Varicocele Is the Root Cause Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Normal 3T MR Anatomy of the Prostate Gland and Surrounding Structures
Hindawi Advances in Medicine Volume 2019, Article ID 3040859, 9 pages https://doi.org/10.1155/2019/3040859 Review Article Normal 3T MR Anatomy of the Prostate Gland and Surrounding Structures K. Sklinda ,1 M. Fra˛czek,2 B. Mruk,1 and J. Walecki1 1MD PhD, Dpt. of Radiology, Medical Center of Postgraduate Education, CSK MSWiA, Woloska 137, 02-507 Warsaw, Poland 2MD, Dpt. of Radiology, Medical Center of Postgraduate Education, CSK MSWiA, Woloska 137, 02-507 Warsaw, Poland Correspondence should be addressed to K. Sklinda; [email protected] Received 24 September 2018; Accepted 17 December 2018; Published 28 May 2019 Academic Editor: Fakhrul Islam Copyright © 2019 K. Sklinda et al. +is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Development on new fast MRI scanners resulted in rising number of prostate examinations. High-spatial resolution of MRI examinations performed on 3T scanners allows recognition of very fine anatomical structures previously not demarcated on performed scans. We present current status of MR imaging in the context of recognition of most important anatomical structures. 1. Introduction also briefly present benign prostate hypertrophy (BPH) which is the most common condition of the prostate, oc- Aging of the society together with growing consciousness of curring in most patients over 50 years of age. the role of early detection of oncologic diseases leads to globally occurring rise in number of detected cases of 2. Imaging Protocol prostate cancer. Widely used transrectal sonography of the prostate gland despite additional support of contrast media According to PI-RADS v2, T1W and T2W sequences should and elastography does not provide sufficient sensitivity or be obtained for all prostate mpMR exams [1]. -

Mvdr. Natália Hvizdošová, Phd. Mudr. Zuzana Kováčová
MVDr. Natália Hvizdošová, PhD. MUDr. Zuzana Kováčová ABDOMEN Borders outer: xiphoid process, costal arch, Th12 iliac crest, anterior superior iliac spine (ASIS), inguinal lig., mons pubis internal: diaphragm (on the right side extends to the 4th intercostal space, on the left side extends to the 5th intercostal space) plane through terminal line Abdominal regions superior - epigastrium (regions: epigastric, hypochondriac left and right) middle - mesogastrium (regions: umbilical, lateral left and right) inferior - hypogastrium (regions: pubic, inguinal left and right) ABDOMINAL WALL Orientation lines xiphisternal line – Th8 subcostal line – L3 bispinal line (transtubercular) – L5 Clinically important lines transpyloric line – L1 (pylorus, duodenal bulb, fundus of gallbladder, superior mesenteric a., cisterna chyli, hilum of kidney, lower border of spinal cord) transumbilical line – L4 Bones Lumbar vertebrae (5): body vertebral arch – lamina of arch, pedicle of arch, superior and inferior vertebral notch – intervertebral foramen vertebral foramen spinous process superior articular process – mammillary process inferior articular process costal process – accessory process Sacrum base of sacrum – promontory, superior articular process lateral part – wing, auricular surface, sacral tuberosity pelvic surface – transverse lines (ridges), anterior sacral foramina dorsal surface – median, intermediate, lateral sacral crest, posterior sacral foramina, sacral horn, sacral canal, sacral hiatus apex of the sacrum Coccyx coccygeal horn Layers of the abdominal wall 1. SKIN 2. SUBCUTANEOUS TISSUE + SUPERFICIAL FASCIAS + SUPRAFASCIAL STRUCTURES Superficial fascias: Camper´s fascia (fatty layer) – downward becomes dartos m. Scarpa´s fascia (membranous layer) – downward becomes superficial perineal fascia of Colles´) dartos m. + Colles´ fascia = tunica dartos Suprafascial structures: Arteries and veins: cutaneous brr. of posterior intercostal a. and v., and musculophrenic a. -

Genitalia Blood Supply to Internal Female Course
U4-Reproductive BS+NS DEC 2016 FNF, approved by: DR.manoj Blood supply to internal female genitalia: artery origin distribution Anastamoses? Course Sup. large branch: Medially in base of broad Yes, cranially with Internal iliac uterus, inf. Small ligament to junction between ovarian, caudally uterine artery branch: cervix+ sup. cervix and uterus, run above with vaginal Vagina ureter, ascend to anastamose Middle +inferior part Yes, ant+post azygos Descand to vagina after Uterine of vagina along with arteries of vagina branching at junction between Vaginal artery pudendal artery with uterine artery uterus + cervix Yes, with uterine Descend along post. abdominal artery (collateral Ovarian Abdominal wall, at pelvic prim cross Ovary+ uterine tube circulation between artery aorta external iliac> enter suspensory abdominal +pelvic ligament source) vein Drainage Anastamoses? Course Vaginal venous plexus>vaginal vein> anastamose with uterine venous plexus Yes, vaginal plexus with Sides of vagina Vaginal >uterovaginal venous plexus>uterine uterine plexus vein>internal iliac vein uterine venous plexus >uterovaginal Yes, vaginal plexus with Uterine venous plexus>uterine vein>internal iliac Pass in broad ligament uterine plexus vein Pampiniform plexus of veins>ovarian vein Plexus in broad ligament Ovarian Rt:IVC - , ovarian vein in suspensory ligament Lt:LRV Note: -tubal veins drain in ovarian veins+ uterovaginal venous plexus -uterine vessels pass in cardinal ligament 1 | P a g e U4-Reproductive BS+NS DEC 2016 FNF, approved by: DR.manoj Blood supply to external female genitalia: artery origin distribution Course Perineum Leave pelvis through greater sciatic foramen hook Internal Internal iliac artery +external around ischial spine then enter through lesser pudendal genitalia sciatic foramen. -

Prostate 1 Prostate
Prostate 1 Prostate Prostate Male Anatomy Prostate with seminal vesicles and seminal ducts, viewed from in front and above. Latin prostata [1] Gray's subject #263 1251 Artery internal pudendal artery, inferior vesical artery, and middle rectal artery Vein prostatic venous plexus, pudendal plexus, vesicle plexus, internal iliac vein Nerve inferior hypogastric plexus Lymph external iliac lymph nodes, internal iliac lymph nodes, sacral lymph nodes Precursor Endodermic evaginations of the urethra [2] MeSH Prostate [3] Dorlands/Elsevier Prostate The prostate (from Greek προστάτης - prostates, literally "one who stands before", "protector", "guardian"[4] ) is a compound tubuloalveolar exocrine gland of the male reproductive system in most mammals unless they have it removed at birth.[5] [6] In 2002, female paraurethral glands, or Skene's glands, were officially renamed the female prostate by the Federative International Committee on Anatomical Terminology.[7] The prostate differs considerably among species anatomically, chemically, and physiologically. Prostate 2 Function The function of the prostate is to store and secrete a slightly alkaline fluid, milky or white in appearance,[8] that usually constitutes 20-30% of the volume of the semen along with spermatozoa and seminal vesicle fluid. The alkalinity of semen helps neutralize the acidity of the vaginal tract, prolonging the lifespan of sperm. The alkalinization of semen is primarily accomplished through secretion from the seminal vesicles.[9] The prostatic fluid is expelled in the first ejaculate fractions, together with most of the spermatozoa. In comparison with the few spermatozoa expelled together with mainly seminal vesicular fluid, those expelled in prostatic fluid have better motility, longer survival and better protection of the genetic material (DNA). -

The Prostate
The Prostate It is an accessory gland of male reproductive system, which surrounds the prostatic urethra Site : it lies in the lower part of the lesser pelvis behind the inferior border of the pubic symphysis in front of the rectum, below neck of the bladder. The prostatic capsules: 1. Inner true capsule : it is fibromuscular in structure. 2. Outer false capsule (prostatic sheath): it is a condensed visceral pelvic fascia. Between the two capsules, lies the prostatic venous plexus. Shape and Description: It simulates an inverted cone which has a base (directed superiorly); an apex (directed inferiorly), four surfaces: anterior, posterior, and two inferolateral surfaces. 1- Base of the prostate : It is directed upwards, separated from the bladder by a groove contains part of the prostatic venous plexus. It is pierced by the urethra. 2- Apex of the prostate: Is directed downwards It rests on the perineal membrane (floor of the deep perineal pouch). The urethra emerges from the prostate anterosuperior to the apex. 3-Anterior surface: It is convex and lies behind the lower part of the symphysis pubis. Its upper part is connected to the pubic bodies by puboprostatic ligaments. The urethra emerges from this surface a little above and in front of the apex of the gland. 4- Posterior surface: It is nearly fiat and is related to ampulla of the rectum separated from it by rectovesical fascia (fascia of Denonvilliers) The prostate is easily palpated by a finger in the rectum Near its upper border, this surface is pierced by the two ejaculatory ducts. 5- Right and left inferolateral surfaces: Are convex and related to levator prostatae parts of levator ani muscle. -

Anatomy and Physiology Model Guide Book
Anatomy & Physiology Model Guide Book Last Updated: August 8, 2013 ii Table of Contents Tissues ........................................................................................................................................................... 7 The Bone (Somso QS 61) ........................................................................................................................... 7 Section of Skin (Somso KS 3 & KS4) .......................................................................................................... 8 Model of the Lymphatic System in the Human Body ............................................................................. 11 Bone Structure ........................................................................................................................................ 12 Skeletal System ........................................................................................................................................... 13 The Skull .................................................................................................................................................. 13 Artificial Exploded Human Skull (Somso QS 9)........................................................................................ 14 Skull ......................................................................................................................................................... 15 Auditory Ossicles .................................................................................................................................... -
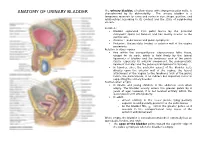
ANATOMY of URINARY BLADDER Characterized by Its Distensibility
The urinary bladder, a hollow viscus with strong muscular walls, is ANATOMY OF URINARY BLADDER characterized by its distensibility . The urinary bladder is a temporary reservoir for urine and varies in size, shape, position, and relationships according to its content and the state of neighboring viscera. Location : Bladder separated from pubic bones by the potential retropubic space (of Retzius) and lies mostly inferior to the peritoneum, Anterior : pubic bones and pubic symphysis Posterior : the prostate (males) or anterior wall of the vagina posteriorly Relation to other organs free within the extraperitoneal subcutaneous fatty tissue, except for its neck, which is held firmly by the lateral ligaments of bladder and the tendinous arch of the pelvic fascia—especially its anterior component, the puboprostatic ligament in males and the pubovesical ligament in females In females, since the posterior aspect of the bladder rests directly upon the anterior wall of the vagina, the lateral attachment of the vagina to the tendinous arch of the pelvic fascia, the paracolpium, is an indirect but important factor in supporting the urinary bladder Position when empty In infants and young children: in the abdomen even when empty. The bladder usually enters the greater pelvis by 6 years of age; however, it is not located entirely within the lesser pelvis until after puberty. In adult : o almost entirely in the lesser pelvis, lying partially superior to and partially posterior to the pubic bones o As the bladder fills, enters the greater pelvis as it ascends in the extraperitoneal fatty tissue of the anterior abdominal wall When empty, the bladder is somewhat tetrahedral externally has an apex,body, fundus, and neck. -

The Cerebrospinal Venous System: Anatomy, Physiology, and Clinical Implications Edward Tobinick, MD
5/8/2017 www.medscape.org/viewarticle/522597_print www.medscape.org The Cerebrospinal Venous System: Anatomy, Physiology, and Clinical Implications Edward Tobinick, MD Posted: 2/22/2006 Abstract and Introduction Abstract There is substantial anatomical and functional continuity between the veins, venous sinuses, and venous plexuses of the brain and the spine. The term "cerebrospinal venous system" (CSVS) is proposed to emphasize this continuity, which is further enhanced by the general lack of venous valves in this network. The first of the two main divisions of this system, the intracranial veins, includes the cortical veins, the dural sinuses, the cavernous sinuses, and the ophthalmic veins. The second main division, the vertebral venous system (VVS), includes the vertebral venous plexuses which course along the entire length of the spine. The intracranial veins richly anastomose with the VVS in the suboccipital region. Caudally, the CSVS freely communicates with the sacral and pelvic veins and the prostatic venous plexus. The CSVS constitutes a unique, largecapacity, valveless venous network in which flow is bidirectional. The CSVS plays important roles in the regulation of intracranial pressure with changes in posture, and in venous outflow from the brain. In addition, the CSVS provides a direct vascular route for the spread of tumor, infection, or emboli among its different components in either direction. Introduction "... we begin to wonder whether our conception of the circulation today is completely acceptable. As regards the venous part of the circulation, I believe our present conception is incorrect." Herlihy[1] "It seems incredible that a great functional complex of veins would escape recognition as a system until 1940.. -

Posterior Mediastinum: Mediastinal Organs 275
104750_S_265_290_Kap_4:_ 05.01.2010 10:43 Uhr Seite 275 Posterior Mediastinum: Mediastinal Organs 275 1 Internal jugular vein 2 Right vagus nerve 3 Thyroid gland 4 Right recurrent laryngeal nerve 5 Brachiocephalic trunk 6 Trachea 7 Bifurcation of trachea 8 Right phrenic nerve 9 Inferior vena cava 10 Diaphragm 11 Left subclavian artery 12 Left common carotid artery 13 Left vagus nerve 14 Aortic arch 15 Esophagus 16 Esophageal plexus 17 Thoracic aorta 18 Left phrenic nerve 19 Pericardium at the central tendon of diaphragm 20 Right pulmonary artery 21 Left pulmonary artery 22 Tracheal lymph nodes 23 Superior tracheobronchial lymph nodes 24 Bronchopulmonary lymph nodes Bronchial tree in situ (ventral aspect). Heart and pericardium have been removed; the bronchi of the bronchopulmonary segments are dissected. 1–10 = numbers of segments (cf. p. 246 and 251). 15 12 22 6 11 5 2 1 14 2 23 1 3 21 3 20 24 4 5 4 17 8 5 6 6 15 8 7 8 9 9 10 10 Relation of aorta, pulmonary trunk, and esophagus to trachea and bronchial tree (schematic drawing). 1–10 = numbers of segments (cf. p. 246 and 251). 104750_S_265_290_Kap_4:_ 05.01.2010 10:43 Uhr Seite 276 276 Posterior Mediastinum: Mediastinal Organs Mediastinal organs (ventral aspect). The heart with the pericardium has been removed, and the lungs and aortic arch have been slightly reflected to show the vagus nerves and their branches. 1 Supraclavicular nerves 12 Right pulmonary artery 24 Left vagus nerve 2 Right internal jugular vein with ansa cervicalis 13 Right pulmonary veins 25 Left common carotid artery -

Veins of the Systemic Circulation
O.L. ZHARIKOVA, L.D.CHAIKA VEINS OF THE SYSTEMIC CIRCULATION Minsk BSMU 2020 0 МИНИСТЕРСТВО ЗДРАВООХРАНЕНИЯ РЕСПУБЛИКИ БЕЛАРУСЬ БЕЛОРУССКИЙ ГОСУДАРСТВЕННЫЙ МЕДИЦИНСКИЙ УНИВЕРСИТЕТ КАФЕДРА НОРМАЛЬНОЙ АНАТОМИИ О. Л. ЖАРИКОВА, Л.Д.ЧАЙКА ВЕНЫ БОЛЬШОГО КРУГА КРОВООБРАЩЕНИЯ VEINS OF THE SYSTEMIC CIRCULATION Учебно-методическое пособие Минск БГМУ 2018 1 УДК 611.14 (075.8) — 054.6 ББК 28.706я73 Ж34 Рекомендовано Научно-методическим советом в качестве учебно-методического пособия 21.10.2020, протокол №12 Р е ц е н з е н т ы: каф. оперативной хирургии и топографической анатомии; кан- дидат медицинских наук, доцент В.А.Манулик; кандидат филологических наук, доцент М.Н. Петрова. Жарикова, О. Л. Ж34 Вены большого круга кровообращения = Veins of the systemic circulation : учебно-методическое пособие / О. Л. Жарикова, Л.Д.Чайка. — Минск : БГМУ, 2020. — 29 с. ISBN 978-985-21-0127-1. Содержит сведения о топографии и анастомозах венозных сосудов большого круга кровообраще- ния. Предназначено для студентов 1-го курса медицинского факультета иностранных учащихся, изучающих дисциплину «Анатомия человека» на английском языке. УДК 611.14 (075.8) — 054.6 ББК 28.706я73 ISBN 978-985-21-0127-1 © Жарикова О. Л., Чайка Л.Д., 2020 © УО «Белорусский государственный медицинский университет», 2020 2 INTRODUCTION The cardiovascular system consists of the heart and numerous blood and lymphatic vessels carrying blood and lymph. The major types of the blood ves- sels are arteries, veins, and capillaries. The arteries conduct blood away from the heart; they branch into smaller arteries and, finally, into their smallest branches — arterioles, which give rise to capillaries. The capillaries are the smallest vessels that serve for exchange of gases, nutrients and wastes between blood and tissues. -

Vas Deferens : Blood Supply : Artery of the Vas Is Derived from Inferior Vesical Artery
Vas deferens : Blood supply : Artery of the vas is derived from inferior vesical artery. It runs in the spermatic cord and anastomoses with the testicular artery. Veins : join the vesical venous plexus. Nerves : are derived from prostatic nerve plexus which comes from the inferior hypogastric plexus. Fibers are mainly sympathetic for the process of ejaculation. Seminal Vesicles Arterial supply : from inferior vesical and middle rectal arteries. Veins : to vesical venous plexus. Nerves: from prostatic nerve plexus (mainly sympathetic). Bulbourethral Glands : Blood supply: by artery of the bulb of the penis. It is innervated by prostatic nerve plexus Prostate gland: Arteries are derived from inferior vesical and middle rectal arteries. Venous drainage : the veins form the prostatic venous plexus which has the following features : It is embedded between the two capsules of the prostate. It is present only in front and sides of the gland Superiorly, it is continuous with the vesical venous plexus. Anteriorly : it receives the deep dorsal vein of penis. Posterolaterally : the plexus is drained to the internal iliac veins which in turn communicates with the internal vertebral venous plexuses by the Batson venous plexus. These veins are valveless and responsible for spread of cancer prostate to lumbar vertebrae Lymphatic Drainage: to internal, external iliac lymph nodes. Nerve Supply: by prostatic nerve plexus derived from the inferior hypogastric plexus. Penis Blood supply :All are branches of internal pudendal artery and all are paired (right and left). • Dorsal artery of the penis supplies the skin, fascia, and glans . • Deep artery of the penis supplies the corpus cavernous with convoluted helicine arteries • Artery of the bulb supplies the corpus spongiosum and glans penis Venous drainage of penis 1 . -

Ursa Education Institute for Manual Therapy 1221 S Street, Sacramento, CA 95811 Page 1
Analysis and Correction of Locomotor Dysfunction as It Applies to Autonomic Nervous System Dysregulation Lab Lino Cedros ATC, MT, CAMTC Neal O’Neal PT Test leg for loss of femur internal rotation – Mechanical or Chapman’s Obturator internus Piriformis Quadratus Laborum Illiopsoas Test groin glands for pelvic congestion GG-The lowest 2/5ths of the Sartorius muscle and its tendinous attachment on the tibia and just above the inner condyle of the femur. Chapmans drainage - Rectum and Hemorrhoids R-Lesser trochanter of the femur downward. H-Just medial and above the tuber ischii. Indicates congestion of the glands draining the rectal walls and tissues – in the rectum just below the sigmoid flexure Deep rotatory movement Reach from back for femoral points Drainage area-At angles of 7th and 8 rids on left side is a very sensitive reflex about 3 inches from the spine. Indicates a variant of rectum and colon close to the sigmoid flexure. Deep pressure between 5-6 sacral nerves for tight anal sphincter. Ursa Education Institute for Manual Therapy 1221 S Street, Sacramento, CA 95811 http://www.ursa.education/ Page 1 Test heel sign Test Hypogastic plexus Midline Sided Ursa Education Institute for Manual Therapy 1221 S Street, Sacramento, CA 95811 http://www.ursa.education/ Page 2 Test foot shake Test great toe movement on first cuneiform Ursa Education Institute for Manual Therapy 1221 S Street, Sacramento, CA 95811 http://www.ursa.education/ Page 3 Test muscles of the foot related to fluid drive Ursa Education Institute for Manual Therapy 1221 S Street, Sacramento, CA 95811 http://www.ursa.education/ Page 4 Test talus for glide- Fred Mitchell Jr test.