Supplementary Material
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

View a Copy of This Licence, Visit Tivecommons.Org/Licenses/By/4.0
Katakami et al. Cardiovasc Diabetol (2020) 19:110 https://doi.org/10.1186/s12933-020-01079-4 Cardiovascular Diabetology ORIGINAL INVESTIGATION Open Access Tofoglifozin does not delay progression of carotid atherosclerosis in patients with type 2 diabetes: a prospective, randomized, open-label, parallel-group comparative study Naoto Katakami1,2* , Tomoya Mita3, Hidenori Yoshii4, Toshihiko Shiraiwa5, Tetsuyuki Yasuda6, Yosuke Okada7, Keiichi Torimoto7, Yutaka Umayahara8, Hideaki Kaneto9, Takeshi Osonoi10, Tsunehiko Yamamoto11, Nobuichi Kuribayashi12, Kazuhisa Maeda13, Hiroki Yokoyama14, Keisuke Kosugi15, Kentaro Ohtoshi16, Isao Hayashi17, Satoru Sumitani18, Mamiko Tsugawa19, Kayoko Ryomoto20, Hideki Taki21, Tadashi Nakamura22, Satoshi Kawashima23, Yasunori Sato24, Hirotaka Watada3 and Iichiro Shimomura1 on behalf of the UTOPIA study investigators Abstract Background: This study aimed to investigate the preventive efects of tofoglifozin, a selective sodium-glucose cotransporter 2 (SGLT2) inhibitor, on atherosclerosis progression in type 2 diabetes (T2DM) patients without apparent cardiovascular disease (CVD) by monitoring carotid intima-media thickness (IMT). Methods: This prospective, randomized, open-label, blinded-endpoint, multicenter, parallel-group, comparative study included 340 subjects with T2DM and no history of apparent CVD recruited at 24 clinical units. Subjects were randomly allocated to either the tofoglifozin treatment group (n 169) or conventional treatment group using drugs other than SGLT2 inhibitors (n 171). Primary outcomes were changes= in mean and maximum common carotid IMT measured by echography during= a 104-week treatment period. Results: In a mixed-efects model for repeated measures, the mean IMT of the common carotid artery (mean- IMT-CCA), along with the right and left maximum IMT of the CCA (max-IMT-CCA), signifcantly declined in both the tofoglifozin ( 0.132 mm, SE 0.007; 0.163 mm, SE 0.013; 0.170 mm, SE 0.020, respectively) and the control group ( 0.140 mm,− SE 0.006; 0.190 mm,− SE 0.012; 0.190 mm,− SE 0.020, respectively). -

Dapagliflozin – Structure, Synthesis, and New Indications
Pharmacia 68(3): 591–596 DOI 10.3897/pharmacia.68.e70626 Review Article Dapagliflozin – structure, synthesis, and new indications Stefan Balkanski1 1 Bulgarian Pharmaceutical Union, Sofia, Bulgaria Corresponding author: Stefan Balkanski ([email protected]) Received 24 June 2021 ♦ Accepted 4 July 2021 ♦ Published 4 August 2021 Citation: Balkanski S (2021) Dapagliflozin – structure, synthesis, and new indications. Pharmacia 68(3): 591–596.https://doi. org/10.3897/pharmacia.68.e70626 Abstract Dapagliflozin is a sodium-glucose co-transporter-2 (SGLT2) inhibitors used in the treatment of patients with type 2 diabetes. An aryl glycoside with significant effect as glucose-lowering agents, Dapagliflozin also has indication for patients with Heart Failure and Chronic Kidney Disease. This review examines the structure, synthesis, analysis, structure activity relationship and uses of the prod- uct. The studies behind this drug have opened the doors for the new line of treatment – a drug that reduces blood glucoses, decreases the rate of heart failures, and has a positive effect on patients with chronic kidney disease. Keywords Dapagliflozin, SGLT2-inhibitor, diabetes, heart failure Structure of dapagliflozin against diabetes (Lee et al. 2005; Lemaire 2012; Mironova et al. 2017). Embodiments of (SGLT-2) inhibitors include C-glycosides have a remarkable rank in medicinal chemis- dapagliflozin, canagliflozin, empagliflozin and ipragliflozin, try as they are considered as universal natural products shown in Figure 1. It has molecular formula of C24H35ClO9. (Qinpei and Simon 2004). Selective sodium-dependent IUPAC name (2S,3R,4R,5S,6R)-2-[4-chloro-3-[(4- glucose cotransporter 2 (SGLT-2) inhibitors are potent ethoxyphenyl)methyl]phenyl]-6-(hydroxymethyl)oxa- medicinal candidates of aryl glycosides that are functional ne-3,4,5-triol;(2S)-propane-1,2-diol;hydrate. -

Glucose Cotransporter 2 Inhibitor, Attenuates Body Weight Gain and Fat Accumulation in Diabetic and Obese Animal Models
OPEN Citation: Nutrition & Diabetes (2014) 4, e125; doi:10.1038/nutd.2014.20 & 2014 Macmillan Publishers Limited All rights reserved 2044-4052/14 www.nature.com/nutd ORIGINAL ARTICLE Tofogliflozin, a sodium/glucose cotransporter 2 inhibitor, attenuates body weight gain and fat accumulation in diabetic and obese animal models M Suzuki1, M Takeda1, A Kito1, M Fukazawa1, T Yata2, M Yamamoto1, T Nagata1, T Fukuzawa1, M Yamane1, K Honda1, Y Suzuki1 and Y Kawabe1 OBJECTIVE: Tofogliflozin, a highly selective inhibitor of sodium/glucose cotransporter 2 (SGLT2), induces urinary glucose excretion (UGE), improves hyperglycemia and reduces body weight in patients with Type 2 diabetes (T2D). The mechanisms of tofogliflozin on body weight reduction were investigated in detail with obese and diabetic animal models. METHODS: Diet-induced obese (DIO) rats and KKAy mice (a mouse model of diabetes with obesity) were fed diets containing tofogliflozin. Body weight, body composition, biochemical parameters and metabolic parameters were evaluated. RESULTS: In DIO rats tofogliflozin was administered for 9 weeks, UGE was induced and body weight gain was attenuated. Body fat mass decreased without significant change in bone mass or lean body mass. Food consumption (FC) increased without change in energy expenditure, and deduced total calorie balance (deduced total calorie balance ¼ FC À UGE À energy expenditure) decreased. Respiratory quotient (RQ) and plasma triglyceride (TG) level decreased, and plasma total ketone body (TKB) level increased. Moreover, plasma leptin level, adipocyte cell size and proportion of CD68-positive cells in mesenteric adipose tissue decreased. In KKAy mice, tofogliflozin was administered for 3 or 5 weeks, plasma glucose level and body weight gain decreased together with a reduction in liver weight and TG content without a reduction in body water content. -

International Journal of Pharmacy & Life Sciences
Research Article Nizami et al., 9(7): July, 2018:5860-5865] CODEN (USA): IJPLCP ISSN: 0976-7126 INTERNATIONAL JOURNAL OF PHARMACY & LIFE SCIENCES (Int. J. of Pharm. Life Sci.) Analytical method development and validation for simultaneous estimation of Ipragliflozin and Sitagliptin in tablet form by RP-HPLC method Tahir Nizami*, Birendra Shrivastava and Pankaj Sharma School of Pharmaceutical Sciences, Jaipur National University, Jagatpura, Jaipur, (RJ) - India Abstract An economical RP-HPLC method using a PDA detector at 224 nm wavelength for simultaneous estimation of Ipragliflozin and Sitagliptin in pharmaceutical dosage forms has been developed. The method was validated as per ICH guidelines over a range of 50-150 µg/mL for Ipragliflozin and Sitagliptin respectively. Analytical column used was ACE Column C18, (150 mm x 4.6 mm i.d, 5μm) with flow rate of 1.0 mL / min at a temperature of 30°C ± 0.5°C. The separation was carried out using a mobile phase consisting of orthophosphoric acid buffer and methanol in the ratio of 60: 40%v/v. Retention times of 3.092 and 4.549 min were obtained for Ipragliflozin and Sitagliptin respectively. The percentage recoveries of Ipragliflozin and Sitagliptin are 100.12% and 99.42% respectively. The goodness of fit was close to 1 for all the three components. The relative standard deviations are always less than 2%. Keywords: Ipragliflozin and Sitagliptin, RP -HPLC, Simultaneous analysis, Tablets Introduction Ipragliflozin (IPRA) a novel SGLT2 selective The empirical formulaC16H15F6N5O and the inhibitor was investigated. In vitro, the potency of molecular mass 523.32. Sitagliptin is an orally-active Ipragliflozin to inhibit SGLT2 and SGLT1 and inhibitor of the dipeptidyl peptidase-4 (DPP-4) stability were assessed. -

Comparison of Tofogliflozin 20 Mg and Ipragliflozin 50 Mg Used Together
2017, 64 (10), 995-1005 Original Comparison of tofogliflozin 20 mg and ipragliflozin 50 mg used together with insulin glargine 300 U/mL using continuous glucose monitoring (CGM): A randomized crossover study Soichi Takeishi, Hiroki Tsuboi and Shodo Takekoshi Department of Diabetes, General Inuyama Chuo Hospital, Inuyama 484-8511, Japan Abstract. To investigate whether sodium glucose co-transporter 2 inhibitors (SGLT2i), tofogliflozin or ipragliflozin, achieve optimal glycemic variability, when used together with insulin glargine 300 U/mL (Glargine 300). Thirty patients with type 2 diabetes were randomly allocated to 2 groups. For the first group: After admission, tofogliflozin 20 mg was administered; Fasting plasma glucose (FPG) levels were titrated using an algorithm and stabilized at 80 mg/dL level with Glargine 300 for 5 days; Next, glucose levels were continuously monitored for 2 days using continuous glucose monitoring (CGM); Tofogliflozin was then washed out over 5 days; Subsequently, ipragliflozin 50 mg was administered; FPG levels were titrated using the same algorithm and stabilized at 80 mg/dL level with Glargine 300 for 5 days; Next, glucose levels were continuously monitored for 2 days using CGM. For the second group, ipragliflozin was administered prior to tofogliflozin, and the same regimen was maintained. Glargine 300 and SGLT2i were administered at 8:00 AM. Data collected on the second day of measurement (mean amplitude of glycemic excursion [MAGE], average daily risk range [ADRR]; on all days of measurement) were analyzed. Area over the glucose curve (<70 mg/dL; 0:00 to 6:00, 24-h), M value, standard deviation, MAGE, ADRR, and mean glucose levels (24-h, 8:00 to 24:00) were significantly lower in patients on tofogliflozin than in those on ipragliflozin. -

202293Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 202293Orig1s000 RISK ASSESSMENT and RISK MITIGATION REVIEW(S) Department of Health and Human Services Public Health Service Food and Drug Administration Center for Drug Evaluation and Research Office of Surveillance and Epidemiology Office of Medication Error Prevention and Risk Management Final Risk Evaluation and Mitigation Strategy (REMS) Review Date: December 20, 2013 Reviewer(s): Amarilys Vega, M.D., M.P.H, Medical Officer Division of Risk Management (DRISK) Team Leader: Cynthia LaCivita, Pharm.D., Team Leader DRISK Drug Name(s): Dapagliflozin Therapeutic Class: Antihyperglycemic, SGLT2 Inhibitor Dosage and Route: 5 mg or 10 mg, oral tablet Application Type/Number: NDA 202293 Submission Number: Original, July 11, 2013; Sequence Number 0095 Applicant/sponsor: Bristol-Myers Squibb and AstraZeneca OSE RCM #: 2013-1639 and 2013-1637 *** This document contains proprietary and confidential information that should not be released to the public. *** Reference ID: 3426343 1 INTRODUCTION This review documents DRISK’s evaluation of the need for a risk evaluation and mitigation strategy (REMS) for dapagliflozin (NDA 202293). The proposed proprietary name is Forxiga. Bristol-Myers Squibb and AstraZeneca (BMS/AZ) are seeking approval for dapagliflozin as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus (T2DM). Bristol-Myers Squibb and AstraZeneca did not submit a REMS or risk management plan (RMP) with this application. At the time this review was completed, FDA’s review of this application was still ongoing. 1.1 BACKGROUND Dapagliflozin. Dapagliflozin is a potent, selective, and reversible inhibitor of the human renal sodium glucose cotransporter 2 (SGLT2), the major transporter responsible for renal glucose reabsorption. -

Open-Label Study to Assess the Efficacy of Ipragliflozin for Reducing
Clinical Drug Investigation (2019) 39:1213–1221 https://doi.org/10.1007/s40261-019-00851-z ORIGINAL RESEARCH ARTICLE Open‑Label Study to Assess the Efcacy of Ipraglifozin for Reducing Insulin Dose in Patients with Type 2 Diabetes Mellitus Receiving Insulin Therapy Hisamitsu Ishihara1 · Susumu Yamaguchi2 · Toshifumi Sugitani2 · Yoshinori Kosakai2 Published online: 24 September 2019 © The Author(s) 2019 Abstract Background and Objective To avoid insulin-induced hypoglycemia and weight gain, the minimum dose of insulin should be used. In this study, therefore, we examined insulin dose reduction by ipraglifozin add-on therapy in Japanese patients with type 2 diabetes mellitus treated with long-acting basal insulin. Methods In this multicenter, open-label study, patients received one ipraglifozin 50-mg tablet once daily in combination with basal insulin for 24 weeks. The primary efcacy endpoint was the change and percent change in insulin dose from base- line to Week 24. Secondary efcacy endpoints included changes in glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), glycoalbumin, cholesterol, leptin, adiponectin, C-peptide, glucagon, body weight, and blood pressure, and number of patients achieving withdrawal of insulin at the end of treatment (EOT). Treatment-emergent adverse events (TEAEs) were evaluated for safety. Results In total, 114 patients were screened, 103 were registered, and 97 completed the study. The mean age was 59 years and 72.8% of patients were male. The mean change in insulin dose from baseline at Week 24 was − 6.6 ± 4.4 units/day (p < 0.001); the mean percent change was − 29.87%. HbA1c, FPG, glycoalbumin, glucagon levels, body weight, and blood pressure signifcantly decreased from baseline to EOT (p < 0.05). -

Populationsweite Utilisationsuntersuchung in Den Chronischen Krankheitsbildern Hypertonie, Hyperlipid¨Amieund Typ 2 Diabetes Mellitus –
Ruhr-Universit¨atBochum Prof. Dr. rer. nat. Hans J. Trampisch Dienstort: Abteilung f¨urMedizinische Informatik, Biometrie und Epidemiologie Populationsweite Utilisationsuntersuchung in den chronischen Krankheitsbildern Hypertonie, Hyperlipid¨amieund Typ 2 Diabetes Mellitus { Eine Studie des Projekts PUKO-BHD an der Medizinischen Universit¨atWien Inaugural-Dissertation zur Erlangung des Doktorgrades der Medizin einer Hohen Medizinischen Fakult¨at der Ruhr-Universit¨atBochum vorgelegt von: Lisanne M. Jandeck aus Herford 2014 Dekan: Prof. Dr. med. Albrecht Bufe Referent: Prof. Dr. rer. nat. Hans J. Trampisch Korreferent: Prof. Dr. med. J¨urgenWindeler Tag der M¨undlichen Pr¨ufung:09.02.2017 Abstract Jandeck Lisanne M. Populationsweite Utilisationsuntersuchung in den chronischen Krankheitsbildern Hypertonie, Hyperlipid¨amieund Typ 2 Diabetes Mellitus Problem: Hypertonie (HT), Hyperlipid¨amie(HL) und Typ 2 Diabetes Mellitus (DM) stellen die h¨aufigstenchronischen Erkrankungen in Osterreich¨ dar, besonders bei Uber-50j¨ahrigen.Die¨ Zielsetzung dieser Teilstudie Utilisation\ des Projekts mit " dem Titel PUKO-BHD { Pr¨avalenz, Utilisation, Kosten und Outcome bei Blut- " hochdruck, Hyperlipid¨amieund Typ 2 Diabetes Mellitus\ ist eine populationsweite epidemiologische Untersuchung zu der Utilisation von Arzneimitteln zur Behand- lung dieser Krankheiten, insbesondere in Bezug auf Mehrfachverschreibungen (dou- ble prescriptions, DP) und Verschreibungen von Kombinationen von Wirkstoffen, die (schwerwiegende) Wechselwirkungen erzeugen k¨onnen (drug-drug -

Clinical Comparison of Tofogliflozin and Empagliflozin Based on An
Obesity Medicine 14 (2019) 100088 Contents lists available at ScienceDirect Obesity Medicine journal homepage: www.elsevier.com/locate/obmed Original research Clinical comparison of tofogliflozin and empagliflozin based on an analysis of 24-h accumulated urine in Japanese patients with type 2 diabetes mellitus T ∗ Kazuo Kobayashia, , Masao Toyodab, Nobuo Hatoric a Kobayashi Clinic of Internal Medicine, Sagamihara, Japan b Division of Nephrology, Endocrinology and Metabolism, Department of Internal Medicine, Tokai University School of Medicine, Isehara, Japan c Kobayashi Hospital, Odawara, Japan ARTICLE INFO ABSTRACT Keywords: Aim: In Japan, six sodium-glucose co-transporter 2 inhibitors have been approved for use, and some agents are Tofogliflozin associated with a significant decrease in cardiovascular events. In this study, the effects of tofogliflozin and Empagliflozin empagliflozin were compared. 24-H accumulated urine Methods: Patients with type 2 diabetes mellitus who were administered tofogliflozin (n = 10) and empagliflozin Sodium-glucose co-transporter 2 inhibitor (n = 12) were extracted. The clinical parameters and 24-h accumulated urine samples before and after 48 weeks Hematocrit were analyzed with generalized linear mixed model. Results: Both groups showed significant differences in the following parameters: body weight (p < 0.0001), mean blood pressure (p = 0.006), glycated hemoglobinA1c (p < 0.0001), alanine aminotransferase (p < 0.0001), high-density lipoprotein cholesterol (p < 0.0001), homeostatic model assessment 2 (%S) (p = 0.006), volume of 24-h accumulated urine (p < 0.0001), and 24-h urine glucose excretion (p < 0.0001). The hematocrit differed significantly over the study period (p < 0.0001); however, empaglifozin had a sig- nificantly stronger effect on the hematocrit than tofoglifozin (p = 0.007). -

Assessment of the Pharmacokinetic Interaction Between the Novel DPP-4 Inhibitor Linagliptin Andasulfonylurea,Glyburide,Inhealthysubjects
Drug Metab. Pharmacokinet. 26 (2): 123129 (2011). Copyright © 2011 by the Japanese Society for the Study of Xenobiotics (JSSX) Regular Article Assessment of the Pharmacokinetic Interaction between the Novel DPP-4 Inhibitor Linagliptin andaSulfonylurea,Glyburide,inHealthySubjects Ulrike GRAEFE-MODY1,*, Peter ROSE2,ArneRING2,KerstinZANDER2, Mario IOVINO2 and Hans-Juergen WOERLE1 1Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim, Germany 2Boehringer Ingelheim Pharma GmbH & Co. KG, Biberach, Germany Full text of this paper is available at http://www.jstage.jst.go.jp/browse/dmpk Summary: The aim of this study was to investigate the effect of the dipeptidyl peptidase-4 inhibitor linagliptin on the pharmacokinetics of glyburide (a CYP2C9 and CYP3A4 substrate) and vice versa.This randomized, open-label, three-period, two-way crossover study examined the effects of co-administration of multiple oral doses of linagliptin (5 mg/day © 6 days) and single doses of glyburide (1.75 mg/day © 1day)on the relative bioavailability of either compound in healthy subjects (n = 20, age 1855 years). Coadmin- istration of glyburide did not alter the steady-state pharmacokinetics of linagliptin. Geometric mean ratios (GMRs) [90% CI] for (linagliptin + glyburide)/linagliptin AUC¸,ss and Cmax,ss were 101.7% [97.7105.8%] and 100.8% [89.0114.3%], respectively. For glyburide, there was a slight reduction in exposure of ³14% when coadministered with linagliptin (GMRs [90% CI] for (glyburide + linagliptin)/glyburide AUC0¨ and Cmax were 85.7% [79.892.1%] and 86.2% [79.693.3%], respectively). However, this was not seen as clinically relevant due to the absence of a reliable doseresponse relationship and the known large pharmacokinetic interindividual variability of glyburide. -

Combination Use of Insulin and Incretins in Type 2 Diabetes
Canadian Agency for Agence canadienne Drugs and Technologies des médicaments et des in Health technologies de la santé CADTH Optimal Use Report Volume 3, Issue 1C Combination Use of Insulin and July 2013 Incretins in Type 2 Diabetes Supporting Informed Decisions This report is prepared by the Canadian Agency for Drugs and Technologies in Health (CADTH). The report contains a comprehensive review of the existing public literature, studies, materials, and other information and documentation (collectively the “source documentation”) available to CADTH at the time of report preparation. The information in this report is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. The information in this report should not be used as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process, nor is it intended to replace professional medical advice. While CADTH has taken care in the preparation of this document to ensure that its contents are accurate, complete, and up to date as of the date of publication, CADTH does not make any guarantee to that effect. CADTH is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in the source documentation. CADTH is not responsible for any errors or omissions or injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the information in this document or in any of the source documentation. -
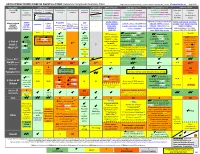
ANTI-HYPERGLYCEMIC DIABETES AGENTS in T2DM: Color Outcomes Comparison Summary Table
ANTI-HYPERGLYCEMIC DIABETES AGENTS in T2DM: Outcomes Comparison Summary Table L Regier BSP BA, M LeBras PharmD, T Trischuk PharmD, J Bareham BSP, L Lu BSP © www.RxFiles.ca Aug 2021 Drug Class Sulfonylureas TZDs Meglitinides DPP4 Inhibitors GLP1 Agonists *** SGLT2 Inhibitors *** Insulin in T2DM Generic Metformin Gliclazide Glyburide Pioglitazone Rosiglitazone Acarbose Repaglinide Saxagliptin ONGLYZA Liraglutide VICTOZA Empagliflozin JARDIANCE Intensity: Intensity: BRAND (MF) DIAMICRON DIABETA ACTOS, g AVANDIA GLUCOBAY GLUCONORM Sitagliptin JANUVIA Exenatide BYETTA, BYDUREON Canagliflozin INVOKANA Less More GLUCOPHAGE Dulaglutide TRULICITY Dapagliflozin FORXIGA, FARXIGA Alogliptin NESINA (e.g. NPH (Multiple daily GLUCOTROL D/C STEGLATRO Glipizide Nateglinide Semaglutide OZEMPIC, RYBELSUS (PO) Ertugliflozin Linagliptin TRAJENTA HS + MF) doses) STARLIX D/C SPREAD-DIMCAD] Lixisenatide ADLYXINE; ALBIGLUTIDE D/C SAVOR-TIMI 53, EMPA-REG, CANVAS, CREDENCE, T2DM: UKPDS-33,80; ADVANCE, Major trials to UKPDS- ProACTIVE ACE 33,34,80 UKPDS- Meta-analysis. TECOS, EXAMINE LEADER, EXSCEL, FREEDOM CVO, DECLARE, VERTIS-CV (2020), ACCORD, VADT, ORIGIN, DEVOTE support ADVANCE (Prevention (ADOPT; 33,80 Ferwana M. Meta- RECORD interim, PROLOGUE, REWIND, SUSTAIN-6, PIONEER-6, DAPA-HF, DAPA-CKD (2020), T1DM: DCCT/EDIC findings/ analysis 2013. trial: Stop- - some use in (ADOPT) ADOPT, DREAM CARMELINA, EMPEROR-Reduced & -Preserved (Also Boussageon et al. Meta- Outcomes* ADVANCE) SR-Liao 2017; IRIS NIDDM) ELIXA, HARMONY CAROLINA (2020), EMPA-Kidney (2022) analysis.