Intravenous Salbutamol: Too Much of a Good Thing?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ep 2560611 B1
(19) TZZ Z___T (11) EP 2 560 611 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: A61K 9/00 (2006.01) 03.01.2018 Bulletin 2018/01 (86) International application number: (21) Application number: 11719211.2 PCT/EP2011/056227 (22) Date of filing: 19.04.2011 (87) International publication number: WO 2011/131663 (27.10.2011 Gazette 2011/43) (54) "PROCESS FOR PROVIDING PARTICLES WITH REDUCED ELECTROSTATIC CHARGES" VERFAHREN ZUR BEREITSTELLUNG VON PARTIKELN MIT REDUZIERTEN ELEKTROSTATISCHEN LADUNGEN PROCÉDÉ DE PRÉPARATION DE PARTICULES AYANT DES CHARGES ÉLECTROSTATIQUES RÉDUITES (84) Designated Contracting States: • GUCHARDI ET AL: "Influence of fine lactose and AL AT BE BG CH CY CZ DE DK EE ES FI FR GB magnesium stearate on low dose dry powder GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO inhaler formulations", INTERNATIONAL PL PT RO RS SE SI SK SM TR JOURNAL OF PHARMACEUTICS, ELSEVIER BV, NL LNKD- DOI:10.1016/J.IJPHARM.2007.06.041, (30) Priority: 21.04.2010 EP 10160565 vol. 348, no. 1-2, 19 December 2007 (2007-12-19), pages 10-17, XP022393884, ISSN: 0378-5173 (43) Date of publication of application: • ELAJNAF A ET AL: "Electrostatic 27.02.2013 Bulletin 2013/09 characterisation of inhaled powders: Effect of contact surface and relative humidity", (73) Proprietor: Chiesi Farmaceutici S.p.A. EUROPEAN JOURNAL OF PHARMACEUTICAL 43100 Parma (IT) SCIENCES, ELSEVIER, AMSTERDAM, NL LNKD- DOI:10.1016/J.EJPS.2006.07.006, vol. 29, no. 5, 1 (72) Inventors: December 2006 (2006-12-01), pages 375-384, • COCCONI, Daniela XP025137181, ISSN: 0928-0987 [retrieved on I-43100 Parma (IT) 2006-12-01] • MUSA, Rossella • CHAN ET AL: "Dry powder aerosol drug I-43100 Parma (IT) delivery-Opportunities for colloid and surface scientists", COLLOIDS AND SURFACES. -

That Had Torte I Una Altra Manian Literatura
THAT HAD TORTE I USUNA 20180016601A1ALTRA MANIAN LITERATURA UNA ( 19) United States (12 ) Patent Application Publication ( 10) Pub . No. : US 2018 / 0016601 A1 Qi et al. ( 43 ) Pub . Date: Jan . 18 , 2018 ( 54 ) METHODS FOR MODULATING GENOME C12N 15 / 10 (2006 .01 ) EDITING A6IK 38 / 46 ( 2006 .01 ) A61K 31 /365 (2006 .01 ) ( 71) Applicants: The Board of Trustees of the Leland A61K 31/ 63 ( 2006 .01 ) Stanford Junior University , Palo Alto , A61K 31 /513 ( 2006 . 01 ) CA (US ) ; The J . David Gladstone A61K 31 /505 ( 2006 .01 ) Institutes , a Testamentary Trust C12Q 1 / 68 ( 2006 .01 ) established under the Will of J . David C12N 9 / 22 ( 2006 . 01 ) Glads, San Francisco , CA ( US) ; The (52 ) U . S . CI. Regents of the University of CPC . .. - . C12N 15/ 907 ( 2013 .01 ) ; C12Q 1 /68 California , Oakland , CA (US ) ( 2013 . 01 ) ; C12Q 1 /44 ( 2013 .01 ) ; C12N 15 / 1024 (2013 .01 ) ; C12N 9 /22 ( 2013. 01 ) ; ( 72 ) Inventors : Lei S . Qi, Palo Alto , CA (US ) ; Sheng A61K 31/ 365 ( 2013 . 01) ; A61K 31 /63 Ding , Orinda , CA ( US ) ; Chen Yu , San ( 2013 .01 ) ; A61K 31/ 513 ( 2013 . 01 ) ; A61K Francisco , CA (US ) 31/ 505 ( 2013. 01 ) ; A61K 38 /465 (2013 . 01 ) (57 ) ABSTRACT ( 21 ) Appl. No. : 15 / 649, 304 Provided herein are methods and kits for modulating (22 ) Filed : Jul. 13 , 2017 genome editing of target DNA . The invention includes using small molecules that enhance or repress homology - directed Related U . S . Application Data repair (HDR ) and / or nonhomologous end joining (NHEJ ) (63 ) Continuation of application No . PCT /US2016 / repair of double - strand breaks in a target DNA sequence . -

The Use of Stems in the Selection of International Nonproprietary Names (INN) for Pharmaceutical Substances
WHO/PSM/QSM/2006.3 The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances 2006 Programme on International Nonproprietary Names (INN) Quality Assurance and Safety: Medicines Medicines Policy and Standards The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 © World Health Organization 2006 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. -

Pharmacology and Therapeutics of Bronchodilators
1521-0081/12/6403-450–504$25.00 PHARMACOLOGICAL REVIEWS Vol. 64, No. 3 Copyright © 2012 by The American Society for Pharmacology and Experimental Therapeutics 4580/3762238 Pharmacol Rev 64:450–504, 2012 ASSOCIATE EDITOR: DAVID R. SIBLEY Pharmacology and Therapeutics of Bronchodilators Mario Cazzola, Clive P. Page, Luigino Calzetta, and M. Gabriella Matera Department of Internal Medicine, Unit of Respiratory Clinical Pharmacology, University of Rome ‘Tor Vergata,’ Rome, Italy (M.C., L.C.); Department of Pulmonary Rehabilitation, San Raffaele Pisana Hospital, Istituto di Ricovero e Cura a Carattere Scientifico, Rome, Italy (M.C., L.C.); Sackler Institute of Pulmonary Pharmacology, Institute of Pharmaceutical Science, King’s College London, London, UK (C.P.P., L.C.); and Department of Experimental Medicine, Unit of Pharmacology, Second University of Naples, Naples, Italy (M.G.M.) Abstract............................................................................... 451 I. Introduction: the physiological rationale for using bronchodilators .......................... 452 II. -Adrenergic receptor agonists .......................................................... 455 A. A history of the development of -adrenergic receptor agonists: from nonselective  Downloaded from adrenergic receptor agonists to 2-adrenergic receptor-selective drugs.................... 455  B. Short-acting 2-adrenergic receptor agonists........................................... 457 1. Albuterol........................................................................ 457 -

(12) Patent Application Publication (10) Pub. No.: US 2009/0047336A1 Yang Et Al
US 20090047336A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2009/0047336A1 Yang et al. (43) Pub. Date: Feb. 19, 2009 (54) NOVEL FORMULATION OF DEHYDRATED Publication Classification LPID VESICLES FOR CONTROLLED (51) Int. Cl. RELEASE OF ACTIVE PHARMACEUTICAL A63/37 (2006.01) INGREDIENT VLANHALATION A6II 47/06 (2006.01) A 6LX 9/27 (2006.01) (75) Inventors: Zhijun Yang, Kowloon (CN); A6IR 9/14 (2006.01) Wenhua Huang, Kowloon (CN); A6IP II/00 (2006.01) Chi Sun Wong, Hong Kong (CN); A6IP II/06 (2006.01) Zhongzhen Zhao, Kowloon (CN) (52) U.S. Cl. .......... 424/450; 424/489: 514/653: 514/772 Correspondence Address: (57) ABSTRACT LEYDIG VOIT & MAYER, LTD A new formulation of dehydrated lipid vesicles employs a 700 THIRTEENTH ST. NW, SUITE 300 vesicle preserver and permits the control of release and deliv WASHINGTON, DC 20005-3960 (US) ery of active pharmaceutical ingredients into the respiratory system for treatment in particular of asthma. The typical (73) Assignee: HONG KONG BAPTIST formulation provides controlled release of the active pharma UNIVERSITY, Kowloon (CN) ceutical ingredient from 0% to 100% from 0 to 72 hours after inhalation, changes the systemic administration to topical (21) Appl. No.: 11/840,537 administration, allows prolonged therapeutic period for one administration, increased stability, with reduced dose, (22) Filed: Aug. 17, 2007 reduced systemic side effects, reduced toxicity. S Patent Application Publication US 2009/0047336A1 60 T. 50 40 30 20 O O Time (hours) --DOPC+1% gly cerin w8m DOTAP+1% glycerin FIG. 2 US 2009/0047336A1 Feb. 19, 2009 NOVEL FORMULATION OF DEHYDRATED blood pressure. -
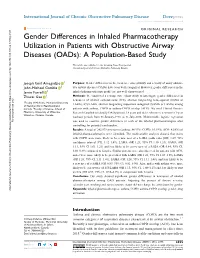
Gender Differences in Inhaled Pharmacotherapy Utilization in Patients with Obstructive Airway Diseases (Oads): a Population-Based Study
International Journal of Chronic Obstructive Pulmonary Disease Dovepress open access to scientific and medical research Open Access Full Text Article ORIGINAL RESEARCH Gender Differences in Inhaled Pharmacotherapy Utilization in Patients with Obstructive Airway Diseases (OADs): A Population-Based Study This article was published in the following Dove Press journal: International Journal of Chronic Obstructive Pulmonary Disease Joseph Emil Amegadzie 1 Purpose: Gender differences in the incidence, susceptibility and severity of many obstruc John-Michael Gamble 2 tive airway diseases (OADs) have been well recognized. However, gender differences in the Jamie Farrell 1 inhaled pharmacotherapy profile are not well characterized. Zhiwei Gao 1 Methods: We conducted a retrospective cohort study to investigate gender differences in new-users of inhaled corticosteroids (ICS), short-or long-acting beta2-agonist (SABA or 1 Faculty of Medicine, Memorial University LABA), ICS/LABA, short-or long-acting muscarinic antagonist (SAMA or LAMA) among of Newfoundland, Newfoundland, Canada; 2Faculty of Science, School of patients with asthma, COPD or asthma-COPD overlap (ACO). We used Clinical Practice Pharmacy, University of Waterloo, Research Datalink to identify OAD patients, 18 years and older, who were new-users (1-year Waterloo, Ontario, Canada washout period) from 01-January-1998 to 31-July-2018. Multivariable logistic regression For personal use only. was used to examine gender differences in each of the inhaled pharmacotherapies after controlling for potential confounders. Results: A total of 242,079 new-users (asthma: 84.93%; COPD: 10.19%; ACO: 4.88%) of inhaled pharmacotherapies were identified. The multivariable analyses showed that males with COPD were more likely to be a new user of a LABA (odds ratio [OR] 1.29; 95% confidence interval [CI], 1.12–1.49), LAMA (OR 1.21; 95% CI 1.10–1.33), SAMA (OR 1.11; 95% CI 1.01–1.21) and less likely to be a new user of a SABA (OR 0.84; 95% CI, 0.80–0.89) compared to females. -

Short-Acting Inhaled B2-Agonists: Why, Whom, What, How?
REVIEW Andrzej Emeryk1, Justyna Emeryk-Maksymiuk2 1Department of Pediatric Pulmonology and Rheumatology Medical University in Lublin, Poland 2Chair of Internal Medicine and Department of Internal Medicine in Nursing Medical University in Lublin, Poland Short-acting inhaled b2-agonists: why, whom, what, how? Abstract We showed the present data about the efficacy and safety of inhaled short-acting b2-agonists (SABA), such as salbutamol and fenoterol, in the management of obstructive diseases in children and adults. Our work discusses major mechanisms of action, clinical effects, possible side effects and indications of inhaled SABA. We presented current recommendations for the position of SABA in the therapy of obstructive diseases in children and adults, particularly in asthma and chronic obstructive pulmonary disease. Key words: short-acting b2-agonist, salbutamol, fenoterol, inhalation, nebulization, asthma, COPD Adv Respir Med. 2020; 88: 443–449 Introduction after administration of inhaled salbutamol, but the duration of action does not exceed 4–6 hours Short-acting b2-agonists (SABA) stimulate (Figure 1) [8]. b2-adrenergic receptor (b2-AR). They are called Drugs from this group provide effective b2-mimetics or b2-agonists. First selective SABA protection against exercise-induced bronchoc- widely used in clinical practice appeared more onstriction within 0.5–2.0 hours also against than 50 years ago. They were introduced to the bronchoconstriction triggered by exposure to global market in the following order: terbutaline sensitizing allergen [9, 10]. Clinical studies show (1966 yr.), salbutamol (1968 yr.) and fenoterol more potent bronchodilation and less side effects (1970 yr.) [1]. Next drugs, such as levalbuterol, of R-salbutamol in comparison with racemic sal- reproterol, rimiterol, klenbuterol and pirbuterol, butamol [11–13]. -

Comtan, INN-Entacapone
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Comtan 200 mg film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 200 mg entacapone. Excipients: Sucrose: 1.82 mg per tablet. For a full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Film-coated tablet Brownish-orange, oval, biconvex film-coated tablet with “Comtan” engraved on one side. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Entacapone is indicated as an adjunct to standard preparations of levodopa/benserazide or levodopa/carbidopa for use in patients with Parkinson’s disease and end-of-dose motor fluctuations, who cannot be stabilised on those combinations. 4.2 Posology and method of administration Entacapone should only be used in combination with levodopa/benserazide or levodopa/carbidopa. The prescribing information for these levodopa preparations is applicable to their concomitant use with entacapone. Posology One 200 mg tablet is taken with each levodopa/dopa decarboxylase inhibitor dose. The maximum recommended dose is 200 mg ten times daily, i.e. 2,000 mg of entacapone. Entacapone enhances the effects of levodopa. Hence, to reduce levodopa-related dopaminergic adverse reactions e.g. dyskinesias, nausea, vomiting and hallucinations, it is often necessary to adjust levodopa dosage within the first days to first weeks after initiating entacapone treatment. The daily dose of levodopa should be reduced by about 10–30% by extending the dosing intervals and/or by reducing the amount of levodopa per dose, according to the clinical condition of the patient. If entacapone treatment is discontinued, it is necessary to adjust the dosing of other antiparkinsonian treatments, especially levodopa, to achieve a sufficient level of control of the parkinsonian symptoms. -

Supplementary Material A: RECORD Statement
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Open Supplementary Material A: RECORD Statement The RECORD statement – checklist of items, extended from the STROBE statement, that should be reported in observational studies using routinely collected health data. Item STROBE items Location in RECORD items Location in manuscript where No. manuscript where items are reported items are reported Title and abstract 1 (a) Indicate the Page 1 in title and RECORD 1.1: The type of data 1.1 Page 1 in the abstract. study’s design with abstract used should be specified in the a commonly used title or abstract. When possible, term in the title or the name of the databases used the abstract (b) should be included. Provide in the 1.2 Page 1 in the abstract. abstract an RECORD 1.2: If applicable, informative and the geographic region and balanced summary timeframe within which the of what was done study took place should be and what was found reported in the title or abstract. 1.3 Page 1 – data were linked in a system wide dataset. RECORD 1.3: If linkage between databases was conducted for the study, this should be clearly stated in the title or abstract. Introduction Background 2 Explain the Page 3 under rationale scientific Introduction background and rationale for the investigation being reported Objectives 3 State specific Page 3 at the bottom objectives, including of the page. any prespecified hypotheses Methods Study Design 4 Present key elements Page 4 under 2.1 Data, of study design early application and in the paper setting. -

Stembook 2018.Pdf
The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. -

A Abacavir Abacavirum Abakaviiri Abagovomab Abagovomabum
A abacavir abacavirum abakaviiri abagovomab abagovomabum abagovomabi abamectin abamectinum abamektiini abametapir abametapirum abametapiiri abanoquil abanoquilum abanokiili abaperidone abaperidonum abaperidoni abarelix abarelixum abareliksi abatacept abataceptum abatasepti abciximab abciximabum absiksimabi abecarnil abecarnilum abekarniili abediterol abediterolum abediteroli abetimus abetimusum abetimuusi abexinostat abexinostatum abeksinostaatti abicipar pegol abiciparum pegolum abisipaaripegoli abiraterone abirateronum abirateroni abitesartan abitesartanum abitesartaani ablukast ablukastum ablukasti abrilumab abrilumabum abrilumabi abrineurin abrineurinum abrineuriini abunidazol abunidazolum abunidatsoli acadesine acadesinum akadesiini acamprosate acamprosatum akamprosaatti acarbose acarbosum akarboosi acebrochol acebrocholum asebrokoli aceburic acid acidum aceburicum asebuurihappo acebutolol acebutololum asebutololi acecainide acecainidum asekainidi acecarbromal acecarbromalum asekarbromaali aceclidine aceclidinum aseklidiini aceclofenac aceclofenacum aseklofenaakki acedapsone acedapsonum asedapsoni acediasulfone sodium acediasulfonum natricum asediasulfoninatrium acefluranol acefluranolum asefluranoli acefurtiamine acefurtiaminum asefurtiamiini acefylline clofibrol acefyllinum clofibrolum asefylliiniklofibroli acefylline piperazine acefyllinum piperazinum asefylliinipiperatsiini aceglatone aceglatonum aseglatoni aceglutamide aceglutamidum aseglutamidi acemannan acemannanum asemannaani acemetacin acemetacinum asemetasiini aceneuramic -
Study Protocol and Statistical Analysis Plan
ABCD TITLE PAGE Protocol for observational studies based on existing data Document Number: c02330001-03 BI Study Number: 1222.54 BI Investigational Olodaterol Product(s): Title: Cohort study of cardiovascular events in patients with chronic obstructive pulmonary disease initiating olodaterol or other long- acting beta2-agonists Protocol version 3.0 identifier: Date of last version of 14 Oct 2014 protocol: PASS: Yes EU PASS register Study not registered number: Active substance: Olodaterol Medicinal product: Striverdi, Respimat Product reference: BI 1744 Procedure number: Not applicable Marketing authorisation holder(s): Joint PASS: No Date: 28 October 2016 Page 1 of 69 Proprietary confidential information © 2016 Boehringer Ingelheim International GmbH or one or more of its affiliated companies. All rights reserved. This document may not - in full or in part - be passed on, reproduced, published or otherwise used without prior written permission Boehringer Ingelheim Page 2 of 69 Protocol for observational studies based on existing data BI Study Number 1222.54 c02330001-03 Proprietary confidential information © 2016 Boehringer Ingelheim International GmbH or one or more of its affiliated companies Additional Information Research question and Examine the risk of selected cardiac arrhythmias in patients objectives: with chronic obstructive pulmonary disease (COPD) exposed to olodaterol compared with the risk in patients exposed to other long-acting beta2-agonists (LABAs) Examine the risk of acute myocardial infarction (AMI) and other serious