Overcoming the Challenges of COVID-19 Together Responding to a Global Crisis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda
EASE – CA PROJECT PARTNERS EAST AFRICAN CIVIL SOCIETY FOR SUSTAINABLE ENERGY & CLIMATE ACTION (EASE – CA) PROJECT DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda SEPTEMBER 2019 Prepared by: Joint Energy and Environment Projects (JEEP) P. O. Box 4264 Kampala, (Uganda). Supported by Tel: +256 414 578316 / 0772468662 Email: [email protected] JEEP EASE CA PROJECT 1 Website: www.jeepfolkecenter.org East African Civil Society for Sustainable Energy and Climate Action (EASE-CA) Project ALEF Table of Contents ACRONYMS ......................................................................................................................................... 4 ACKNOWLEDGEMENT .................................................................................................................... 5 EXECUTIVE SUMMARY .................................................................................................................. 6 CHAPTER ONE: INTRODUCTION ................................................................................................. 8 1.1 Background of JEEP ............................................................................................................ 8 1.2 Energy situation in Uganda .................................................................................................. 8 1.3 Objectives of the baseline study ......................................................................................... 11 1.4 Report Structure ................................................................................................................ -

Nakaseke Constituency: 109 Nakaseke South County
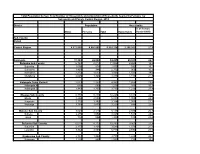
Printed on: Monday, January 18, 2021 16:36:23 PM PRESIDENTIAL ELECTIONS, (Presidential Elections Act, 2005, Section 48) RESULTS TALLY SHEET DISTRICT: 069 NAKASEKE CONSTITUENCY: 109 NAKASEKE SOUTH COUNTY Parish Station Reg. AMURIAT KABULETA KALEMBE KATUMBA KYAGULA MAO MAYAMBA MUGISHA MWESIGYE TUMUKUN YOWERI Valid Invalid Total Voters OBOI KIIZA NANCY JOHN NYI NORBERT LA WILLY MUNTU FRED DE HENRY MUSEVENI Votes Votes Votes PATRICK JOSEPH LINDA SSENTAMU GREGG KAKURUG TIBUHABU ROBERT U RWA KAGUTA Sub-county: 001 KAASANGOMBE 014 BUKUUKU 01 TIMUNA/KAFENE 716 1 0 1 0 278 2 0 1 0 1 140 424 43 467 0.24% 0.00% 0.24% 0.00% 65.57% 0.47% 0.00% 0.24% 0.00% 0.24% 33.02% 9.21% 65.22% 02 LUKYAMU PR. SCHOOL 778 2 2 0 1 348 2 2 0 1 0 110 468 24 492 0.43% 0.43% 0.00% 0.21% 74.36% 0.43% 0.43% 0.00% 0.21% 0.00% 23.50% 4.88% 63.24% 03 BUKUUKU PRI. SCHOOL 529 0 0 1 1 188 0 1 0 0 0 74 265 3 268 0.00% 0.00% 0.38% 0.38% 70.94% 0.00% 0.38% 0.00% 0.00% 0.00% 27.92% 1.12% 50.66% Parish Total 2023 3 2 2 2 814 4 3 1 1 1 324 1157 70 1227 0.26% 0.17% 0.17% 0.17% 70.35% 0.35% 0.26% 0.09% 0.09% 0.09% 28.00% 5.70% 60.65% 015 BULYAKE 01 NJAGALABWAMI COMM. -

Nakaseke Makes Model Town Plan
40 The New Vision, FrIday, June 4, 2010 NAKASEKE DISTRICT REVIEW SUPPLEMENT Farmers benefit from Caritas support JOHN KASOZI By John Kasozi education, in August 1993 increased, I got married truck. Next year, he plans he moved to Kampala to the following year.” to buy a plot in Kampala ILSON Nsobya find employment. He initial- Nsobya now has 15 and build a commercial could not ly wanted to work as a acres of land under structure in future. believe, when vehicle mechanic, but he pineapples. He pays school fees Wa lady she met ended up as a cleaner. He notes that on for his four children and six in the bank paid sh24,000 “I decided to go back average an acre of others. as school fees for her home after working for one pineapple brings in about Joyce Kizito, the kindergarten child. That and half years,” says sh5m per year. But with Kamukamu community was in 1993 when his Nsobya. intensive farming, a farmer resource person from monthly pay was One morning in 1994, can garner about sh10m, Kawula, Luweero who sh20,000. Nsobya decided to pack his he says. is also a CARITAS “From that day, I became four-inch mattress, The cost of one pineapple beneficiary says before restless. I wondered how Panasonic radio, a basin ranges between sh600 to they started getting I would pay fees for my and utensils. He used his sh1, 000, Nsobya says support from from the children, rent, feed the savings of sh3,000 for adding that his clientele is organisation in 2002, their family, settle medical transport. -

Pdacl827.Pdf
Promoting Community-Based Distribution / Community Reproductive Health Worker Provision of DMPA Educational Visit to Uganda – Summary Report February 18 – 20, 2008 Family Health International • Plot 6 Kafu Road • Kampala, Uganda • 256 414 235035 TABLE OF CONTENTS I. Executive Summary II. Overview III. Introductory Session with Key Stakeholders in the Uganda CBD of DMPA Project IV. Meeting with Key Stakeholders and District Officials V. Field Trip to Luwero and Nakaseke Districts VI. Debriefing with Key Stakeholders and District Officials VII. The Way Forward – Country Team Planning Sessions VIII. Tour Reflections and Take-home Messages IX. Conclusion Appendices: A: List of Participants B: Educational Tour Program E: Contents List of Informational Packages Provided to Delegates ACRONYMS ARFH Association for Reproductive and Family Health CBD Community-based Distributors/Distribution CPR Contraceptive Prevalence Rate CBD AGENT Community Reproductive Health Worker CTPH Conservation Through Public Health DDHS District Director of Health Services DMPA Depot-Medroxyprogesterone Acetate (Also called Depo-Provera) EH EngenderHealth FHI Family Health International FP Family Planning MIHV Minnesota Health Volunteers MOH Ministry of Health NGO Nongovernmental Organization RH Reproductive Health RHD Reproductive Health Division SC Save the Children TFR Total Fertility Rate USAID United States Agency for International Development I. EXECUTIVE SUMMARY Agenda An educational tour to Uganda on February 18–20 provided delegates from other countries with an introduction to the community-based distribution (CBD) of the injectable contraceptive DMPA (depot medroxyprogesterone acetate, or Depo Provera). The goal was to learn about Uganda’s experiences with the CBD of DMPA and to forge relationships between the delegates so that they could exchange information about such programs in their home countries. -

Challenges of Development and Natural Resource Governance In
Ian Karusigarira Uganda’s revolutionary memory, victimhood and regime survival The road that the community expects to take in each generation is inspired and shaped by its memories of former heroic ages —Smith, D.A. (2009) Ian Karusigarira PhD Candidate, Graduate School of Global Studies, Tokyo University of Foreign Studies, Japan Abstract In revolutionary political systems—such as Uganda’s—lies a strong collective memory that organizes and enforces national identity as a cultural property. National identity nurtured by the nexus between lived representations and narratives on collective memory of war, therefore, presents itself as a kind of politics with repetitive series of nation-state narratives, metaphorically suggesting how the putative qualities of the nation’s past reinforce the qualities of the present. This has two implications; it on one hand allows for changes in a narrative's cognitive claims which form core of its constitutive assumptions about the nation’s past. This past is collectively viewed as a fight against profanity and restoration of political sanctity; On the other hand, it subjects memory to new scientific heuristics involving its interpretations, transformation and distribution. I seek to interrogate the intricate memory entanglement in gaining and consolidating political power in Uganda. Of great importance are politics of remembering, forgetting and utter repudiation of memory of war while asserting control and restraint over who governs. The purpose of this paper is to understand and internalize the dynamics of how knowledge of the past relates with the present. This gives a precise definition of power in revolutionary-dominated regimes. Keywords: Memory of War, national narratives, victimhood, regime survival, Uganda ―75― 本稿の著作権は著者が保持し、クリエイティブ・コモンズ表示4.0国際ライセンス(CC-BY)下に提供します。 https://creativecommons.org/licenses/by/4.0/deed.ja Uganda’s revolutionary memory, victimhood and regime survival 1. -

Typhoid Over Diagnosis in Nakaseke District, June 2016
Public Health Fellowship Program – Field Epidemiology Track Typhoid Over diagnosis in Nakaseke District, June 2016 Dr. Kusiima Joy, MBChB-MHSR Fellow,2016 Typhoid Alert May June 2016 2016 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Notification Data Audit ,12 health Reviewed HMIS data facilities Nakaseke 84 cases/ 50,000 by FFETP(wk 15-21) Typhoid Outbreak verification exercise 323 Typhoid cases reported 2 Typhoid verification in Nakaseke District Objectives . Verify the existence of an outbreak . Verify reported diagnosis using standard case definition . Recommend public health action 3 Typhoid verification in Nakaseke District District location 4 Typhoid verification in Nakaseke District Facilities selected . Private hospital - Kiwoko . Government hospital - Nakaseke . Health center IV - Semuto . Health center III - Kapeeka 5 Typhoid verification in Nakaseke District Data collection . Extracted records from registers (1st/12/ 2015 to 14th/06/2016) . Discussed with clinicians & lab personnel . Took clinical history &examined typhoid suspects 6 Typhoid verification in Nakaseke District Standard case definition . Suspected case: Onset of fever ≥3days,negative malaria test, resident of Nakaseke district Plus any of following: chills, malaise, headache, sore throat, cough, abdominal pain, constipation, diarrhea . Probable case: Suspected case plus positive antigen test (Widal) . Confirmed case: Suspected case plus salmonella typhi (+) blood or stool by culture 7 Typhoid verification in Nakaseke District Data quality assessment . Reviewed laboratory -
Population by Parish
Total Population by Sex, Total Number of Households and proportion of Households headed by Females by Subcounty and Parish, Central Region, 2014 District Population Households % of Female Males Females Total Households Headed HHS Sub-County Parish Central Region 4,672,658 4,856,580 9,529,238 2,298,942 27.5 Kalangala 31,349 22,944 54,293 20,041 22.7 Bujumba Sub County 6,743 4,813 11,556 4,453 19.3 Bujumba 1,096 874 1,970 592 19.1 Bunyama 1,428 944 2,372 962 16.2 Bwendero 2,214 1,627 3,841 1,586 19.0 Mulabana 2,005 1,368 3,373 1,313 21.9 Kalangala Town Council 2,623 2,357 4,980 1,604 29.4 Kalangala A 680 590 1,270 385 35.8 Kalangala B 1,943 1,767 3,710 1,219 27.4 Mugoye Sub County 6,777 5,447 12,224 3,811 23.9 Bbeta 3,246 2,585 5,831 1,909 24.9 Kagulube 1,772 1,392 3,164 1,003 23.3 Kayunga 1,759 1,470 3,229 899 22.6 Bubeke Sub County 3,023 2,110 5,133 2,036 26.7 Bubeke 2,275 1,554 3,829 1,518 28.0 Jaana 748 556 1,304 518 23.0 Bufumira Sub County 6,019 4,273 10,292 3,967 22.8 Bufumira 2,177 1,404 3,581 1,373 21.4 Lulamba 3,842 2,869 6,711 2,594 23.5 Kyamuswa Sub County 2,733 1,998 4,731 1,820 20.3 Buwanga 1,226 865 2,091 770 19.5 Buzingo 1,507 1,133 2,640 1,050 20.9 Maziga Sub County 3,431 1,946 5,377 2,350 20.8 Buggala 2,190 1,228 3,418 1,484 21.4 Butulume 1,241 718 1,959 866 19.9 Kampala District 712,762 794,318 1,507,080 414,406 30.3 Central Division 37,435 37,733 75,168 23,142 32.7 Bukesa 4,326 4,711 9,037 2,809 37.0 Civic Centre 224 151 375 161 14.9 Industrial Area 383 262 645 259 13.9 Kagugube 2,983 3,246 6,229 2,608 42.7 Kamwokya -
Legend " Wanseko " 159 !
CONSTITUENT MAP FOR UGANDA_ELECTORAL AREAS 2016 CONSTITUENT MAP FOR UGANDA GAZETTED ELECTORAL AREAS FOR 2016 GENERAL ELECTIONS CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY 266 LAMWO CTY 51 TOROMA CTY 101 BULAMOGI CTY 154 ERUTR CTY NORTH 165 KOBOKO MC 52 KABERAMAIDO CTY 102 KIGULU CTY SOUTH 155 DOKOLO SOUTH CTY Pirre 1 BUSIRO CTY EST 53 SERERE CTY 103 KIGULU CTY NORTH 156 DOKOLO NORTH CTY !. Agoro 2 BUSIRO CTY NORTH 54 KASILO CTY 104 IGANGA MC 157 MOROTO CTY !. 58 3 BUSIRO CTY SOUTH 55 KACHUMBALU CTY 105 BUGWERI CTY 158 AJURI CTY SOUTH SUDAN Morungole 4 KYADDONDO CTY EST 56 BUKEDEA CTY 106 BUNYA CTY EST 159 KOLE SOUTH CTY Metuli Lotuturu !. !. Kimion 5 KYADDONDO CTY NORTH 57 DODOTH WEST CTY 107 BUNYA CTY SOUTH 160 KOLE NORTH CTY !. "57 !. 6 KIIRA MC 58 DODOTH EST CTY 108 BUNYA CTY WEST 161 OYAM CTY SOUTH Apok !. 7 EBB MC 59 TEPETH CTY 109 BUNGOKHO CTY SOUTH 162 OYAM CTY NORTH 8 MUKONO CTY SOUTH 60 MOROTO MC 110 BUNGOKHO CTY NORTH 163 KOBOKO MC 173 " 9 MUKONO CTY NORTH 61 MATHENUKO CTY 111 MBALE MC 164 VURA CTY 180 Madi Opei Loitanit Midigo Kaabong 10 NAKIFUMA CTY 62 PIAN CTY 112 KABALE MC 165 UPPER MADI CTY NIMULE Lokung Paloga !. !. µ !. "!. 11 BUIKWE CTY WEST 63 CHEKWIL CTY 113 MITYANA CTY SOUTH 166 TEREGO EST CTY Dufile "!. !. LAMWO !. KAABONG 177 YUMBE Nimule " Akilok 12 BUIKWE CTY SOUTH 64 BAMBA CTY 114 MITYANA CTY NORTH 168 ARUA MC Rumogi MOYO !. !. Oraba Ludara !. " Karenga 13 BUIKWE CTY NORTH 65 BUGHENDERA CTY 115 BUSUJJU 169 LOWER MADI CTY !. -

Client Satisfaction with Health Insurance in Uganda
Client Satisfaction with Health Insurance - Uganda CLIENT SATISFACTION WITH HEALTH INSURANCE IN UGANDA 1 Client Satisfaction with Health Insurance - Uganda TABLE OF CONTENTS I INTRODUCTION ..................................................................................................................................................... 6 II RESEARCH OVERVIEW ..................................................................................................................................... 6 RESEARCH OBJECTIVE ............................................................................................................................................... 6 RESEARCH METHODS ................................................................................................................................................ 6 RESEARCH SAMPLE ................................................................................................................................................... 7 REPORT OUTLINE ...................................................................................................................................................... 7 III SAVE FOR HEALTH UGANDA (SHU) ............................................................................................................. 8 BACKGROUND ON SAVE FOR HEALTH UGANDA (SHU) ............................................................................................. 8 THE KAMULI MUGANZI AWONGERWA ASSOCIATION – INSURANCE/CREDIT SCHEME .............................................. 8 -

NAKASEKE DLG Q4 REPORT.Pdf
Local Government Quarterly Performance Report Vote: 569 Nakaseke District 2016/17 Quarter 4 Structure of Quarterly Performance Report Summary Quarterly Department Workplan Performance Cumulative Department Workplan Performance Location of Transfers to Lower Local Services and Capital Investments Submission checklist I hereby submit _________________________________________________________________________. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:569 Nakaseke District for FY 2016/17. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Chief Administrative Officer, Nakaseke District Date: 8/23/2017 cc. The LCV Chairperson (District)/ The Mayor (Municipality) Page 1 Local Government Quarterly Performance Report Vote: 569 Nakaseke District 2016/17 Quarter 4 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Cumulative Receipts Performance Approved Budget Cumulative % UShs 000's Receipts Budget Received 1. Locally Raised Revenues 1,338,786 1,704,820 127% 2a. Discretionary Government Transfers 3,314,474 3,260,284 98% 2b. Conditional Government Transfers 16,270,489 15,459,486 95% 2c. Other Government Transfers 948,643 966,847 102% 4. Donor Funding 22,900 Total Revenues 21,872,393 21,414,338 98% Overall Expenditure Performance Cumulative Releases and Expenditure Perfromance Approved Budget Cumulative Cumulative % % % UShs 000's Releases Expenditure -

Estimated Land Area and Projected Population by Sex by Lower Local
Table 1.1 : Estimated Land Area and Projected Population by Sex by Lower Local Government Cost Vote Lower Local Estimated District Center ID Code Government Land Area Male Female Total Abim 75,500 78,000 153,500 237254 573 Abim 183.9 8,900 9,100 18,000 237249 573 Abim Town Council 110.7 12,100 12,300 24,400 237252 573 Alerek 927.5 6,500 6,600 13,100 237250 573 Lotukei 71.5 8,300 8,800 17,100 237251 573 Morulem 274.0 15,900 16,500 32,400 237253 573 Nyakwae 343.5 10,400 10,800 21,200 237256 573 Awach 118.9 7,800 7,800 15,600 237255 573 Magamaga 321.7 5,600 6,100 11,700 Adjumani 112,600 123,300 235,900 236327 501 Adjumani Town Council 15.6 17,700 19,400 37,100 236322 501 Adropi 78.1 6,100 6,200 12,300 236320 501 Arinyapi 184.9 6,000 6,200 12,200 236324 501 Ciforo 167.6 7,400 7,700 15,100 236319 501 Dzaipi 237.1 21,000 24,000 45,000 236328 501 Itirikwa 708.0 8,500 9,400 17,900 236323 501 Ofua 79.5 7,000 7,700 14,700 236325 501 Pacara 194.4 8,700 9,300 18,000 236326 501 Pakele 604.0 24,400 27,300 51,700 236321 501 Ukusijoni 685.4 5,800 6,100 11,900 Agago 121,900 129,300 251,200 237587 611 Adilang 390.4 10,900 11,400 22,300 237590 611 Agago Town Council 49.2 3,200 3,500 6,700 237591 611 Arum 198.8 6,400 6,600 13,000 237594 611 Kalongo Town Council 26.5 5,900 6,900 12,800 237583 611 Kotomol 160.7 6,700 7,100 13,800 237596 611 Lamiyo 138.9 4,500 4,900 9,400 237584 611 Lapono 465.0 11,800 12,500 24,300 237588 611 Lira Palwo 239.8 8,700 9,300 18,000 237597 611 Lokole 293.8 8,300 8,800 17,100 237592 611 Omiya Pacwa 320.7 6,200 6,600 12,800 237582 -

Evaluating Local, National, Regional and International Interventions in Northern Uganda Using a Human Security Approach
The University of Notre Dame Australia ResearchOnline@ND Theses 2019 Evaluating local, national, regional and international interventions in northern Uganda using a human security approach Davis Kawooya The University of Notre Dame Australia Follow this and additional works at: https://researchonline.nd.edu.au/theses Part of the Arts and Humanities Commons COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING The material in this communication may be subject to copyright under the Act. Any further copying or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice. Publication Details Kawooya, D. (2019). Evaluating local, national, regional and international interventions in northern Uganda using a human security approach (Doctor of Philosophy (College of Arts and Science)). University of Notre Dame Australia. https://researchonline.nd.edu.au/theses/230 This dissertation/thesis is brought to you by ResearchOnline@ND. It has been accepted for inclusion in Theses by an authorized administrator of ResearchOnline@ND. For more information, please contact [email protected]. Evaluating local, national, regional and international interventions in northern Uganda using a human security approach by Davis Lubwama Kawooya A thesis submitted to The University of Notre Dame Australia to fulfil the partial requirements for the degree of Doctor of Philosophy School of Arts and Sciences The University of Notre Dame Australia 2019 ii Author’s Declaration I, Davis Lubwama Kawooya to the best of my knowledge, declare that this is my original work and has not been submitted for a degree or a diploma in any other university.