Leaning Into Local: Impact of Federalisation on Social
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Mise En Page 1
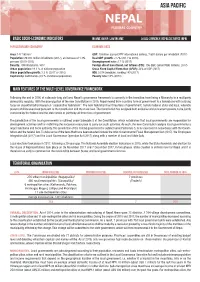
ASIA PACIFIC NEPAL FEDERAL COUNTRY BASIC SOCIO-ECONOMIC INDICATORS INCOME GROUP: LOW INCOME LOCAL CURRENCY: NEPALESE RUPEE (NPR) POPULATION AND GEOGRAPHY ECONOMIC DATA Area: 147 180 km 2 GDP: 79 billion (current PPP international dollars), 2 697 dollars per inhabitant (2017) Population: 29.305 million inhabitants (2017), an increase of 1.2% Real GDP growth: 7.5 % (2017 vs 2016) per year (2010-2015) Unemployment rate: 2.7 % (2017) Density: 199 inhabitants / km 2 Foreign direct investment, net inflows (FDI): 196 (BoP, current USD millions, 2017) Urban population: 19.3 % of national population Gross Fixed Capital Formation (GFCF): 34% of GDP (2017) Urban population growth: 3.2 % (2017 vs 2016) HDI: 0.574 (medium), ranking 149 (2017) Capital city: Kathmandu (4.5 % of national population) Poverty rate: 15% (2010) MAIN FEATURES OF THE MULTI-LEVEL GOVERNANCE FRAMEWORK Following the end in 2006 of a decade-long civil war, Nepal’s governance framework is currently in the transition from being a Monarchy to a multiparty democratic republic. With the promulgation of the new Constitution in 2015, Nepal moved from a unitary form of government to a federal one with a strong focus on decentralization based on “cooperative federalism”. The new federation has three tiers of government, namely federal, state and local, whereby powers shall be exercised pursuant to the Constitution and the state laws. The Constitution has assigned both exclusive and concurrent powers, to be jointly exercised by the federal and the state levels or jointly by all three tiers of government. The jurisdiction of the local governments is outlined under Schedule 8 of the Constitution, which establishes that local governments are responsible for development activities and for mobilizing the necessary resources to carry out such activities. -

Download Publication
No. 43 Working Papers Working Negotiating Between Unequal Neighbours: India‘s Role in Nepal‘s Recent Constitution-Making Process Prakash Bhattarai December 2018 1 Negotiating Between Unequal Neighbours: India’s Role in Nepal’s Recent Constitution-Making Process1 Prakash Bhattarai ABSTRACT Nepal’s post-conflict constitution-making process has seen the involvement of many international actors. While studies on democracy promotion, to this day, mainly focus on Western “donors” and international organizations, this paper looks at the role played by India in the complicated process of moving from a peace agreement to the establishment of an inclusive, democratic constitution in Nepal. More specifically, it is analysed how a powerful neighbouring democracy (India) participated in what is essentially a domestic negotiation process (constitution-making) with a view to influencing the emerging demo- cratic regime. In terms of the issues on the negotiation table, the analysis shows that India, in pushing for an inclusive constitution, pursued the specific agenda of supporting the inclusion of the Madheshis, an ethnic group mostly living in Nepal’s Terai region. In terms of negotiation strategies, the paper identifies four different ways in which India tried to influence the constitution: high-level dialogue; economic blockade; international coalition building; and targeted support of domestic oppositional forces in Nepal. Com- prehensive as this negotiation strategy was, it only met with partial success. Parameters that limited India’s influence included the domestic strength and legitimacy of the official Nepali position (elite alignment; popular support) as well as scepticism concerning In- dia’s role in Nepal, which was reinforced by India’s overly partisan agenda. -

Nepal's Constitution (I): Evolution Not Revolution
NEPAL’S CONSTITUTION (I): EVOLUTION NOT REVOLUTION Asia Report N°233 – 27 August 2012 TABLE OF CONTENTS EXECUTIVE SUMMARY AND RECOMMENDATIONS ................................................. i I. INTRODUCTION ............................................................................................................. 1 II. STEPPING OFF THE EDGE .......................................................................................... 3 A. FRUSTRATED IN FEDERALISM ...................................................................................................... 3 1. The sticking points ....................................................................................................................... 3 2. Bogeymen .................................................................................................................................... 5 3. Missing all the signs ..................................................................................................................... 6 4. The final weeks of the assembly .................................................................................................. 8 5. The mood outside Kathmandu ................................................................................................... 10 B. WHAT HAPPENED ON 27 MAY ................................................................................................... 12 1. Talks ........................................................................................................................................... 12 -
Policy Note for the Federalism Transition in Nepal
Policy Note for the Federalism Transition in Nepal AUGUST 2019 Empowered lives. Resilient nations. Abbreviations and Acronyms CIP Capital Investment Plan FCNA Federalism Capacity Needs Assessment HEZ Himalayan Ecological Zone GDP Gross Domestic Product GRB Gender Responsive Budgeting GESI Gender Equality and Social Inclusion GoN Government of Nepal IPC Inter-Provincial Council LDTA Local Development Training Academy LGCDP Local Governance and Community Development Program LMBIS Line Ministry Budget Information System MOFAGA Ministry of Federal Affairs and General Administration NPSAS National Public Sector Accounting Standards NNRFC National Natural Resource and Fiscal Commission O&M Organization and Management OPMCM Office of the Prime Minister and Council of Ministers PEFA Public Expenditure and Financial Accountability PFM Public Financial Management PIFIP Physical Infrastructure and Facility Improvement Plan PPSC Provincial Public Service Commission PLGs Provincial and Local Governments SUTRA Sub-National Treasury Regulatory Application TEZ Terai Ecological Zone i Table of Contents Abbreviations and Acronyms ........................................................................................................................ i Table of Contents .......................................................................................................................................... ii Foreword .................................................................................................................................................... -

Federalism Is Debated in Nepal More As an ‘Ism’ Than a System
The FEDERALISM Debate in Nepal Post Peace Agreement Constitution Making in Nepal Volume II Post Peace Agreement Constitution Making in Nepal Volume II The FEDERALISM Debate in Nepal Edited by Budhi Karki Rohan Edrisinha Published by United Nations Development Programme (UNDP) Support to Participatory Constitution Building in Nepal (SPCBN) 2014 United Nations Development Programme (UNDP) Support to Participatory Constitution Building in Nepal (SPCBN) UNDP is the UN’s global development network, advocating for change and connecting countries to knowledge, experience and resources to help people build a better life. United Nations Development Programme UN House, Pulchowk, GPO Box: 107 Kathmandu, Nepal Phone: +977 1 5523200 Fax: +977 1 5523991, 5523986 ISBN : 978 9937 8942 1 0 © UNDP, Nepal 2014 Book Cover: The painting on the cover page art is taken from ‘A Federal Life’, a joint publication of UNDP/ SPCBN and Kathmandu University, School of Art. The publication was the culmination of an initiative in which 22 artists came together for a workshop on the concept of and debate on federalism in Nepal and then were invited to depict their perspective on the subject through art. The painting on the cover art titled ‘’Emblem” is created by Supriya Manandhar. DISCLAIMER: The views expressed in the book are those of the authors and do not necessarily represent the views of UNDP/ SPCBN. PREFACE A new Constitution for a new Nepal drafted and adopted by an elected and inclusive Constituent Assembly (CA) is a key element of the Comprehensive Peace Agreement (CPA) of November 2006 that ended a decade long Maoist insurgency. -

Nepal's Constitution (Ii): the Expanding
NEPAL’S CONSTITUTION (II): THE EXPANDING POLITICAL MATRIX Asia Report N°234 – 27 August 2012 TABLE OF CONTENTS EXECUTIVE SUMMARY ...................................................................................................... i I. INTRODUCTION ............................................................................................................. 1 II. THE REVOLUTIONARY SPLIT ................................................................................... 3 A. GROWING APART ......................................................................................................................... 5 B. THE END OF THE MAOIST ARMY .................................................................................................. 7 C. THE NEW MAOIST PARTY ............................................................................................................ 8 1. Short-term strategy ....................................................................................................................... 8 2. Organisation and strength .......................................................................................................... 10 3. The new party’s players ............................................................................................................. 11 D. REBUILDING THE ESTABLISHMENT PARTY ................................................................................. 12 1. Strategy and organisation .......................................................................................................... -

An Application of Doctrine of Necessity: Previous Constituent Assembly of Nepal 117
Jayshwal, An Application of Doctrine of Necessity: Previous Constituent Assembly of Nepal 117 AN APPLICATION OF DOCTRINE OF NECESSITY: PREVIOUS CONSTITUENT ASSEMBLY OF NEPAL AND ITS TIME EXTENSION TO AVOID CONSTITUTIONAL UNCERTAINTY Vijay Pd. Jayshwal* Department of Constitutional Law, Kathmandu School of Law, Dadhikot 09 Purbanchal University-44811, Bhakatpur, New Thimi, Kathmandu, Nepal Abstract This paper aims to investigate issues in relation of constitutional doctrine which had potential debate among the jurists of Nepal for the issues of time extension. The paper will also argue some weaknesses in the constituent assembly and their role expected by the people of Nepal. This paper will discuss about the evolution of constitution in Nepal, its features, the principle of Constitutionalism embodied in Nepalese constitution. This paper will further argue about the legitimacy of Doctrine of Necessity and its application in Nepal. In last, this paper will show the possibility of constitutional uncertainty by newly elected constituent assembly. Keywords: constituent assembly, constitutional uncertainty, constitution. Intisari Penulisan ini dalam rangka mengkaji doktrin konstitusional yang tengah ramai diperdebatkan oleh para ahli hukum di Nepal, khususnya berkaitan dengan isu mengenai perpanjangan waktu. Me- lalui tulisan ini, terdapat temuan yang menunjukkan beberapa kelemahan yang ada dalam majelis konstituate Nepal di samping peran-perannya sebagaimana yang diharapkan oleh rakyat Nepal. Tulisan ini membahas pula mengenai evolusi konstitusi Nepal sebagaimana diwujudkan dalam prinsip-prinsip konstitusionalism yang dianut oleh Konstitusi Nepal. Lebih lanjut, berkaitan de- ngan legitimasi dari Doctrin of Necessity dan penerapannya di Nepal. Pada akhirnya, tulisan ini akan memberikan gambaran mengenai kemungkinan ketidakpastian secara konstitusional berkai- tan dengan kondisi majelis konstituante yang baru saja terpilih. -

How Women Influence Constitution Making After Conflict and Unrest
JANUARY 2018 RESEARCH REPORT AP Photo / Aimen Zine How Women Influence Constitution Making After Conflict and Unrest BY NANAKO TAMARU AND MARIE O’REILLY RESEARCH REPORT | JANUARY 2018 CONTENTS Executive Summary . 1 Introduction: The Global Context . 3 1 | How Do Women Get Access? . 9 2 | What Impact Do Women Have? . 19 3 | Case Study: Women InfluencingConstitution Reform in Tunisia . 30 4 | Challenges to Women’s Influence . 50 5 | Lessons for Action . 56 Annexes . 61 Acknowledgements . 66 PHOTO ON FRONT COVER | Members of the Tunisian National Constituent Assembly celebrate the adoption of the new constitution in Tunis, January 26, 2014 . How Women Influence Constitution Making t RESEARCH REPORT | JANUARY 2018 EXECUTIVE SUMMARY Constitution reform is a frequent feature of peace Despite these hurdles, the cases show that women and transition processes: 75 countries undertook have exerted considerable influence on the decision- constitution reform in the wake of armed conflict, making process, the text of the constitution, and unrest, or negotiated transition from authoritarianism broader prospects for a successful transition to lasting to democracy between 1990 and 2015 . Often peace. Women repeatedly bridged divides in the complementing peace talks, constitutional negotiations negotiating process, contributing to peacebuilding and advance new political settlements, bringing diverse reconciliation in deeply divided societies, while also parties together to agree on how power will be advancing consensus on key issues. They broadened exercised in a country’s future. Increasingly, citizens societal participation and informed policymakers of and international actors alike advocate for participatory citizens’ diverse priorities for the constitution, helping constitution-making processes that include a broader to ensure greater traction for the emerging social cross-section of society—often to address the contract . -

Chronology of Major Political Events in Contemporary Nepal
Chronology of major political events in contemporary Nepal 1846–1951 1962 Nepal is ruled by hereditary prime ministers from the Rana clan Mahendra introduces the Partyless Panchayat System under with Shah kings as figureheads. Prime Minister Padma Shamsher a new constitution which places the monarch at the apex of power. promulgates the country’s first constitution, the Government of Nepal The CPN separates into pro-Moscow and pro-Beijing factions, Act, in 1948 but it is never implemented. beginning the pattern of splits and mergers that has continued to the present. 1951 1963 An armed movement led by the Nepali Congress (NC) party, founded in India, ends Rana rule and restores the primacy of the Shah The 1854 Muluki Ain (Law of the Land) is replaced by the new monarchy. King Tribhuvan announces the election to a constituent Muluki Ain. The old Muluki Ain had stratified the society into a rigid assembly and introduces the Interim Government of Nepal Act 1951. caste hierarchy and regulated all social interactions. The most notable feature was in punishment – the lower one’s position in the hierarchy 1951–59 the higher the punishment for the same crime. Governments form and fall as political parties tussle among 1972 themselves and with an increasingly assertive palace. Tribhuvan’s son, Mahendra, ascends to the throne in 1955 and begins Following Mahendra’s death, Birendra becomes king. consolidating power. 1974 1959 A faction of the CPN announces the formation The first parliamentary election is held under the new Constitution of CPN–Fourth Congress. of the Kingdom of Nepal, drafted by the palace. -

Creating the New Constitution: a Guide for Nepali Citizens
Creating the New Constitution: A Guide for Nepali Citizens Creating the New Constitution: A Guide for Nepali Citizens Editors Yash Ghai Jill Cottrell Contributors Bipin Adhikari Lok Raj Baral Surendra Bhandari Jill Cottrell Yash Ghai Krishna Hachhethu Krishna Khanal Dhruba Kumar Sapana Malla Kumar Regmi Geeta Pathak Sangroula Yubaraj Sangroula Pitamber Sharma Tek Tamrakar Mihir Thakur International IDEA publications are independent of specifi c national or political interests. Views expressed in this publication do not necessarily represent the views of Internatinoal IDEA, its Board or its Council members. @ International Institute for Democracy and Electoral Assistance 2008 Applications for permission to reproduce or translate all or any part of this publication should be made to: International IDEA SE - 103 34 Stockholm Sweden International IDEA encourages dissemination of its work and will promptly respond to request for permission to reproduce or translate its publications. Cover Photo: Deependra Bajracharya Graphic Design: Subarna Humagai ISBN : 978-91-85724-51-2 Preface The International Institute for Democracy and Electoral Assistance (International IDEA) is an intergovernmental organization that supports sustainable democratic change worldwide, including support to the constitution-making process. Since 2006, and on the basis of requests by national parties including political parties and more recently the Constituent Assembly, International IDEA has been providing support to the constitution-making process in Nepal. This support has focused mainly on the pro- visioning of resource materials and the convening of dialogues among national political actors on topics of key importance to the constitutional process. International IDEA will continue supporting the constitution-making process by open- ing avenues through which a broad cross-section of Nepali society can come together to discuss a host of constitutional issues. -

The Abolition of Monarchy and Constitution Making in Nepal
THE KING VERSUS THE PEOPLE(BHANDARI) Article THE KING VERSUS THE PEOPLE: THE ABOLITION OF MONARCHY AND CONSTITUTION MAKING IN NEPAL Surendra BHANDARI Abstract The abolition of the institution of monarchy on May 28, 2008 marks a turning point in the political and constitutional history of Nepal. This saga of constitutional development exemplifies the systemic conflict between people’s’ aspirations for democracy and kings’ ambitions for unlimited power. With the abolition of the monarchy, the process of making a new constitution for the Republic of Nepal has started under the auspices of the Constituent Assembly of Nepal. This paper primarily examines the reasons or causes behind the abolition of monarchy in Nepal. It analyzes the three main reasons for the abolition of monarchy. First, it argues that frequent slights and attacks to constitutionalism by the Nepalese kings had brought the institution of the monarchy to its end. The continuous failures of the early democratic government and the Supreme Court of Nepal in bringing the monarchy within the constitutional framework emphatically weakened the fledgling democracy, but these failures eventually became fatal to the monarchical institution itself. Second, it analyzes the indirect but crucial role of India in the abolition of monarchy. Third, it explains the ten-year-long Maoist insurgency and how the people’s movement culminated with its final blow to the monarchy. Furthermore, this paper also analyzes why the peace and constitution writing process has yet to take concrete shape or make significant process, despite the abolition of the monarchy. Finally, it concludes by recapitulating the main arguments of the paper. -

IFES, Faqs, 'Elections in Nepal: 2020 National Assembly Elections'
Elections in Nepal 2020 National Assembly Elections Frequently Asked Questions Asia-Pacific International Foundation for Electoral Systems 2011 Crystal Drive | Floor 10 | Arlington, VA 22202 | www.IFES.org January 22, 2020 Frequently Asked Questions When is Election Day? ................................................................................................................................... 1 What is the National Assembly and how is it constituted? .......................................................................... 1 Which electoral system will be used in these elections?.............................................................................. 1 What is the structure of the ballots? ............................................................................................................ 1 Who can vote in these elections? ................................................................................................................. 2 What is the process for counting and tabulation? ....................................................................................... 3 Who is eligible to contest these elections? .................................................................................................. 4 Are there reserved seats for women and minorities? .................................................................................. 4 When do elected representatives assume office? ....................................................................................... 4 What is the term of office for