hydrological Assessment A weak El Niño event lingered from November 2019 to April 2020 over the -

Soil Ph Is the Primary Factor Driving the Distribution and Function of Microorganisms in Farmland Soils in Northeastern China
Annals of Microbiology (2019) 69:1461–1473 https://doi.org/10.1007/s13213-019-01529-9 ORIGINAL ARTICLE Soil pH is the primary factor driving the distribution and function of microorganisms in farmland soils in northeastern China Cheng-yu Wang1 & Xue Zhou1 & Dan Guo1 & Jiang-hua Zhao1 & Li Yan1 & Guo-zhong Feng1 & Qiang Gao1 & Han Yu2 & Lan-po Zhao1 Received: 26 May 2019 /Accepted: 3 November 2019 /Published online: 19 December 2019 # The Author(s) 2019 Abstract Purpose To understand which environmental factors influence the distribution and ecological functions of bacteria in agricultural soil. Method A broad range of farmland soils was sampled from 206 locations in Jilin province, China. We used 16S rRNA gene- based Illumina HiSeq sequencing to estimated soil bacterial community structure and functions. Result The dominant taxa in terms of abundance were found to be, Actinobacteria, Acidobacteria, Gemmatimonadetes, Chloroflexi, and Proteobacteria. Bacterial communities were dominantly affected by soil pH, whereas soil organic carbon did not have a significant influence on bacterial communities. Soil pH was significantly positively correlated with bacterial opera- tional taxonomic unit abundance and soil bacterial α-diversity (P<0.05) spatially rather than with soil nutrients. Bacterial functions were estimated using FAPROTAX, and the relative abundance of anaerobic and aerobic chemoheterotrophs, and nitrifying bacteria was 27.66%, 26.14%, and 6.87%, respectively, of the total bacterial community. Generally, the results indicate that soil pH is more important than nutrients in shaping bacterial communities in agricultural soils, including their ecological functions and biogeographic distribution. Keywords Agricultural soil . Soil bacterial community . Bacterial diversity . Bacterial biogeographic distribution . -
05 Ctt0401c Ni
CHINESE RAILWAY TIMETABLE APRIL 2001 EDITION Compiled By Duncan Peattie © Duncan Peattie, July 2001 Please read the Copyright Notice on page 15 Page 1 CTT0401C.xls Version date: 19-07-01 Page 1 Chinese Railway Timetable - April 2001 Edition CONTENTS SECTION/ CONTENTS / LINES COVERED VERSION FIRST No. OF TABLE DATE PAGE PAGES Title Title 19-07-01 1 1 Contents Contents (this page) 19-07-01 2 3 Intro Introduction and Acknowledgments 19-07-01 5 2 User Guide Explanation of how to use the timetable 10-07-01 7 1 Example Example table and notes 12-07-01 8 1 Index Station index showing table numbers 19-07-01 9 6 Overlapping Details of cases where more than one table covers one section of line. 19-07-01 15 1 Tables/ Also COPYRIGHT NOTICE - please read this. Copyright Non-Daily Details of trains which do not operate every day 19-07-01 16 2 Trains Key Table showing the relationship between tables of this timetable and pages of the CRPH timetable 12-07-01 18 4 1 Jing-Shan (1), Jing-Qin (3), Tie-Fa (1F) and Tao-Yu (1G) lines 12-07-01 22 6 BEIJING - TIANJIN / FENGRUN - QINGHUANGDAO - JINZHOU - SHENYANG - SIPING - CHANGCHUN - HAERBIN 1# Jing-Shan (1) [part] and Tanggu (1B) lines 12-07-01 28 2 BEIJING - TIANJIN - TAIDA (Complete Service) 4 Shen-Dan (4) and Liao-Xi (4A) lines and branches (4D/E) 12-07-01 30 1 SHENYANG / LIAOYANG - BENXI - TONGYUANPU - DANDONG 5 Chang-Da (5), Gou-Hai (5A) and Yingkou (5B) lines 12-07-01 31 2 SHENYANG - ANSHAN - GOUBANGZI / DASHIQIAO - YINGKOU / WAFANGDIAN - DALIAN TABLES FOR LOCAL LINES L1-5 28-06-01+ 33 1 1A Jin-Ji line -

North Korean Migrants in China
NORTH KOREAN MIGRANTS IN CHINA: A CASE STUDY OF HUMAN SMUGGLING AND TRAFFICKING BY HYOUNGAH PARK A dissertation submitted to the Graduate School-Newark Rutgers, The State University of New Jersey In partial fulfillment of the requirements For the degree of Doctor of Philosophy Graduate Program in the School of Criminal Justice Written under the direction of Ko-Lin Chin And approved by ____________________________________________ ____________________________________________ ____________________________________________ ____________________________________________ Newark, New Jersey October 2018 Copyright page: 2018 Hyoungah Park ALL RIGHTS RESERVED ABSTRACT OF THE DISSERTATION North Korean Migrants in China: A Case Study of Human Smuggling and Trafficking By Hyoungah Park Dissertation Director: Ko-lin Chin This study investigates the smuggling and trafficking (e.g. forced marriage, sex trafficking, and labor exploitation) of North Korean Migrants in China (NKMCs). It seeks to answer the following questions: First, how should we define the status of NKMCs (e.g. illegal economic migrant, refugee, or trafficking victim)? Second, are the NKMCs victimized? If any, what are the contexts and factors that contribute to such victimization, and how? Further, what are the characteristics of the victims, smugglers, and traffickers? Finally, what are the contributing factors and possible policy implications to prevent the victimization of NKMCs? For this, one-on-one, face-to-face in-depth interviews with 58 NKMCs (47 women and 11 men) currently living in South Korea were conducted. Study participants were recruited through the purposive snowball sampling method. Interviews were conducted using a standardized questionnaire. This study suggests that 37 NKMCs (64%) should be classified as trafficking victims of forced marriage, commercial sex, or labor exploitation. -

Democartic People's Republic of Korea Atlas
PGDS in DOS Democratic People's Rep. of Korea Atlas Map Population and Geographic Data Section As of July 2005 Division of Operational Support Email : [email protected] ! !!!!!!!! ) )))))))) )))))))) ! ! Nongan ! !!!!!!!! Shulan ))) Pogranichnyy ))))))))))))))))) ! !!!!!!!! Ningan r ! !!!!!!!! Jiutai o w ! !!!!!!!! . ! ! Dongjingcheng C P 3 A _ m e D _ p e ! !!!!!!!! R ! ! Changchung _ ! !!!!!!!! Jilin a ! ! e r ! !!!!!!!! o ! ! Jiaohe K ! !!!!!!!! Datun ! !!!!!!!! Xinan ! !!!!!!!! ! !!!!!!!! Gongzhuling ! !!!!!!!! Dunhua ! !!!!!!!! Yitong ! !!!!!!!! Yantongshan ! !!!!!!!! Bamiancheng ! !!!!!!!! ! !!!!!!!! ! ! Huadian ! !!!!!!!! Tumen) )))))))))))))))) ! !!!!!!!! Panshi ))) ! !!!!!!!! Liaoyuan ! !!!!!!!! Yanji ! !!!!!!!! Hunchun ! !!!!!!!! ! !!!!!!!! ! ! Chongsong ! ! Laochengzhen ! !!!!!!!! ))))))))))))))))) I Dong ) )))))))) )))))))) CHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINACHINA ! !!!!!!!! Kaishantun ))) Kraskino ! !!!!!!!! Dongfeng ! !!!!!!!! ))))))))))))))))) Hailong ! !!!!!!!! Laocheng ))))))))))))))))) Sechon-dong ! !!!!!!!! Helong ! !!!!!!!! Kaiyuan ! !!!!!!!! Meihekou ! !!!!!!!! Kyongchung ) )))))))) )))))))) ! !!!!!!!! ))) Yuson! ! ! !!!!!!!! Qingyu ! !!!!!!!! Shanchengzhen ! !!!!!!!! Unggi ! !!!!!!!! Lihue ))))))))))))))))) Najin ))))))))))))))))) Musan ))))))))))))))))) Komusan Dong ))))))))))))))))) ! !!!!!!!! Hunjiang !! Fushun ) )))))))) )))))))) Lingjiang ))) ! !!!!!!!! ! ! ) )))))))))))))))) ! !!!!!!!! Tong Hua ))) Nanam RUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIANRUSSIAN