Report of the Expert Committee on the Diagnosis and Classification Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 7: Monogenic Forms of Diabetes
CHAPTER 7 MONOGENIC FORMS OF DIABETES Mark A. Sperling, MD, and Abhimanyu Garg, MD Dr. Mark A. Sperling is Emeritus Professor and Chair, University of Pittsburgh, Department of Pediatrics, Children’s Hospital of Pittsburgh of UPMC, Pittsburgh, PA. Dr. Abhimanyu Garg is Professor of Internal Medicine and Chief of the Division of Nutrition and Metabolic Diseases at University of Texas Southwestern Medical Center, Dallas, TX. SUMMARY Types 1 and 2 diabetes have multiple and complex genetic influences that interact with environmental triggers, such as viral infections or nutritional excesses, to result in their respective phenotypes: young, lean, and insulin-dependence for type 1 diabetes patients or older, overweight, and often manageable by lifestyle interventions and oral medications for type 2 diabetes patients. A small subset of patients, comprising ~2%–3% of all those diagnosed with diabetes, may have characteristics of either type 1 or type 2 diabetes but have single gene defects that interfere with insulin production, secretion, or action, resulting in clinical diabetes. These types of diabetes are known as MODY, originally defined as maturity-onset diabetes of youth, and severe early-onset forms, such as neonatal diabetes mellitus (NDM). Defects in genes involved in adipocyte development, differentiation, and death pathways cause lipodystrophy syndromes, which are also associated with insulin resistance and diabetes. Although these syndromes are considered rare, more awareness of these disorders and increased availability of genetic testing in clinical and research laboratories, as well as growing use of next generation, whole genome, or exome sequencing for clinically challenging phenotypes, are resulting in increased recognition. A correct diagnosis of MODY, NDM, or lipodystrophy syndromes has profound implications for treatment, genetic counseling, and prognosis. -

Divergent Genes in Gerbils: Prevalence, Relation to GC-Biased Substitution, and Phenotypic Relevance Yichen Dai, Rodrigo Pracana and Peter W
Dai et al. BMC Evolutionary Biology (2020) 20:134 https://doi.org/10.1186/s12862-020-01696-3 RESEARCH ARTICLE Open Access Divergent genes in gerbils: prevalence, relation to GC-biased substitution, and phenotypic relevance Yichen Dai, Rodrigo Pracana and Peter W. H. Holland* Abstract Background: Two gerbil species, sand rat (Psammomys obesus) and Mongolian jird (Meriones unguiculatus), can become obese and show signs of metabolic dysregulation when maintained on standard laboratory diets. The genetic basis of this phenotype is unknown. Recently, genome sequencing has uncovered very unusual regions of high guanine and cytosine (GC) content scattered across the sand rat genome, most likely generated by extreme and localized biased gene conversion. A key pancreatic transcription factor PDX1 is encoded by a gene in the most extreme GC-rich region, is remarkably divergent and exhibits altered biochemical properties. Here, we ask if gerbils have proteins in addition to PDX1 that are aberrantly divergent in amino acid sequence, whether they have also become divergent due to GC-biased nucleotide changes, and whether these proteins could plausibly be connected to metabolic dysfunction exhibited by gerbils. Results: We analyzed ~ 10,000 proteins with 1-to-1 orthologues in human and rodents and identified 50 proteins that accumulated unusually high levels of amino acid change in the sand rat and 41 in Mongolian jird. We show that more than half of the aberrantly divergent proteins are associated with GC biased nucleotide change and many are in previously defined high GC regions. We highlight four aberrantly divergent gerbil proteins, PDX1, INSR, MEDAG and SPP1, that may plausibly be associated with dietary metabolism. -

Genes in Eyecare Geneseyedoc 3 W.M
Genes in Eyecare geneseyedoc 3 W.M. Lyle and T.D. Williams 15 Mar 04 This information has been gathered from several sources; however, the principal source is V. A. McKusick’s Mendelian Inheritance in Man on CD-ROM. Baltimore, Johns Hopkins University Press, 1998. Other sources include McKusick’s, Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. Baltimore. Johns Hopkins University Press 1998 (12th edition). http://www.ncbi.nlm.nih.gov/Omim See also S.P.Daiger, L.S. Sullivan, and B.J.F. Rossiter Ret Net http://www.sph.uth.tmc.edu/Retnet disease.htm/. Also E.I. Traboulsi’s, Genetic Diseases of the Eye, New York, Oxford University Press, 1998. And Genetics in Primary Eyecare and Clinical Medicine by M.R. Seashore and R.S.Wappner, Appleton and Lange 1996. M. Ridley’s book Genome published in 2000 by Perennial provides additional information. Ridley estimates that we have 60,000 to 80,000 genes. See also R.M. Henig’s book The Monk in the Garden: The Lost and Found Genius of Gregor Mendel, published by Houghton Mifflin in 2001 which tells about the Father of Genetics. The 3rd edition of F. H. Roy’s book Ocular Syndromes and Systemic Diseases published by Lippincott Williams & Wilkins in 2002 facilitates differential diagnosis. Additional information is provided in D. Pavan-Langston’s Manual of Ocular Diagnosis and Therapy (5th edition) published by Lippincott Williams & Wilkins in 2002. M.A. Foote wrote Basic Human Genetics for Medical Writers in the AMWA Journal 2002;17:7-17. A compilation such as this might suggest that one gene = one disease. -

Intraceuular Transport and Sorting of Mutant Human Proinsulins That Fail to Form Hexamers David Quinn,* Lelio Orci,* Mariella Ravazzola,~ and Hsiao-Ping H
IntraceUular Transport and Sorting of Mutant Human Proinsulins that Fail to Form Hexamers David Quinn,* Lelio Orci,* Mariella Ravazzola,~ and Hsiao-Ping H. Moore* * Department of Molecular and Cell Biology, Life Sciences Addition, University of California, Berkeley, California 94720; and *Department of Morphology, University of Geneva Medical School, Geneva, Switzerland Abstract. Human proinsulin and insulin oligomerize both dimers and hexamers. The mutants were trans- to form dimers and hemmers. It has been suggested fected into the mouse pituitary AtT-20 cells, and their that the ability of prohormones to self associate and ability to be sorted into regulated secretory granules form aggregates may be responsible for the sorting was compared to wild-type insulin. We found that process at the trans-Golgi. To examine whether insulin while B10His-~p is sorted somewhat less efficiently than oligomerization is required for proper sorting into reg- wild-type insulin as reported previously (Carroll, R. J., ulated storage granules, we have constructed point R. E. Hammer, S. J. Chan, H. H. Swift, A. H. Ruben- mutations in human insulin B chain that have been stein, and D. E Steiner. 1988. Proc. Natl. Acad. Sci. previously shown to prevent formation of insulin hexa- USA. 85:8943-8947; Gross, D. J., P. A. Halban, C. R. mers (Brange, J., U. Ribel, J. E Hansen, G. Dodson, Kahn, G. C. Weir, and L. Villa-Kumaroff. 1989. Proc. M. T. Hansen, S. Havelund, S. G. Melberg, E Norris, Natl. Acad. Sci. USA. 86:4107-4111). B9Se~p is tar- K. Norris, L. Snel, A. R. Sorensen, and H. -

The Un-Design and Design of Insulin: Structural Evolution
THE UN-DESIGN AND DESIGN OF INSULIN: STRUCTURAL EVOLUTION WITH APPLICATION TO THERAPEUTIC DESIGN By NISCHAY K. REGE Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of Biochemistry Dissertation Advisor: Dr. Michael A. Weiss CASE WESTERN RESERVE UNIVERSITY August, 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis/dissertation of Nischay K. Rege candidate for the degree of Doctor of Philosophy*. Committee Chair Paul Carey Committee Member Michael Weiss Committee Member Faramarz Ismail-Beigi Committee Member George Dubyak Date of Defense: June 26th, 2018 *We also certify that written approval has been obtained for any proprietary material contained therein. Dedication This thesis is dedicated to my mother, Dipti, whose constant love and faith have never failed, to my father, Kiran, who taught me of the virtue of curiosity, and to my wife, Shipra, whose kindness and companionship have given me enough strength for eight lifetimes. i Table of Contents Dedication ..................................................................................................................................... i Table of Contents ......................................................................................................................... ii List of Tables ............................................................................................................................... v List of Figures ........................................................................................................................... -

Nutrient Control of Mrna Translation
NU40CH07_Qian ARjats.cls June 24, 2020 11:31 Annual Review of Nutrition Nutrient Control of mRNA Translation Xin Erica Shu,1 Robert V. Swanda,2 and Shu-Bing Qian1,2 1Division of Nutritional Sciences, Cornell University, Ithaca, New York 14853, USA; email: [email protected] 2Department of Biomedical and Biological Sciences, Cornell University, Ithaca, New York 14853, USA Annu. Rev. Nutr. 2020. 40:7.1–7.25 Keywords The Annual Review of Nutrition is online at amino acids, mRNA translation, ribosome, mTOR, O-GlcNAcylation, nutr.annualreviews.org methylation https://doi.org/10.1146/annurev-nutr-120919- 041411 Abstract Copyright © 2020 by Annual Reviews. The emergence of genome-wide analyses to interrogate cellular DNA, All rights reserved Annu. Rev. Nutr. 2020.40. Downloaded from www.annualreviews.org RNA, and protein content has revolutionized the study of control networks Access provided by Cornell University on 08/04/20. For personal use only. that mediate cellular homeostasis. mRNA translation represents the last step of genetic flow and primarily defines the proteome. Translational regulation is thus critical for gene expression, in particular under nutrient excess or deficiency. Until recently, it was unclear how the global effects of transla- tional control are orchestrated by nutrient signaling pathways. An emerging concept of translational reprogramming addresses how to maintain the ex- pression of specific proteins during nutrient stress by translation of selective mRNAs. In this review, we describe recent advances in our understanding of translational control principles; nutrient-sensing mechanisms; and their dysregulation in human diseases such as diabetes, cancer, and aging. The mechanistic understanding of translational regulation in response to differ- ent nutrient conditions may help identify potential dietary and therapeutic targets to improve human health. -

USDA/APHIS Environmental Assessment
USDA-APHIS Environmental Assessment In response to permit application (06-363-103r), received from SemBioSys, Inc. for a field-test to produce human proinsulin (line 4438-5A) in genetically engineered safflower (Carthamus tinctorius) seeds U.S. Department of Agriculture Animal and Plant Health Inspection Service Biotechnology Regulatory Services 06_363103r_062207 TABLE OF CONTENTS TABLE OF CONTENTS............................................................................................................................. 2 I. SUMMARY .................................................................................................................................... 3 II. INTRODUCTION.......................................................................................................................... 3 A. USDA REGULATORY AUTHORITY .................................................................................................... 3 B. FOOD AND DRUG ADMINISTRATION (FDA) REGULATORY AUTHORITY ........................................... 4 III. PURPOSE AND NEED ................................................................................................................. 4 IV. ALTERNATIVES .......................................................................................................................... 4 A. NO ACTION: DO NOT ALLOW PLANTING TO INCREASE SEED PRODUCTION ........................................ 5 B. ISSUE THE PERMIT: ALLOW PLANTING WITH SUPPLEMENTAL CONDITIONS ....................................... 5 C. PREFERRED -

Endocrine Test Selection and Interpretation
The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition Edited by: Delbert A. Fisher, MD Senior Science Officer Quest Diagnostics Nichols Institute Professor Emeritus, Pediatrics and Medicine UCLA School of Medicine Consulting Editors: Wael Salameh, MD, FACP Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute San Juan Capistrano, CA Associate Clinical Professor of Medicine, David Geffen School of Medicine at UCLA Richard W. Furlanetto, MD, PhD Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute Chantilly, VA ©2007 Quest Diagnostics Incorporated. All rights reserved. Fourth Edition Printed in the United States of America Quest, Quest Diagnostics, the associated logo, Nichols Institute, and all associated Quest Diagnostics marks are the trademarks of Quest Diagnostics. All third party marks − ®' and ™' − are the property of their respective owners. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, and information storage and retrieval system, without permission in writing from the publisher. Address inquiries to the Medical Information Department, Quest Diagnostics Nichols Institute, 33608 Ortega Highway, San Juan Capistrano, CA 92690-6130. Previous editions copyrighted in 1996, 1998, and 2004. Re-order # IG1984 Forward Quest Diagnostics Nichols Institute has been -

Whole Exome Sequencing Gene Package Multiple Congenital Anomaly, Version 8.1, 31-1-2020
Whole Exome Sequencing Gene package Multiple congenital anomaly, version 8.1, 31-1-2020 Technical information DNA was enriched using Agilent SureSelect DNA + SureSelect OneSeq 300kb CNV Backbone + Human All Exon V7 capture and paired-end sequenced on the Illumina platform (outsourced). The aim is to obtain 10 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate and non-unique reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA-MEM algorithm (reference: http://bio-bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x A4GALT [Blood group, P1Pk system, P(2) phenotype], 111400 [Blood group, P1Pk system, p phenotype], 111400 NOR poly607922 146 100 100 99 AAAS Achalasia-addisonianism-alacrimia syndrome, 231550 605378 102 100 100 100 -
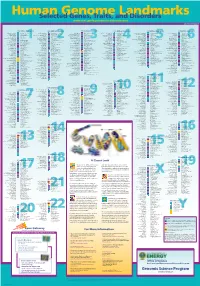
Genomeposter2009.Pdf
Fold HumanSelected Genome Genes, Traits, and Landmarks Disorders www.ornl.gov/hgmis/posters/chromosome genomics.energy. -

Hyperproinsulinemia Is Not a Characteristic Feature in the Offspring of Patients with Different Phenotypes of Type II Diabetes
European Journal of Endocrinology (2000) 143 251±260 ISSN 0804-4643 CLINICAL STUDY Hyperproinsulinemia is not a characteristic feature in the offspring of patients with different phenotypes of type II diabetes Ilkka K J Vauhkonen1, Leo K Niskanen1, Leena MykkaÈnen3, Steven M Haffner3, Matti I J Uusitupa2 and Markku Laakso1 Departments of 1Medicine and 2Clinical Nutrition, Kuopio University Hospital and University of Kuopio, Kuopio, Finland, and 3Department of Medicine/Division of Clinical Epidemiology, University of Texas, San Antonio, Texas, USA (Correspondence should be addressed to M Laakso, Department of Medicine, University of Kuopio, FIN-70210 Kuopio, Finland; Fax: +358-17-173993) Abstract Objective: The purpose of this work was to study whether there are differences in plasma proinsulin levels and proinsulin-to-speci®c insulin ratio in the offspring of patients with different phenotypes of type II diabetes. Design: Eleven glucose-tolerant offspring of type II diabetic patients with de®cient insulin secretion phenotype (IS group), nine glucose-tolerant offspring of patients with insulin-resistant phenotype (IR group), and fourteen healthy control subjects without a family history of diabetes were studied. Methods: Plasma speci®c insulin, plasma proinsulin, and plasma C-peptide levels were measured during a 2-h oral glucose tolerance test and during hyperglycemic clamp. Results: Plasma proinsulin levels during the oral glucose tolerance test and the hyperglycemic clamp did not differ among the study groups. The IR group had a lower fasting plasma proinsulin-to-speci®c insulin ratio (10.3 6 1.7%) than the control group (15.4 6 1.4%; P < 0.05) and the IS group (18.6 6 2.7%; P < 0.05). -

Test Selection and Interpretation the Quest Diagnostics
The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition The Quest Diagnostics Manual Endocrinology Test Selection and Interpretation Fourth Edition Edited by: Delbert A. Fisher, MD Senior Science Officer Quest Diagnostics Nichols Institute Professor Emeritus, Pediatrics and Medicine UCLA School of Medicine Consulting Editors: Wael Salameh, MD, FACP Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute San Juan Capistrano, CA Associate Clinical Professor of Medicine, David Geffen School of Medicine at UCLA Richard W. Furlanetto, MD, PhD Medical Director, Endocrinology/Metabolism Quest Diagnostics Nichols Institute Chantilly, VA ©2007 Quest Diagnostics Incorporated. All rights reserved. Fourth Edition Printed in the United States of America Quest, Quest Diagnostics, the associated logo, Nichols Institute, and all associated Quest Diagnostics marks are the trademarks of Quest Diagnostics. All third party marks − ®' and ™' − are the property of their respective owners. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, and information storage and retrieval system, without permission in writing from the publisher. Address inquiries to the Medical Information Department, Quest Diagnostics Nichols Institute, 33608 Ortega Highway, San Juan Capistrano, CA 92690-6130. Previous editions copyrighted in 1996, 1998, and 2004. Re-order # IG1984 Forward Quest Diagnostics Nichols Institute has been