Anatomical Eponyms — Unloved Names in Medical Terminology F
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

The Anatomy of the Rectum and Anal Canal
BASIC SCIENCE identify the rectosigmoid junction with confidence at operation. The anatomy of the rectum The rectosigmoid junction usually lies approximately 6 cm below the level of the sacral promontory. Approached from the distal and anal canal end, however, as when performing a rigid or flexible sigmoid- oscopy, the rectosigmoid junction is seen to be 14e18 cm from Vishy Mahadevan the anal verge, and 18 cm is usually taken as the measurement for audit purposes. The rectum in the adult measures 10e14 cm in length. Abstract Diseases of the rectum and anal canal, both benign and malignant, Relationship of the peritoneum to the rectum account for a very large part of colorectal surgical practice in the UK. Unlike the transverse colon and sigmoid colon, the rectum lacks This article emphasizes the surgically-relevant aspects of the anatomy a mesentery (Figure 1). The posterior aspect of the rectum is thus of the rectum and anal canal. entirely free of a peritoneal covering. In this respect the rectum resembles the ascending and descending segments of the colon, Keywords Anal cushions; inferior hypogastric plexus; internal and and all of these segments may be therefore be spoken of as external anal sphincters; lymphatic drainage of rectum and anal canal; retroperitoneal. The precise relationship of the peritoneum to the mesorectum; perineum; rectal blood supply rectum is as follows: the upper third of the rectum is covered by peritoneum on its anterior and lateral surfaces; the middle third of the rectum is covered by peritoneum only on its anterior 1 The rectum is the direct continuation of the sigmoid colon and surface while the lower third of the rectum is below the level of commences in front of the body of the third sacral vertebra. -

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Rectum & Anal Canal
Rectum & Anal canal Dr Brijendra Singh Prof & Head Anatomy AIIMS Rishikesh 27/04/2019 EMBRYOLOGICAL basis – Nerve Supply of GUT •Origin: Foregut (endoderm) •Nerve supply: (Autonomic): Sympathetic Greater Splanchnic T5-T9 + Vagus – Coeliac trunk T12 •Origin: Midgut (endoderm) •Nerve supply: (Autonomic): Sympathetic Lesser Splanchnic T10 T11 + Vagus – Sup Mesenteric artery L1 •Origin: Hindgut (endoderm) •Nerve supply: (Autonomic): Sympathetic Least Splanchnic T12 L1 + Hypogastric S2S3S4 – Inferior Mesenteric Artery L3 •Origin :lower 1/3 of anal canal – ectoderm •Nerve Supply: Somatic (inferior rectal Nerves) Rectum •Straight – quadrupeds •Curved anteriorly – puborectalis levator ani •Part of large intestine – continuation of sigmoid colon , but lacks Mesentery , taeniae coli , sacculations & haustrations & appendices epiploicae. •Starts – S3 anorectal junction – ant to tip of coccyx – apex of prostate •12 cms – 5 inches - transverse slit •Ampulla – lower part Development •Mucosa above Houstons 3rd valve endoderm pre allantoic part of hind gut. •Mucosa below Houstons 3rd valve upto anal valves – endoderm from dorsal part of endodermal cloaca. •Musculature of rectum is derived from splanchnic mesoderm surrounding cloaca. •Proctodeum the surface ectoderm – muco- cutaneous junction. •Anal membrane disappears – and rectum communicates outside through anal canal. Location & peritoneal relations of Rectum S3 1 inch infront of coccyx Rectum • Beginning: continuation of sigmoid colon at S3. • Termination: continues as anal canal, • one inch below -
Pubid-1446077038.Pdf
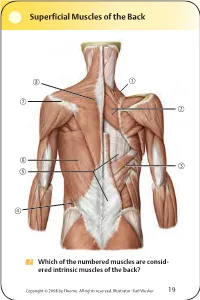
Superficial Muscles of the Back Which of the numbered muscles are consid- ered intrinsic muscles of the back? Copyright © 2008 by Thieme. All rights reserved. Illustrator: Karl Wesker 19 Superficial Muscles of the Back Posterior view. A Levator scapulae S Rhomboideus major D Serratus posterior inferior F Lumbar triangle, internal oblique G Thoracolumbar fascia, superficial layer H Latissimus dorsi J Scapular spine K Trapezius, transverse part Only the serratus posterior inferior is an intrinsic muscle of the back. The trapezius, latissimus dorsi, leva- tor scapulae, and rhomboideus muscles assist in move- ment of the shoulder or arm and are considered muscles of the upper limb. Fig. 2.1. Gilroy, MacPherson, Ross, Atlas of Anatomy, p. 22. Course of the Intercostal Nerves Copyright © 2008 by Thieme. All rights reserved. Illustrator: Markus Voll 39 Course of the Intercostal Nerves Coronal section. Anterior view. A Visceral pleura S Parietal pleura, diaphragmatic part D Diaphragm F Costodiaphragmatic recess G Endothoracic fascia H External intercostal J Costal groove K Intercostal vein, artery, and nerve Abnormal fluid collection in the pleural space (e.g., pleural effusion due to bronchial carcinoma) may necessitate the insertion of a chest tube. Generally, the optimal puncture site in a sitting patient is at the level of the 7th or 8th intercostal space on the posterior axillary line. The drain should always be introduced at the upper margin of a rib to avoid injuring the intercostal vein, artery, and nerve. Fig. 5.24. From Atlas of Anatomy, p. 59. Copyright ©2008 byThieme. Allrightsreserved. Illustrator: Markus Voll Right Lung 74 Right Lung Lateral and medial views. -
Endolymphatic Sac Tumors: an Overview Michael B
Endolymphatic Sac Tumors: An Overview Michael B. Gluth, MD, FACS Associate Professor Director, Comprehensive Ear & Hearing Ctr. Section of Otolaryngology-Head & Neck Surgery VHL Alliance, Chicago, 2015 Disclosure • No relevant financial interests or other relevant relationships to disclose • Will discuss off-label use of cochlear implants for single-sided SNHL VHL | 2 Outline • What is an endolymphatic sac tumor? • What are the symptoms? • What is the work-up and treatment? VHL | 3 Endolymphatic Sac Anatomy VHL | 4 Endolymphatic Sac Function • Part of the “membranous labyrinth” • Filled with fluid called endolymph • Secretes locally acting chemical called “saccin” • Involved with inner ear fluid homeostasis, mechanisms not fully understood – ELS is involved with Meniere’s disease VHL | 5 ELS Tumors • Extremely rare tumor originating from the endolymphatic sac, only recognized as a unique entity since 1989 • Benign (not cancer) • Highly destructive, slowly progressive – Destroy bone of inner ear, around cranial vault/skull base, and around facial nerve – Can grow into nerves, pass through dura (sac around brain) and press on cerebellum • May be asymptomatic until inner ear is partially destroyed • Key: if hearing loss is present: high chance dura is invaded VHL | 6 Symptoms • Most common presenting symptoms: – Hearing loss (85%) – Visible mass in the ear (50%) – Ringing in the ear (48%) – Facial paralysis (44%) – Dizziness/imbalance (44%) – Headache (37%) – Other neurologic (cranial nerve) weakness (25%) • If present in both ears, outlook -

Female Perineum Doctors Notes Notes/Extra Explanation Please View Our Editing File Before Studying This Lecture to Check for Any Changes
Color Code Important Female Perineum Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, the student should be able to describe the: ✓ Boundaries of the perineum. ✓ Division of perineum into two triangles. ✓ Boundaries & Contents of anal & urogenital triangles. ✓ Lower part of Anal canal. ✓ Boundaries & contents of Ischiorectal fossa. ✓ Innervation, Blood supply and lymphatic drainage of perineum. Lecture Outline ‰ Introduction: • The trunk is divided into 4 main cavities: thoracic, abdominal, pelvic, and perineal. (see image 1) • The pelvis has an inlet and an outlet. (see image 2) The lowest part of the pelvic outlet is the perineum. • The perineum is separated from the pelvic cavity superiorly by the pelvic floor. • The pelvic floor or pelvic diaphragm is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue. (see image 3) We will talk about them more in the next lecture. Image (1) Image (2) Image (3) Note: this image is seen from ABOVE Perineum (In this lecture the boundaries and relations are important) o Perineum is the region of the body below the pelvic diaphragm (The outlet of the pelvis) o It is a diamond shaped area between the thighs. Boundaries: (these are the external or surface boundaries) Anteriorly Laterally Posteriorly Medial surfaces of Intergluteal folds Mons pubis the thighs or cleft Contents: 1. Lower ends of urethra, vagina & anal canal 2. External genitalia 3. Perineal body & Anococcygeal body Extra (we will now talk about these in the next slides) Perineum Extra explanation: The perineal body is an irregular Perineal body fibromuscular mass. -

Scrotal Ultrasound
Scrotal Ultrasound Bruce R. Gilbert, MD, PhD Associate Clinical Professor of Urology & Reproductive Medicine Weill Cornell Medical College Director, Reproductive and Sexual Medicine Smith Institute For Urology North Shore LIJ Health System 1 Developmental Anatomy" Testis and Kidney Hindgut Allantois In the 3-week-old embryo the Primordial primordial germ cells in the wall of germ cells the yolk sac close to the attachment of the allantois migrate along the Heart wall of the hindgut and the dorsal Genital Ridge mesentery into the genital ridge. Yolk Sac Hindgut At 5-weeks the two excretory organs the pronephros and mesonephros systems regress Primordial Pronephric system leaving only the mesonephric duct. germ cells (regressing) Mesonephric The metanephros (adult kidney) system forms from the metanephric (regressing) diverticulum (ureteric bud) and metanephric mass of mesoderm. The ureteric bud develops as a dorsal bud of the mesonephric duct Cloaca near its insertion into the cloaca. Mesonephric Duct Mesonephric Duct Ureteric Bud Ureteric Bud Metanephric system Metanephric system 2 Developmental Anatomy" Wolffian and Mullerian DuctMesonephric Duct Under the influence of SRY, cells in the primitive sex cords differentiate into Sertoli cells forming the testis cords during week 7. Gonads Mesonephros It is at puberty that these testis cords (in Paramesonephric association with germ cells) undergo (Mullerian) Duct canalization into seminiferous tubules. Mesonephric (Wolffian) Duct At 7 weeks the indifferent embryo also has two parallel pairs of genital ducts: the Mesonephric (Wolffian) and the Paramesonephric (Mullerian) ducts. Bladder Bladder Mullerian By week 8 the developing fetal testis tubercle produces at least two hormones: Metanephros 1. A glycoprotein (MIS) produced by the Ureter Uterovaginal fetal Sertoli cells (in response to SRY) primordium Rectum which suppresses unilateral development of the Paramesonephric (Mullerian) duct 2. -

A CASE REPORT and LITERATURE REVIEW Dr. P
Original Research Paper Volume - 7 | Issue - 6 | June - 2017 | ISSN - 2249-555X | IF : 4.894 | IC Value : 79.96 Medical Science COMBINED ANOMALLY OF RIGHT HEPATIC ARTERY & RIGHT HEPATIC DUCT IN CHOLESYSTECTOMY: A CASE REPORT AND LITERATURE REVIEW Dr. Pankaj Kumar MBBS, MS, Assistant Professor, Medical College Hospital, 88 College Street, Sarkar Kolkata, West Bengal MBBS, MS, RMO cum Clinical Tutor, Medical College Hospital, 88 College Street, Dr. Shibaji Basu Kolkata, West Bengal Dr. Shibsankar MBBS, MS, Associate Professor, Medical College Hospital, 88 College Street, Ray Chaudhury Kolkata, West Bengal ABSTRACT In contrast to the conventional belief that ligation & division of the cystic artery & duct almost completes the operation we would like to say dissection in gall bladder fossa also may be very dangerous. We are presenting a case here to show how dangerous gall bladder fossa may be after an easy Calot's Triangle dissection. A 45 year old female with a history of biliary colic was scheduled for open cholecystectomy. After dissection in Calot's triangle & removal of gall bladder from liver bed it was seen that the right hepatic artery travels a long extra- hepatic course through gall bladder fossa before entering the liver near thefundus of the gall bladder. The right hepatic duct also seen to travel an unusually long extra-hepatic coursethrough the gall bladder fossa before entering into the liver. The right hepatic duct was punctured with fine needle to confirm the presence of bile. KEYWORDS : open cholecystectomy, aberrant right hepatic artery, aberrant right hepatic duct INTRODUCTION the gall bladder after giving off the cystic artery branch. -
Dissertation
A STUDY OF PREVALENCE AND ASSOCIATION OF HYPOTHYROIDISM AND SERUM LIPID PROFILE IN DIAGNOSED GALL STONE DISEASE AT TERTIARY CARE HOSPITAL Dissertation Submitted to THE TAMILNADU Dr. M.G.R MEDICAL UNIVERSITY In partial fulfilment of the requirements for the award of the degree of M.S. GENERAL SURGERY Branch I MAY 2019 CERTIFICATE I This is to certify that this dissertation entitled “A Study of Prevalence and Association of Hypothyroidism and Serum Lipid profile in diagnosed Gall Stone Disease at Tertiary Care Hospital” is a bonafide record of the work done by Dr. Soumya Shree under the supervision and guidance of Dr. R. Maheswari, M.S., Professor, Department of General Surgery, Sree Mookambika Institute of Medical Sciences, Kulasekharam. This is submitted in partial fulfilment of the requirement of The Tamilnadu Dr. M.G.R. Medical University, Chennai for the award of M.S. Degree in General Surgery. Dr. R. Maheswari, M.S., Dr. S. Soundara Rajan, M.S., [Guide] Professor & HOD, Professor, Department Of General Surgery Department Of General Surgery Sree Mookambika Institute of Sree Mookambika Institute of Medical Sciences [SMIMS] Medical Sciences [SMIMS] Kulasekharam, K.K District, Kulasekharam, K.K District, Tamil Nadu -629161 Tamil Nadu -629161 Dr. Rema V. Nair, M.D., D.G.O., [Director] Sree Mookambika Institute of Medical Sciences [SMIMS] Kulasekharam, K.K District, Tamil Nadu -629161 CERTIFICATE II This is to certify that this dissertation work “A Study of Prevalence and Association of Hypothyroidism and Serum Lipid profile in diagnosed Gall Stone Disease at Tertiary Care Hospital” of the candidate Dr. Soumya Shree with registration Number 221611703 for the award of M.S. -

Name: David Daniella Christabel Matric Number: 18/MHS03/002 Department: Anatomy College: Medicine and Health Sciences Course Code: Ana 212
Name: David Daniella Christabel Matric Number: 18/MHS03/002 Department: Anatomy College: Medicine And Health Sciences Course Code: Ana 212 Question: Discuss the anal canal. The anal canal is the terminal segment of the large intestine between the rectum and the anus. The anal canal is located within the anal triangle of the perineum between the right and left ischioanal fosse. It is the final segment of the gastrointestinal tract, around 4cm in length. The canal begins as a continuation of the rectum and passes inferoposteriorly to terminate at the anus. Anal canal is traditionally divided into two segments, upper and lower, separated by the pectinate line also known as the dentate line. Except during defecation, the anal canal is collapsed by the internal and external sphincters to prevent the passage of faecal material. The anal canal is surrounded by internal and external anal sphincters, which play a crucial role in the maintenance of the faecal continence. • Internal Anal Sphincters: surrounds the upper 2/3 of the anal canal. It is formed from a thickening of the involuntary circular smooth muscle in the bowel wall. • External Anal Sphincter: voluntary muscle that surrounds the lower 2/3 of the anal canal (and so overlaps with the internal sphincter). It blends superiorly with the puborecrtalis muscle of the pelvic floor. At the junction of the rectum and the anal canal, there is a muscular ring known as the anorectal ring. It is formed by the fusion of the internal anal sphincter, external anal sphincter and puborectalis muscle, and is palpable on digital rectal examination. -

Morphological and Functional Changes in a New Animal Model Of
Laboratory Investigation (2013) 93, 1001–1011 & 2013 USCAP, Inc All rights reserved 0023-6837/13 Morphological and functional changes in a new animal model of Me´nie`re’s disease Naoya Egami1, Akinobu Kakigi1, Takashi Sakamoto1, Taizo Takeda2, Masamitsu Hyodo2 and Tatsuya Yamasoba1 The purpose of this study was to clarify the underlying mechanism of vertiginous attacks in Me´nie`re’s disease (MD) while obtaining insight into water homeostasis in the inner ear using a new animal model. We conducted both histopatho- logical and functional assessment of the vestibular system in the guinea-pig. In the first experiment, all animals were maintained 1 or 4 weeks after electrocauterization of the endolymphatic sac of the left ear and were given either saline or desmopressin (vasopressin type 2 receptor agonist). The temporal bones from both ears were harvested and the extent of endolymphatic hydrops was quantitatively assessed. In the second experiment, either 1 or 4 weeks after surgery, animals were assessed for balance disorders and nystagmus after the administration of saline or desmopressin. In the first experiment, the proportion of endolymphatic space in the cochlea and the saccule was significantly greater in ears that survived for 4 weeks after surgery and were given desmopressin compared with other groups. In the second experiment, all animals that underwent surgery and were given desmopressin showed spontaneous nystagmus and balance disorder, whereas all animals that had surgery but without desmopressin administration were asymptomatic. Our animal model induced severe endolymphatic hydrops in the cochlea and the saccule, and showed episodes of balance disorder along with spontaneous nystagmus.